Download as ppt, pdf, or txt
You might also like
- Anatomia de La RodillaDocument11 pagesAnatomia de La RodillaMilena Cardona RuizNo ratings yet
- What Is FashionDocument6 pagesWhat Is FashionArim Arim100% (3)
- Upper Limb SkeletonDocument28 pagesUpper Limb SkeletonDanaNo ratings yet
- Lec 14 THE KNEE JOINTDocument17 pagesLec 14 THE KNEE JOINTMaheen IrfanNo ratings yet
- Hap AssignmentDocument3 pagesHap AssignmentMaliha khanNo ratings yet
- Lectura Previ2 - U1-M6-T4-CAPITULO LESIONES DE PIE 2Document13 pagesLectura Previ2 - U1-M6-T4-CAPITULO LESIONES DE PIE 2Maria De Los Angeles Vitteri EdenNo ratings yet
- Knee Joint (Anatomy)Document5 pagesKnee Joint (Anatomy)Ojambo FlaviaNo ratings yet
- 6 2Document48 pages6 2wx8vnnnzjhNo ratings yet
- Assignment Shoulder JointDocument7 pagesAssignment Shoulder JointMary Grace OrozcoNo ratings yet
- Joints 1Document12 pagesJoints 1Shaik AminaNo ratings yet
- Acetabular LabrumDocument31 pagesAcetabular LabrumhaminatrafNo ratings yet
- Naik, S. - Biomechanics of Knee ComplexDocument25 pagesNaik, S. - Biomechanics of Knee ComplexKyle Bois100% (4)
- Foot and Ankle Bones and JointsDocument43 pagesFoot and Ankle Bones and Jointshannah murphyNo ratings yet
- Snell Lower LimbDocument44 pagesSnell Lower LimbBen100% (3)
- Norm Anatomy Elbow 2011Document11 pagesNorm Anatomy Elbow 2011Екатерина БербецNo ratings yet
- TMJ - Lec8Document10 pagesTMJ - Lec8A.A. HusseinNo ratings yet
- Vertebral JointDocument5 pagesVertebral Jointاحمد البزورNo ratings yet
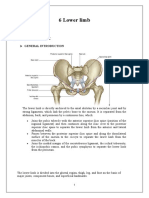
- 6 Lower LimbDocument19 pages6 Lower LimbMOHAMMED BIN BAREKNo ratings yet
- Examen FisicoDocument26 pagesExamen FisicoAmada Angel VillanuevaNo ratings yet
- Biomechanics of Cervical SpineDocument25 pagesBiomechanics of Cervical SpineNithya NithyaNo ratings yet
- Definition of Shoulder DislocationDocument66 pagesDefinition of Shoulder DislocationDeepika verma100% (1)
- Anatomy and PhysiologyDocument4 pagesAnatomy and PhysiologyAnnileighjeanNo ratings yet
- Anatomy Units 9-12 ObjectivesDocument18 pagesAnatomy Units 9-12 ObjectivespoNo ratings yet
- Anatomy, Vetebrae BonesDocument10 pagesAnatomy, Vetebrae Bonesharis13.hsNo ratings yet
- 18 MSK Arm and HandDocument27 pages18 MSK Arm and HandNTRisforthinkersNo ratings yet
- Chapter 24 - MSKDocument3 pagesChapter 24 - MSKannoja selvaNo ratings yet
- ANATOMY I 23.03.20 I The Pectoral Girdle and Upper LimbDocument25 pagesANATOMY I 23.03.20 I The Pectoral Girdle and Upper LimbArianna RomanoNo ratings yet
- Anatomy of KneeDocument47 pagesAnatomy of Kneehanuman kannaNo ratings yet
- Knee Anatomy Osseous Structures: Concept InformationDocument19 pagesKnee Anatomy Osseous Structures: Concept InformationRachel BlackburnNo ratings yet
- 1.review OsteoarthritisDocument22 pages1.review OsteoarthritisGERSON RYANTONo ratings yet
- Vertebra: StructureDocument9 pagesVertebra: StructureayudhyaNo ratings yet
- StructureDocument7 pagesStructureNeirfla WassabiNo ratings yet
- PO2 ArtrologieDocument4 pagesPO2 ArtrologieYiNo ratings yet
- Anatomy, Shoulder and Upper Limb, Shoulder MusclesDocument12 pagesAnatomy, Shoulder and Upper Limb, Shoulder MusclesluizamgoNo ratings yet
- Anatomy and Physiology of The SpineDocument12 pagesAnatomy and Physiology of The SpineKinahZildredBibitNo ratings yet
- Joints and Ligaments Anatomy TablesDocument32 pagesJoints and Ligaments Anatomy TablessmoggindakrakNo ratings yet
- ST - Paulos Hospital Millennium Medical College: Gross Anatomy:Upper LimbDocument256 pagesST - Paulos Hospital Millennium Medical College: Gross Anatomy:Upper LimbetNo ratings yet
- Radius and Ulna: PPP Jazlan Bin Mohamad (Posbasic Ortho 1/2018)Document17 pagesRadius and Ulna: PPP Jazlan Bin Mohamad (Posbasic Ortho 1/2018)Jazlan MohamadNo ratings yet
- 1 Articulating Surfaces 2 Neurovasculature 3 Menisci 4 Bursae 5 Ligaments 6 Movements 7 Clinical Relevance: Injury To The Knee JointDocument7 pages1 Articulating Surfaces 2 Neurovasculature 3 Menisci 4 Bursae 5 Ligaments 6 Movements 7 Clinical Relevance: Injury To The Knee JointHassan Mohamed100% (1)
- Anatomy and Genetics / 1Document36 pagesAnatomy and Genetics / 1Abdul Ghaffar AbdullahNo ratings yet
- 3 Functional Anatomy of The Knee: D. G. EckhoffDocument7 pages3 Functional Anatomy of The Knee: D. G. EckhoffCiberNo ratings yet
- Mandibular MovementsDocument36 pagesMandibular MovementsRagini ShravanNo ratings yet
- AD 5 Vertebral AnatomyDocument37 pagesAD 5 Vertebral AnatomyLintang ZerlinaNo ratings yet
- Solomon Ankle Injury PDFDocument9 pagesSolomon Ankle Injury PDFHikmah Wahid AkbarNo ratings yet
- ThoraxDocument54 pagesThoraxfalz0012kNo ratings yet
- 8 SkeletonDocument3 pages8 SkeletonMichelleAquinoSuzukiNo ratings yet
- Knee JointDocument18 pagesKnee Jointزيد عماد أحمدNo ratings yet
- 8 The Appendicular Skeleton: Chapter ObjectivesDocument48 pages8 The Appendicular Skeleton: Chapter ObjectivessinnueNo ratings yet
- Gross Anatomy I OsteologyDocument42 pagesGross Anatomy I OsteologySonia FelixNo ratings yet
- Anatomi AnkleDocument15 pagesAnatomi AnkleZera DirgantaraNo ratings yet
- Elbow and Antebrachium NotesDocument8 pagesElbow and Antebrachium NoteschadNo ratings yet
- Articulations of The PelvisDocument4 pagesArticulations of The PelvisSiva ShanmugamNo ratings yet
- CRANIOVETEBRALJUNCTIONDocument130 pagesCRANIOVETEBRALJUNCTIONdrarunrao100% (1)
- The Axial Skeleton - 2Document158 pagesThe Axial Skeleton - 2Zaid HamdanNo ratings yet
- Knee 05102018Document24 pagesKnee 05102018Dk KNo ratings yet
- Anatomy of The Elbow JointDocument5 pagesAnatomy of The Elbow JointRahayu EkaNo ratings yet
- BONEDocument27 pagesBONEVIJAYA KUMAR YNo ratings yet
- Upper Limb Anatomy 1Document6 pagesUpper Limb Anatomy 1shahab shamsiNo ratings yet
- Lec 18 THE ANKLE JOINTDocument12 pagesLec 18 THE ANKLE JOINTMaheen IrfanNo ratings yet
- The Axial MusclesDocument163 pagesThe Axial MusclesZaid HamdanNo ratings yet
- The Axial Skeleton - 2Document158 pagesThe Axial Skeleton - 2Zaid HamdanNo ratings yet
- NullDocument36 pagesNullZaid HamdanNo ratings yet
- Musculosk UL3 Muscles 1Document66 pagesMusculosk UL3 Muscles 1Zaid HamdanNo ratings yet
- Cardiovascular Surgery TestbankDocument16 pagesCardiovascular Surgery TestbankZaid HamdanNo ratings yet
- Musculosk UL5 Muscles 3Document94 pagesMusculosk UL5 Muscles 3Zaid HamdanNo ratings yet
- NullDocument158 pagesNullZaid HamdanNo ratings yet
- 3 - Communication SkillsDocument34 pages3 - Communication SkillsZaid HamdanNo ratings yet
- باطني خطاطبةDocument168 pagesباطني خطاطبةZaid HamdanNo ratings yet
- SWM Notes IIDocument8 pagesSWM Notes IIBeast gaming liveNo ratings yet
- Bent Mag-Dec 2009Document80 pagesBent Mag-Dec 2009EcarvalhoStad0% (3)
- Ordi 16 2014 Maternal Neonatal PublishedDocument15 pagesOrdi 16 2014 Maternal Neonatal PublishedAbraham AstoNo ratings yet
- Reblex AnswersDocument17 pagesReblex AnswersAerol Buenaventura100% (1)
- Contra About PolygamyDocument3 pagesContra About PolygamyNabil AushafaNo ratings yet
- C4 Tech Spec Issue 2Document5 pagesC4 Tech Spec Issue 2Дмитрий КалининNo ratings yet
- 11 Ultimate Protection Video Charitable Religious TrustsDocument12 pages11 Ultimate Protection Video Charitable Religious TrustsKing FishNo ratings yet
- Communication MatrixDocument1 pageCommunication Matrixrohini kadamNo ratings yet
- 08 Package Engineering Design Testing PDFDocument57 pages08 Package Engineering Design Testing PDFLake HouseNo ratings yet
- Conceptual Design of An Automotive Composite Brake Pedal: Mohd Sapuan Salit, Mohd Syed Ali Molla and MD Liakot AliDocument5 pagesConceptual Design of An Automotive Composite Brake Pedal: Mohd Sapuan Salit, Mohd Syed Ali Molla and MD Liakot Aliseran ünalNo ratings yet
- GE3 Prelim Exam1Document4 pagesGE3 Prelim Exam1Edrose WycocoNo ratings yet
- LP in MusicDocument10 pagesLP in MusicContagious Joy VillapandoNo ratings yet
- Blockchain-Enabled Drug Supply Chain: Sheetal Nayak, Prachitee Shirvale, Nihar Naik, Snehpriya Khul, Amol SawantDocument4 pagesBlockchain-Enabled Drug Supply Chain: Sheetal Nayak, Prachitee Shirvale, Nihar Naik, Snehpriya Khul, Amol SawantWaspNo ratings yet
- Brocade NetApp Product Quick Reference Guide 201905Document8 pagesBrocade NetApp Product Quick Reference Guide 201905Alex JinNo ratings yet
- FisheriesDocument31 pagesFisheriesGarima LoonaNo ratings yet
- Ivermectin TabletsDocument2 pagesIvermectin Tabletsluis diazNo ratings yet
- Metallic BondingDocument2 pagesMetallic BondingJohanna LipioNo ratings yet
- EPM-1183 Ethics, Code of Conduct & Professional PracticeDocument41 pagesEPM-1183 Ethics, Code of Conduct & Professional PracticeDev ThackerNo ratings yet
- Cemex Holdings Philippines Annual Report 2016 PDFDocument47 pagesCemex Holdings Philippines Annual Report 2016 PDFFritz NatividadNo ratings yet
- JOSE ANTONIO C. LEVISTE v. ELMO M. ALAMEDA, GR No. 182677, Aug. 03, 2010 FactsDocument2 pagesJOSE ANTONIO C. LEVISTE v. ELMO M. ALAMEDA, GR No. 182677, Aug. 03, 2010 FactsRajane Alexandra DequitoNo ratings yet
- Anatomy GuDocument13 pagesAnatomy Gujefel umarNo ratings yet
- 2011 Diving Catalogue BEUCHATDocument60 pages2011 Diving Catalogue BEUCHATRalph KramdenNo ratings yet
- Cosmetics Case ProjectDocument16 pagesCosmetics Case ProjectLaura NardiNo ratings yet
- How To Cite A Research Paper in TextDocument8 pagesHow To Cite A Research Paper in Textafnkaufhczyvbc100% (1)
- English 8-Q4-M1-Grammatical SignalsDocument12 pagesEnglish 8-Q4-M1-Grammatical SignalsShekayna PalagtiwNo ratings yet
- En 12245 (2022) (E)Document9 pagesEn 12245 (2022) (E)David Chirinos100% (1)
- CASHe Soa 568304-1Document2 pagesCASHe Soa 568304-1sathyaNo ratings yet
- Gomez V MontalbanDocument1 pageGomez V MontalbanShariefaAichaseAsaliNo ratings yet
- Lion of The North - Rules & ScenariosDocument56 pagesLion of The North - Rules & ScenariosBrant McClureNo ratings yet