Download as pptx, pdf, or txt
You might also like
- Case Analysis Spina BifidaDocument11 pagesCase Analysis Spina BifidaErica Joy Algire VillalunaNo ratings yet
- Chiari MalformationDocument15 pagesChiari Malformationapi-388981686No ratings yet
- Volume Targeted VentilationDocument5 pagesVolume Targeted VentilationDiego OliveiraNo ratings yet
- Gen Path Case StudyDocument3 pagesGen Path Case Studydex7reme0% (1)
- Spina BifidaDocument26 pagesSpina BifidaZam Pamate0% (1)
- Spina BifidaDocument46 pagesSpina BifidaS G100% (1)
- Neural Tube DefectsDocument51 pagesNeural Tube DefectsSaddat kyajjaNo ratings yet
- Neural Tube DefectsDocument70 pagesNeural Tube Defectsindia2puppy100% (3)
- Neurologic DisorderDocument9 pagesNeurologic DisorderGenki Fay B. LequiganNo ratings yet
- Neema Rawat Microteaching (Spina Bifida)Document67 pagesNeema Rawat Microteaching (Spina Bifida)Dimple GoyalNo ratings yet
- Developmental Anomalies of Spinal CordDocument41 pagesDevelopmental Anomalies of Spinal Cordhamza_shoaib99No ratings yet
- Spina BifidaDocument28 pagesSpina BifidaIshita MaheyNo ratings yet
- Congenital Disorders: S. Yudha Patria Pediatrics Dept. Fac. Medicine, Gadjah Mada University, YogyakartaDocument30 pagesCongenital Disorders: S. Yudha Patria Pediatrics Dept. Fac. Medicine, Gadjah Mada University, YogyakartanadhifafirdausiNo ratings yet
- Deteksi Dini Kelainan Pada JaninDocument108 pagesDeteksi Dini Kelainan Pada JaninYuyunNo ratings yet
- Spina Bifida: by DR - Zakir Uk DPT, MSPT MSK (Kmu)Document19 pagesSpina Bifida: by DR - Zakir Uk DPT, MSPT MSK (Kmu)syge zwvuNo ratings yet
- 15.spina BifidaDocument37 pages15.spina BifidaAbdullah AzamNo ratings yet
- Spina Bifida Hydrocephalus Presentation 0Document75 pagesSpina Bifida Hydrocephalus Presentation 0Emanuel PopoviciNo ratings yet
- Spinalbifida 121213120324 Phpapp02Document28 pagesSpinalbifida 121213120324 Phpapp02Silvana María Espinoza CuadrosNo ratings yet
- Pediatric Neurologic Disorders: Ma. Tosca Cybil A. Torres, RN, MANDocument97 pagesPediatric Neurologic Disorders: Ma. Tosca Cybil A. Torres, RN, MANMa Tosca Cybil TorresNo ratings yet
- Care of A Child With Neuro Muscular DisordersDocument25 pagesCare of A Child With Neuro Muscular DisordersBilly RayNo ratings yet
- RRLDocument14 pagesRRLFreisanChenMandumotanNo ratings yet
- HYDROCEPHALUSDocument63 pagesHYDROCEPHALUSJohnsatish Rudrapogu50% (2)
- Unit 5 Child With Congenital DisordersDocument159 pagesUnit 5 Child With Congenital DisordersRenita RichardNo ratings yet
- Neural Tube DefectDocument43 pagesNeural Tube DefectEllen AngelNo ratings yet
- Central Nervous System AbnormalitiesDocument56 pagesCentral Nervous System AbnormalitiesApin PokhrelNo ratings yet
- Spina BifidaDocument9 pagesSpina BifidaOeyi Mutia SatifaNo ratings yet
- CLUBFOOT, Polydactily, Spina BividaDocument39 pagesCLUBFOOT, Polydactily, Spina BividaRobertus Dwi AtmokoNo ratings yet
- CP-1Document38 pagesCP-1Sabah shahatNo ratings yet
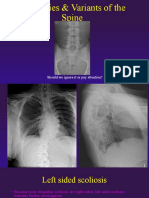
- Anomalies Variants of The SpineDocument41 pagesAnomalies Variants of The SpinekinexNo ratings yet
- Cerebral PalsyDocument38 pagesCerebral PalsyRahul KambleNo ratings yet
- 6 - Cerebral PalsyDocument52 pages6 - Cerebral PalsySaleha TariqNo ratings yet
- Cerebral Palsy (CP) : DR Raj Kumar Yadav Assist. Prof., PMR MBBS VI Sem. - 25/04/2019Document38 pagesCerebral Palsy (CP) : DR Raj Kumar Yadav Assist. Prof., PMR MBBS VI Sem. - 25/04/2019Anjali GuptaNo ratings yet
- Structural DeformitiesDocument10 pagesStructural DeformitiesChriszanie CruzNo ratings yet
- Neuro DisordersDocument159 pagesNeuro DisordersQuolette Constante100% (1)
- Discuss Surgical Management of Cerebral Palsy - 000Document72 pagesDiscuss Surgical Management of Cerebral Palsy - 000SamNo ratings yet
- HYDROCEPHALUSDocument63 pagesHYDROCEPHALUSAjeng Aristiany Rahawarin100% (2)
- Spina BifidaDocument6 pagesSpina BifidaAdiel Calsa100% (1)
- Spina BifidaDocument11 pagesSpina BifidaPauline SajoriNo ratings yet
- Ortho Zusammenfassung 2020Document258 pagesOrtho Zusammenfassung 2020Aastha SethNo ratings yet
- KennethDocument23 pagesKennethridzkhaNo ratings yet
- Meningocele & Spina BifidaDocument20 pagesMeningocele & Spina BifidaAstrid SabirinNo ratings yet
- Spina BifidaDocument6 pagesSpina BifidaFATMA BENBELGACEMNo ratings yet
- Sudden Infant Death Syndrome / Cot DeathDocument20 pagesSudden Infant Death Syndrome / Cot DeathMAHFUZ ISLAMNo ratings yet
- What Is Spina BifidaDocument18 pagesWhat Is Spina BifidaAnonymous dI1hgIJfjzNo ratings yet
- Congenital DisordersDocument56 pagesCongenital DisordersgenalinangNo ratings yet
- Spina BifidaDocument12 pagesSpina Bifidasalsabil aurellNo ratings yet
- Pediatric 222Document53 pagesPediatric 222Festo HakiNo ratings yet
- Physical DisabilitiesDocument65 pagesPhysical DisabilitiesSona CloudNo ratings yet
- Kuliah Klarif Kelainan Kongenital MayorDocument39 pagesKuliah Klarif Kelainan Kongenital MayorzulfiNo ratings yet
- Cerebral Palsy New MateryDocument95 pagesCerebral Palsy New MateryAgus WibowoNo ratings yet
- Orthopedic Congenital and Developmental Conditions in ChildhoodDocument28 pagesOrthopedic Congenital and Developmental Conditions in ChildhoodSalman KhanNo ratings yet
- Meningocele & Spina BifidaDocument21 pagesMeningocele & Spina BifidakeynechristaNo ratings yet
- Down Syndrome PDFDocument30 pagesDown Syndrome PDFAmany SaifNo ratings yet
- Cerebral PalsyDocument33 pagesCerebral PalsySaran GodcilNo ratings yet
- Abnormalities CNS: Arin SupriyadiDocument45 pagesAbnormalities CNS: Arin SupriyadiDessy AdesNo ratings yet
- Neural Tube Defects and Folic Acid: Dr. Sukma Sahreni, M.GiziDocument38 pagesNeural Tube Defects and Folic Acid: Dr. Sukma Sahreni, M.GiziGinanjar Putri SariNo ratings yet
- CP Sujit ModifiedDocument34 pagesCP Sujit ModifiedSujit KoiralaNo ratings yet
- Spina BifidaDocument2 pagesSpina BifidaMI ZINo ratings yet
- Anatomu PPT DefectsDocument87 pagesAnatomu PPT Defectsrazoon haroonNo ratings yet
- Congenital Malformations of The Nervous System PDFDocument16 pagesCongenital Malformations of The Nervous System PDFPriyanjali SainiNo ratings yet
- Common Neonatal Dysmorphic:SyndromesDocument96 pagesCommon Neonatal Dysmorphic:SyndromesMaria Babette Almazan TalaveraNo ratings yet
- Syringomyelia, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandSyringomyelia, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- TB SpineDocument18 pagesTB SpineUsaid SulaimanNo ratings yet
- Fracture Tibia & Fibula-1Document111 pagesFracture Tibia & Fibula-1Usaid SulaimanNo ratings yet
- Nutrition in The Surgical PatientDocument35 pagesNutrition in The Surgical PatientUsaid SulaimanNo ratings yet
- Radiographic Anatomy of Gastrointestinal Tract: Dr. Kikomeko Sharif Department of Radiology Iuiu-Habib Medical SchoolDocument55 pagesRadiographic Anatomy of Gastrointestinal Tract: Dr. Kikomeko Sharif Department of Radiology Iuiu-Habib Medical SchoolUsaid SulaimanNo ratings yet
- 4 Chest Imaging - Part 234Document63 pages4 Chest Imaging - Part 234Usaid SulaimanNo ratings yet
- Abdominal Imaging - Part 23Document74 pagesAbdominal Imaging - Part 23Usaid SulaimanNo ratings yet
- TB and Leprosy Case Management Desk Guide - 3rd Edition - 22!1!2019 - FINAL - SHAREDDocument78 pagesTB and Leprosy Case Management Desk Guide - 3rd Edition - 22!1!2019 - FINAL - SHAREDUsaid SulaimanNo ratings yet
- Hypertensive Emergencies: Sulaiman Usaid G. MBCHB V Facilatator: DR Jack TDocument44 pagesHypertensive Emergencies: Sulaiman Usaid G. MBCHB V Facilatator: DR Jack TUsaid SulaimanNo ratings yet
- COVID-19: Current Understanding of Its Pathophysiology, Clinical Presentation and TreatmentDocument9 pagesCOVID-19: Current Understanding of Its Pathophysiology, Clinical Presentation and TreatmentUsaid SulaimanNo ratings yet
- BURNSDocument17 pagesBURNSUsaid SulaimanNo ratings yet
- Islamic University in Uganda: Name: Abdiqani Omar NoorDocument11 pagesIslamic University in Uganda: Name: Abdiqani Omar NoorUsaid SulaimanNo ratings yet
- Islamic University in Uganda: Habib Medical SchoolDocument8 pagesIslamic University in Uganda: Habib Medical SchoolUsaid SulaimanNo ratings yet
- Psychiatry Made Easy: History Taking Technique Using Life Event ChartDocument14 pagesPsychiatry Made Easy: History Taking Technique Using Life Event ChartvelanganniNo ratings yet
- Brochure IpakitineDocument4 pagesBrochure Ipakitineyudith novida100% (1)
- Funda 9Document20 pagesFunda 9Akia Cayasan BayaNo ratings yet
- Coding Modifiers TableDocument22 pagesCoding Modifiers TableArindamDuttaChoudhury100% (1)
- Di Napoli Et Al 2020 Arterial Spin Labeling Mri in Carotid Stenosis Arterial Transit Artifacts May Predict SymptomsDocument9 pagesDi Napoli Et Al 2020 Arterial Spin Labeling Mri in Carotid Stenosis Arterial Transit Artifacts May Predict SymptomsAdenane BoussoufNo ratings yet
- Acute Respiratory SyndromeDocument10 pagesAcute Respiratory SyndromeEduardo NaranjoNo ratings yet
- Atlas of Laparoscopic Urologic Surgery, 1E (2007) PDFDocument340 pagesAtlas of Laparoscopic Urologic Surgery, 1E (2007) PDFAndreea Q. PopaNo ratings yet
- Andrea MillsDocument2 pagesAndrea MillsAndrea MillsNo ratings yet
- Ambulatory 2009Document14 pagesAmbulatory 2009Army HernandezNo ratings yet
- NURS FPX 6610 Assessment 1 Comprehensive Needs AssessmentDocument6 pagesNURS FPX 6610 Assessment 1 Comprehensive Needs AssessmentCarolyn HarkerNo ratings yet
- MictobiologyDocument26 pagesMictobiologySaransh GhimireNo ratings yet
- Toxemia in PregnancyDocument21 pagesToxemia in PregnancyRiajoy Asis100% (5)
- Approach To The Differential Diagnosis of Leg Ulcers - UpToDateDocument44 pagesApproach To The Differential Diagnosis of Leg Ulcers - UpToDatePriscillaNo ratings yet
- Daftar PustakaDocument5 pagesDaftar PustakaDesyari SusantiNo ratings yet
- MOCKBOARD PART 3 Ready To PrintDocument7 pagesMOCKBOARD PART 3 Ready To PrintJayrald CruzadaNo ratings yet
- EFN - PPTX 3Document9 pagesEFN - PPTX 3Suheni Khotimah IndrianiNo ratings yet
- PE Case StudyDocument5 pagesPE Case StudyMatt Joseph CabantingNo ratings yet
- Conscious Sedation: A Brief Overview Janette Lafroscia, Rces, Rcis, RcsDocument26 pagesConscious Sedation: A Brief Overview Janette Lafroscia, Rces, Rcis, RcsrnvisNo ratings yet
- Vulvectomy: Patient Information Patient InformationDocument11 pagesVulvectomy: Patient Information Patient InformationMega FebrianaNo ratings yet
- Psychological DisordersDocument6 pagesPsychological DisordersDiaиa DiazNo ratings yet
- Can Wearable DevicesDocument15 pagesCan Wearable DevicesJosé A. AristizabalNo ratings yet
- Haematology and Biochemistry in Alpacas and Llamas: Red Blood CellsDocument6 pagesHaematology and Biochemistry in Alpacas and Llamas: Red Blood CellsDarwin Antezana De la RosaNo ratings yet
- Charities That Do Test On AnimalsDocument6 pagesCharities That Do Test On AnimalsKaz100% (2)
- Herbal MedicineDocument5 pagesHerbal MedicineParth RathodNo ratings yet
- Drexel University College of Medicine Department of AnesthesiologyDocument1 pageDrexel University College of Medicine Department of AnesthesiologydrexelanesthesiaNo ratings yet
- JCCA Is Back-ICU Without Wall 2022 OkDocument23 pagesJCCA Is Back-ICU Without Wall 2022 OkJolatuvelBahanaNo ratings yet
- Daftar Harga Terbaru 9 September 2021 Dept. Generik: Column1 Column2 Column3 Column4Document2 pagesDaftar Harga Terbaru 9 September 2021 Dept. Generik: Column1 Column2 Column3 Column4Lia Mahdi AgustianiNo ratings yet
- Martin 2011 Quality of Life Among Caregivers ofDocument11 pagesMartin 2011 Quality of Life Among Caregivers ofjesus angel padierna aceroNo ratings yet