Download as pptx, pdf, or txt
You might also like
- High Yield Surgery Shelf Exam Review CompleteDocument10 pagesHigh Yield Surgery Shelf Exam Review CompleteAmir Ali100% (1)
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Internal Medicine (Ans) - M3 Question BankDocument15 pagesInternal Medicine (Ans) - M3 Question BankWu YanlongNo ratings yet
- Cardio Notes, Heart FailureDocument17 pagesCardio Notes, Heart FailureJoy DunwanNo ratings yet
- CHFSP 2005Document36 pagesCHFSP 2005Andy F MonroeNo ratings yet
- Acquired Cardiac DisordersDocument40 pagesAcquired Cardiac DisordersRajaNo ratings yet
- Lecture 5,7-Heart FailureDocument51 pagesLecture 5,7-Heart Failurenikkonugraha_mdNo ratings yet
- Cardiac Failure: Definition: Compensatory Changes in Heart FailureDocument5 pagesCardiac Failure: Definition: Compensatory Changes in Heart FailureMatyie SmkasNo ratings yet
- Done by Jamil Mourad Supervised by Dr. Sahar ShammahDocument36 pagesDone by Jamil Mourad Supervised by Dr. Sahar ShammahJamilNo ratings yet
- Heart FailureDocument22 pagesHeart FailureYoussef MansourNo ratings yet
- Pediatric Shock: Recognition and ClassificationDocument39 pagesPediatric Shock: Recognition and ClassificationRaghavendra DoddamaniNo ratings yet
- Heart Failure: Kalaiselvan OtDocument46 pagesHeart Failure: Kalaiselvan Otplayme_nowNo ratings yet
- Heart Failure: S. Soliman MDDocument46 pagesHeart Failure: S. Soliman MDRamli HusenNo ratings yet
- Gagal JantungDocument54 pagesGagal JantungMiftahul IfahNo ratings yet
- Cardiac FailureDocument19 pagesCardiac FailureGodfrey FrancoNo ratings yet
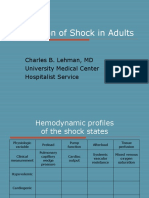
- Evaluation of Shock in AdultsDocument99 pagesEvaluation of Shock in AdultsekramsNo ratings yet
- Heart FailureDocument48 pagesHeart FailureSanjay SathasevanNo ratings yet
- Approach To Breathlessness in ETDDocument32 pagesApproach To Breathlessness in ETDprinceparisNo ratings yet
- Cardiology Notes by Wasim AhmadDocument28 pagesCardiology Notes by Wasim AhmadAshna moeenNo ratings yet
- Cor Pulmonale: Anjela BaidyaDocument31 pagesCor Pulmonale: Anjela BaidyaAnjela BaidyaNo ratings yet
- Clinical Aspect of Heart FailureDocument67 pagesClinical Aspect of Heart FailureAri Bandana TasrifNo ratings yet
- Heart NewDocument27 pagesHeart NewGomathi ShankarNo ratings yet
- Shock: Ibrahim Ali & Winfred C. ParnellDocument30 pagesShock: Ibrahim Ali & Winfred C. ParnellsgolbariNo ratings yet
- Heart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesDocument3 pagesHeart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesPrarthana Thiagarajan100% (3)
- Heart FailureDocument52 pagesHeart Failurerania salsabilaNo ratings yet
- Chinonye Ekeocha, Tazleem Khan, Ogechi Ekeocha August 23, 2010 Jackson Park Hospital Internal Medicine Core ClerkshipDocument31 pagesChinonye Ekeocha, Tazleem Khan, Ogechi Ekeocha August 23, 2010 Jackson Park Hospital Internal Medicine Core ClerkshipsgolbariNo ratings yet
- Heart Failure and ShockDocument34 pagesHeart Failure and Shockfrenee aradanasNo ratings yet
- Hypertensive Crisis: DR Putra Hedra SPPD UnibaDocument27 pagesHypertensive Crisis: DR Putra Hedra SPPD UnibaDian Puspa100% (1)
- Departemen Patologi Anatomi Fk-Usu MedanDocument25 pagesDepartemen Patologi Anatomi Fk-Usu MedanHaniv Prasetya AdhiNo ratings yet
- CCRN-PCCN-CMC Review Cardiac Part 3Document18 pagesCCRN-PCCN-CMC Review Cardiac Part 3Giovanni MictilNo ratings yet
- Vasculitis Syndrome (VS) : Dr. Julius Roma, SP ADocument45 pagesVasculitis Syndrome (VS) : Dr. Julius Roma, SP ADavid ChristianNo ratings yet
- Congestive Heart FailureDocument25 pagesCongestive Heart FailuredevianiamalinaNo ratings yet
- Rheumatic Fever and Rheumatic CarditisDocument8 pagesRheumatic Fever and Rheumatic CarditisDyanne Tan DabuNo ratings yet
- Heart Failure: DR - Liu LixinDocument46 pagesHeart Failure: DR - Liu LixinsanjivdasNo ratings yet
- Heart Failure & Cardiac Arrest: Rony YuliwansyahDocument92 pagesHeart Failure & Cardiac Arrest: Rony YuliwansyahSasha ManoNo ratings yet
- Cardiac EmergencyDocument56 pagesCardiac Emergencysuganthi rajesh kannaNo ratings yet
- Cardiogenic Shock: DR Putra Hendra SPPD UnibaDocument30 pagesCardiogenic Shock: DR Putra Hendra SPPD UnibaDian PuspaNo ratings yet
- Cardiovascular Assessment & Cardiac DisordersDocument57 pagesCardiovascular Assessment & Cardiac DisordersgtsantosNo ratings yet
- Edema Paru: DR Adyan Donastin, SPP Kuliah FK UnusaDocument52 pagesEdema Paru: DR Adyan Donastin, SPP Kuliah FK UnusaArfan AffandyNo ratings yet
- Heart Failure & Circulatory ShockDocument34 pagesHeart Failure & Circulatory ShockMuskaan ZaharaNo ratings yet
- Acute Biologic Crisis & Disaster NursingDocument80 pagesAcute Biologic Crisis & Disaster NursingprinceBel21No ratings yet
- Congestive Heart FailureDocument28 pagesCongestive Heart Failuresarguss1480% (5)
- Cardiovascular Disorders 2Document78 pagesCardiovascular Disorders 2Erlinda SagadsadNo ratings yet
- Cardiovascular Diseases: DR Raveendra K.R Assistant Professor Department of Medicine BMC BangaloreDocument34 pagesCardiovascular Diseases: DR Raveendra K.R Assistant Professor Department of Medicine BMC BangalorerameshbmcNo ratings yet
- Erythema Marginatum Chorea: Migratory Polyarthritis Cardiac Involvement Subcutaneous NodulesDocument27 pagesErythema Marginatum Chorea: Migratory Polyarthritis Cardiac Involvement Subcutaneous NodulesMisbah KaleemNo ratings yet
- Diastolic DysfunctionDocument39 pagesDiastolic Dysfunctionkaaalifa12No ratings yet
- PulseDocument43 pagesPulseAngelo LacisteNo ratings yet
- Acute Biologic Crisis-ArDocument71 pagesAcute Biologic Crisis-ArJayvee Novenario CasaljayNo ratings yet
- USMLE WORLD Medicine NotesDocument126 pagesUSMLE WORLD Medicine NotesaelteeNo ratings yet
- Systolic Dysfunction:: Types of Heart FailureDocument13 pagesSystolic Dysfunction:: Types of Heart FailureElisabeth F. OjhaNo ratings yet
- LT ShockDocument26 pagesLT ShockLong LieNo ratings yet
- 4.cardivascular System ExaminationDocument60 pages4.cardivascular System ExaminationElvisNo ratings yet
- P 3a Gagal JTGDocument35 pagesP 3a Gagal JTGAnaMariyaMaNo ratings yet
- Pulse 160311110553Document43 pagesPulse 160311110553forever studentNo ratings yet
- Nursing Management Patients W CVD Part2 Myocardial Infarction EnglishDocument43 pagesNursing Management Patients W CVD Part2 Myocardial Infarction EnglishRizka Patria SariNo ratings yet
- Acute Heart FailureDocument71 pagesAcute Heart FailureVivek Anandan100% (1)
- All in BriefDocument8 pagesAll in BriefAikoP.NarcisoNo ratings yet
- Cardiac Care and COVID-19: Perspectives in Medical PracticeFrom EverandCardiac Care and COVID-19: Perspectives in Medical PracticeNo ratings yet
- Pharmacotherapeutic Management of Cardiovascular Disease Complications: A Textbook for Medical StudentsFrom EverandPharmacotherapeutic Management of Cardiovascular Disease Complications: A Textbook for Medical StudentsNo ratings yet
- 2019 Esc PPCMDocument17 pages2019 Esc PPCMJayden WaveNo ratings yet
- SEMINARDocument31 pagesSEMINARDeveshNo ratings yet
- Nejmra 2207410Document15 pagesNejmra 2207410rindayusticia100% (1)
- Value of Epicardial Adipose Tissue Assessment by Cardiac Computerized Tomography in Heart Failure Patients With Preserved Ejection FractionDocument6 pagesValue of Epicardial Adipose Tissue Assessment by Cardiac Computerized Tomography in Heart Failure Patients With Preserved Ejection FractionIJAR JOURNALNo ratings yet
- Ateroesclerosis Kimee NeyssaDocument12 pagesAteroesclerosis Kimee NeyssaNEYSSA KIMEE SAINT VILNo ratings yet
- Printed - NCLEX Practice Exam 21Document32 pagesPrinted - NCLEX Practice Exam 21Melodia Turqueza GandezaNo ratings yet
- CSDocument74 pagesCSSimina ÎntunericNo ratings yet
- A Brief Review On The Effects of The Squat Exercise On Lower Limb Muscle HypertrophyDocument10 pagesA Brief Review On The Effects of The Squat Exercise On Lower Limb Muscle HypertrophyDaniel FreireNo ratings yet
- 2017 The Effects of Short Versus Long Inter Set Rest Intervals in Resistance Training On Measures of Muscle Hypertrophy A Systematic ReviewDocument13 pages2017 The Effects of Short Versus Long Inter Set Rest Intervals in Resistance Training On Measures of Muscle Hypertrophy A Systematic ReviewLucas EmanuelNo ratings yet
- Cardiovascular DrillsDocument12 pagesCardiovascular DrillsMaria Garcia Pimentel Vanguardia IINo ratings yet
- Pathophysiology and Etiology of Sudden Cardiac Arrest: Author: Section Editors: Deputy EditorDocument23 pagesPathophysiology and Etiology of Sudden Cardiac Arrest: Author: Section Editors: Deputy EditorAnca StanNo ratings yet
- Cardiac Myocytes CultureDocument6 pagesCardiac Myocytes CultureÉmerson MoreiraNo ratings yet
- Anabolic Androgenic SteroidsDocument70 pagesAnabolic Androgenic Steroidsfaqed ilzakira100% (2)
- High Prevalence of Subclinical Left Ventricular Dysfunction in Patients With Psoriatic ArthritisDocument8 pagesHigh Prevalence of Subclinical Left Ventricular Dysfunction in Patients With Psoriatic ArthritisEmanuel NavarreteNo ratings yet
- Cardiomyopathy: Leonard Shaju Joisy AloorDocument34 pagesCardiomyopathy: Leonard Shaju Joisy AloorJoisy AloorNo ratings yet
- Pathophysiology of Heart Failure: Prof. J. HanacekDocument48 pagesPathophysiology of Heart Failure: Prof. J. Hanaceksukarni84sgdNo ratings yet
- Chapter 35Document14 pagesChapter 35Tr-I-LifeNo ratings yet
- Scandinavian Med Sci Sports - 2022 - Angleri - Resistance Training Variable Manipulations Is Less Relevant Than IntrinsicDocument26 pagesScandinavian Med Sci Sports - 2022 - Angleri - Resistance Training Variable Manipulations Is Less Relevant Than IntrinsicDaniloNo ratings yet
- Applied Anatomy of The Heart - StudentDocument38 pagesApplied Anatomy of The Heart - StudentNatalia RomanNo ratings yet
- Hipertrofia MuscularDocument22 pagesHipertrofia MuscularNonato MendonçaNo ratings yet
- Chronic Adaptations To Training: Liveitup2Document20 pagesChronic Adaptations To Training: Liveitup2dvenumohanNo ratings yet
- Cellular Responses To Stress and Toxic Insults: Adaptation, Injury, and DeathDocument81 pagesCellular Responses To Stress and Toxic Insults: Adaptation, Injury, and DeathICE ADRIENNE OCAMPONo ratings yet
- Acc-Aha Practice GuidelineDocument12 pagesAcc-Aha Practice GuidelineShofa ShofiatunnisaNo ratings yet
- Pathology SummaryDocument30 pagesPathology SummaryFiras Anaya100% (1)
- Chapter 25 The Child With Cardiovascular DysfunctionDocument20 pagesChapter 25 The Child With Cardiovascular DysfunctionJill Hill100% (3)
- Diferentes Modos de Hipertrofia Nas Fibras Musculares Esqueléticas PDFDocument10 pagesDiferentes Modos de Hipertrofia Nas Fibras Musculares Esqueléticas PDFSheilani MartinsNo ratings yet
- Diabetic Cardiomyopathy: An Update On Its Pathophysiology With Specific Emphasis On Epigenetics Modifications Besides Treatment - A Systematic ReviewDocument16 pagesDiabetic Cardiomyopathy: An Update On Its Pathophysiology With Specific Emphasis On Epigenetics Modifications Besides Treatment - A Systematic ReviewIJRDPM JOURNALNo ratings yet
- Management of Hypertension Induced Left Ventricular Hypertrophy A Single Case StudyDocument3 pagesManagement of Hypertension Induced Left Ventricular Hypertrophy A Single Case StudyEditor IJTSRDNo ratings yet
- Vspo 1 100Document83 pagesVspo 1 100calchasNo ratings yet