Download as pptx, pdf, or txt
You might also like
- TNCC Provider Manual Study GuideDocument47 pagesTNCC Provider Manual Study Guideefsf75% (8)
- Prisma Health Adult Antimicrobial Guidebook 2021Document52 pagesPrisma Health Adult Antimicrobial Guidebook 2021JhNo ratings yet
- UWorld Notes Step 2Document93 pagesUWorld Notes Step 2Vee Mend100% (1)
- EndocrinologyDocument34 pagesEndocrinologymiyuchix100% (2)
- Expanded Program For Immunization CHD ReportDocument12 pagesExpanded Program For Immunization CHD ReportCristalPagcaliwangan0% (1)
- Parathyroid Disorders I. HyperparathyroidismDocument4 pagesParathyroid Disorders I. HyperparathyroidismAllene PaderangaNo ratings yet
- RenalDocument109 pagesRenalAlejandro MarinNo ratings yet
- Hyper para Thyroid Is MDocument3 pagesHyper para Thyroid Is MAriefNo ratings yet
- Parathyrooid AnsamDocument65 pagesParathyrooid Ansamansam hirbaweNo ratings yet
- Gout and Pseudogout: Prof ZayDocument56 pagesGout and Pseudogout: Prof ZaySindhu BabuNo ratings yet
- Bone CaseDocument36 pagesBone Caseroquiyabegum1611No ratings yet
- Calcium Disorders 2Document47 pagesCalcium Disorders 2tentenNo ratings yet
- Hiperparatiroid: Dr. Dr. Shahrul Rahman, SP - PD, FINASIMDocument50 pagesHiperparatiroid: Dr. Dr. Shahrul Rahman, SP - PD, FINASIMBonitavanyNo ratings yet
- Parathyroid Gland Diseases: Classification of Diseases of PTGDocument11 pagesParathyroid Gland Diseases: Classification of Diseases of PTGgashbin latifNo ratings yet
- HiperparatiroidDocument23 pagesHiperparatiroidrahmaNo ratings yet
- Chronic Kidney Disease. GolwallaDocument8 pagesChronic Kidney Disease. GolwallaAbdul QuyyumNo ratings yet
- Bhatia Diabetes SpecialDocument24 pagesBhatia Diabetes Specialnaga tanoojNo ratings yet
- Management: DiagnosisDocument6 pagesManagement: DiagnosisAhmed El-MalkyNo ratings yet
- GoutDocument12 pagesGoutEmmanuel KafwitaNo ratings yet
- Parathyroid GlandsDocument17 pagesParathyroid GlandsMalik TamimiNo ratings yet
- Surgical Diseases of The Parathyroid GlandsDocument34 pagesSurgical Diseases of The Parathyroid Glandsanand787No ratings yet
- NCM112 HypercalcemiaDocument14 pagesNCM112 Hypercalcemiammmartinez1583No ratings yet
- Anaesthesia in Parathyroid Gland DisordersDocument25 pagesAnaesthesia in Parathyroid Gland DisordersAshiyan IrfanNo ratings yet
- Parathyroid DiseaseDocument29 pagesParathyroid DiseaseTara AzadNo ratings yet
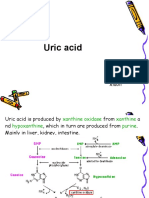
- Uric Acid: XiaoliDocument17 pagesUric Acid: XiaoliRian WibowoNo ratings yet
- IDK HiperparatiroidDocument23 pagesIDK HiperparatiroidWidya GladiantariNo ratings yet
- Disorders of Parathyroid GlandsDocument52 pagesDisorders of Parathyroid GlandsDr. Akash GuptaNo ratings yet
- Electrolyte Imbalance Where You Can See Prominent U Wave On EKGDocument5 pagesElectrolyte Imbalance Where You Can See Prominent U Wave On EKGJwaltzPadlanNo ratings yet
- Parathyroid DiseaseDocument10 pagesParathyroid Diseasemohammedghassan53No ratings yet
- Parathyroid Gland and Other Endocrine GlandsDocument35 pagesParathyroid Gland and Other Endocrine GlandsDrRahma Ali HeissNo ratings yet
- HYPOTHYRODISMDocument11 pagesHYPOTHYRODISMkamalNo ratings yet
- Hyperparathyroidism and HypoparathyroidismDocument44 pagesHyperparathyroidism and Hypoparathyroidismshweta singhNo ratings yet
- Hypercalcemia (F&e)Document3 pagesHypercalcemia (F&e)Sarah Grace CajucomNo ratings yet
- Parathyroid GlandsDocument4 pagesParathyroid GlandsMary Grace Buscargas PolancosNo ratings yet
- Laboratory Finding in Metabolic Bone Disease and AutoimuneDocument58 pagesLaboratory Finding in Metabolic Bone Disease and AutoimuneRikaNo ratings yet
- IKD3 - Uraemic Leontiassis OsseaDocument41 pagesIKD3 - Uraemic Leontiassis OsseaRenal Association MauritiusNo ratings yet
- Brown Tumor of Lower Right Limb in Patients With Primary Hyperparathyroidism: A Case ReportDocument6 pagesBrown Tumor of Lower Right Limb in Patients With Primary Hyperparathyroidism: A Case ReportMuhammad Iqbal Hermawan PutraNo ratings yet
- The Parathyroid GlandDocument66 pagesThe Parathyroid GlandMohammed GamalNo ratings yet
- Parathyroid Gland AnatomyDocument27 pagesParathyroid Gland AnatomyABUBEKER BESHIRNo ratings yet
- Acute Chronic Renal FailureDocument43 pagesAcute Chronic Renal FailureHigh Education100% (1)
- Endo 2Document114 pagesEndo 2rediet shimekachNo ratings yet
- Liver CirrhosisDocument9 pagesLiver CirrhosismedsmracelisNo ratings yet
- Metabolic Conditions Didc ClassDocument14 pagesMetabolic Conditions Didc ClassSiddique SaandNo ratings yet
- Endocrine Physiology - Part 3 Parathyroid GlandDocument30 pagesEndocrine Physiology - Part 3 Parathyroid GlandTerrence Beniasi CharumbiraNo ratings yet
- Diseases of The Adrenal GlandsDocument27 pagesDiseases of The Adrenal GlandsPurnima ChoudhuryNo ratings yet
- Parathyroid & Calcium 1Document52 pagesParathyroid & Calcium 1Mujeeb AfzalNo ratings yet
- Nephrology: Omar K MRCP IrelandDocument54 pagesNephrology: Omar K MRCP IrelandManmeet SNo ratings yet
- Gout 130718051351 Phpapp01Document47 pagesGout 130718051351 Phpapp01Manurun Londong AlloNo ratings yet
- l4 Disorders of Parathyroid GlandsDocument20 pagesl4 Disorders of Parathyroid GlandsJimmy MainaNo ratings yet
- PATH - ANAEMIA - Iron Deficiency (3p)Document3 pagesPATH - ANAEMIA - Iron Deficiency (3p)Omar HamwiNo ratings yet
- Primary HyperparathyroidismDocument13 pagesPrimary Hyperparathyroidismqayyum consultantfpscNo ratings yet
- Parathyroid & Calcitonin HormonesDocument25 pagesParathyroid & Calcitonin HormonesMuhammad Ikram MalkeraNo ratings yet
- Presentation مسنين عمليDocument19 pagesPresentation مسنين عمليzoubia209No ratings yet
- Hyperparathyroidism 170629131536Document48 pagesHyperparathyroidism 170629131536usmanNo ratings yet
- Post Your Experience See Others: Chronic Kidney Disease and Its ManagementDocument6 pagesPost Your Experience See Others: Chronic Kidney Disease and Its ManagementLuvita RonteltapNo ratings yet
- HSP WorkupDocument6 pagesHSP WorkupGiovanni SudargoNo ratings yet
- Inter'Medic AKIDocument48 pagesInter'Medic AKIMAHEJS HDNo ratings yet
- Chronic Kidney DiseaseDocument30 pagesChronic Kidney DiseaseLALITH SAI KNo ratings yet
- RadiologyDocument46 pagesRadiologyOana Nicole StoicanNo ratings yet
- Renal & Electrolyted Physiology FinalDocument21 pagesRenal & Electrolyted Physiology FinalVondNo ratings yet
- Hemochromatosis - PPTX Wk11Document19 pagesHemochromatosis - PPTX Wk11Isaac MwangiNo ratings yet
- Vitamin DDocument25 pagesVitamin DSyeda AlizaNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore Proforma For Registration of Subjects For DissertationDocument9 pagesRajiv Gandhi University of Health Sciences, Karnataka, Bangalore Proforma For Registration of Subjects For DissertationTiara Febriani NurantiNo ratings yet
- Research Ii/Sci & Tech Lab Experiment Cmshs Animal Research: Intraperitoneal InjectionDocument3 pagesResearch Ii/Sci & Tech Lab Experiment Cmshs Animal Research: Intraperitoneal InjectionPatricia Mae Rolls SantillanNo ratings yet
- Most Common Diseases of Upper ExtremitiesDocument22 pagesMost Common Diseases of Upper ExtremitiesEliazar Alumbro Peniton Jr.No ratings yet
- The Liver Flukes Clonorchis Sinensis OpisthorchisDocument17 pagesThe Liver Flukes Clonorchis Sinensis OpisthorchisDion . ANo ratings yet
- Warfarin Dosing ProtocolDocument2 pagesWarfarin Dosing Protocolkiondoon100% (1)
- A Study To Assess The Knowledge Regarding HemorrhoidsDocument26 pagesA Study To Assess The Knowledge Regarding HemorrhoidsShreyance ParakhNo ratings yet
- Clinical Profile and Demographics of Glaucoma Patients Managed in A Philippine Tertiary HospitalDocument7 pagesClinical Profile and Demographics of Glaucoma Patients Managed in A Philippine Tertiary HospitalPierre A. RodulfoNo ratings yet
- Disaster Management Action Plan: Office of The CMO District-Champawat UttarakhandDocument13 pagesDisaster Management Action Plan: Office of The CMO District-Champawat Uttarakhandpurunjay joshiNo ratings yet
- Cartilage Forming Tumors Cartilage Forming TumorsDocument53 pagesCartilage Forming Tumors Cartilage Forming TumorsFerryzal OkviandaNo ratings yet
- Hypertension: Apurva Shrestha AamppipalDocument15 pagesHypertension: Apurva Shrestha AamppipalApurvaNo ratings yet
- ID Gambaran Histologik Hati Pada Kelinci Ya PDFDocument5 pagesID Gambaran Histologik Hati Pada Kelinci Ya PDFYudha Jrokolioli NostNo ratings yet
- 1354 4486 2 PBDocument198 pages1354 4486 2 PBlinda.e.larisaNo ratings yet
- Slides For SeizureDocument15 pagesSlides For SeizureBryan Mae H. Degorio100% (3)
- Mims Jpog August 2015 IdDocument70 pagesMims Jpog August 2015 IdDika MidbrainNo ratings yet
- Mouth Throat Nose and Sinuses Checklist STUDENTSDocument4 pagesMouth Throat Nose and Sinuses Checklist STUDENTSRolandNo ratings yet
- Alprazolam XanaxDocument2 pagesAlprazolam XanaxKristi WrayNo ratings yet
- Atopic Eczema: Dr. Wistiani, Spa, Msi. MedDocument16 pagesAtopic Eczema: Dr. Wistiani, Spa, Msi. MedhwelpNo ratings yet
- Zwamborn Hanssen1997Document4 pagesZwamborn Hanssen1997JohnnyNo ratings yet
- Neurogeriatria 2017 PDFDocument417 pagesNeurogeriatria 2017 PDFWilfredo DavilaNo ratings yet
- Answer Reinforcement Bio f4 Virus - MoneraDocument13 pagesAnswer Reinforcement Bio f4 Virus - MoneranataNo ratings yet
- Ii 2015 2Document258 pagesIi 2015 2tuni santeNo ratings yet
- Resume Kevin DwyerDocument3 pagesResume Kevin Dwyerapi-317592099No ratings yet
- Byu Covid Masks AbbottDocument11 pagesByu Covid Masks AbbottAlyssa RobertsNo ratings yet
- New Vistas In: Fetal MedicineDocument2 pagesNew Vistas In: Fetal MedicineRaviraj TirukeNo ratings yet
- Pain Management Guide PDFDocument5 pagesPain Management Guide PDFPriydarshni KohliNo ratings yet
- Medical ReimbursementDocument7 pagesMedical ReimbursementHayderi GMNo ratings yet
- Under Five Clinic Visit (1) For Non CHN StudentDocument7 pagesUnder Five Clinic Visit (1) For Non CHN Studentnathsujitkr1980No ratings yet