Download as pptx, pdf, or txt
You might also like
- 5 Cases FungalDocument56 pages5 Cases Fungalkoteshwara raoNo ratings yet
- Edited Monkeypox Facts 2022Document93 pagesEdited Monkeypox Facts 2022anghelmiguel07262016No ratings yet
- Antibiotics10 PDFDocument19 pagesAntibiotics10 PDFDharani TharanNo ratings yet
- Antibiotics10 PDFDocument19 pagesAntibiotics10 PDFDharani TharanNo ratings yet
- Case Study: Urinary Tract InfectionDocument21 pagesCase Study: Urinary Tract InfectionRania Sh AzzehNo ratings yet
- SHC Intra Abdominal GuidelinesDocument13 pagesSHC Intra Abdominal GuidelinesNguyễn Mạnh CườngNo ratings yet
- Monkeypox Facts 2022Document88 pagesMonkeypox Facts 2022Edrheyl Limbaga BiadnesNo ratings yet
- Pprom 1 1Document20 pagesPprom 1 1Tehreem AzharNo ratings yet
- Diagnostic Virologique-2022-Pr. EzzikouriDocument52 pagesDiagnostic Virologique-2022-Pr. Ezzikourilefebi6403No ratings yet
- Management of Intra-Abdominal InfectionDocument65 pagesManagement of Intra-Abdominal InfectionKamran SherazNo ratings yet
- Drug Study NicoleDocument6 pagesDrug Study NicoleFrancheska Nicole Delos SantosNo ratings yet
- Classification: Cefditoren, As This Agent May CauseDocument3 pagesClassification: Cefditoren, As This Agent May CauseHavier EsparagueraNo ratings yet
- Pre Anaesthetic Check-UpDocument4 pagesPre Anaesthetic Check-UpUdoy PaulNo ratings yet
- Antibiotic Guidelines For Adults 2018 PDFDocument58 pagesAntibiotic Guidelines For Adults 2018 PDFAhmad RizqiNo ratings yet
- DR - PARTHA - 2018 Clinical Microbiology II PDFDocument88 pagesDR - PARTHA - 2018 Clinical Microbiology II PDFNuzki YofandaNo ratings yet
- Emerging & Remerging Parasitic DiseasesDocument27 pagesEmerging & Remerging Parasitic DiseasesNeha SamalNo ratings yet
- RabiesDocument47 pagesRabiesFrancisco Gangoso Jr.No ratings yet
- Sample Case Studies of COVID-19 in PregnancyDocument29 pagesSample Case Studies of COVID-19 in PregnancyAbdibaset Mohamed AdenNo ratings yet
- Appropriate Antimicrobial Treatment For Complicated Skin & Soft Tissue Infection (CSSTI) - PIN PABDIDocument31 pagesAppropriate Antimicrobial Treatment For Complicated Skin & Soft Tissue Infection (CSSTI) - PIN PABDIReynalth SinagaNo ratings yet
- HEPATITIS A Brief Introduction.Document45 pagesHEPATITIS A Brief Introduction.pharmaci100% (2)
- Communicable Diseases Module 1Document38 pagesCommunicable Diseases Module 1Sanidad Yani BelNo ratings yet
- C Diff SeminarDocument51 pagesC Diff SeminarVivek VijayanNo ratings yet
- Office and Laboratory ManagementDocument8 pagesOffice and Laboratory ManagementEman BayoumiNo ratings yet
- Elsie Kho Ap300 Study NotesDocument36 pagesElsie Kho Ap300 Study Noteshanazawa_rui9878030No ratings yet
- Common Laboratory Investigations in Obstetrics and GynaecologyDocument4 pagesCommon Laboratory Investigations in Obstetrics and GynaecologyIndhumathiNo ratings yet
- 2021 - l4 Medical Bacteriology - Gram Negative Bacteria (I)Document52 pages2021 - l4 Medical Bacteriology - Gram Negative Bacteria (I)Tonny YuliantoNo ratings yet
- Data Collection Pathway: ExcludeDocument1 pageData Collection Pathway: ExcludeAndy F MonroeNo ratings yet
- Urinary Tract Infections in Neonates With Unexplained Pathological Indirect Hyperbilirubinemia: Prevalence and SignificanceDocument5 pagesUrinary Tract Infections in Neonates With Unexplained Pathological Indirect Hyperbilirubinemia: Prevalence and SignificancePutri YingNo ratings yet
- Management of Neonatal SepsisDocument30 pagesManagement of Neonatal SepsisRam krishnaNo ratings yet
- Skin Soft Tissue Infections 1 - 27 - 2019Document14 pagesSkin Soft Tissue Infections 1 - 27 - 2019Muhammad Azhar ImranNo ratings yet
- NOTES - Specimen Collection, Handling & ProcessingDocument4 pagesNOTES - Specimen Collection, Handling & ProcessingOdette G. TanNo ratings yet
- Infectious Diarrhea: Ordering Stool Test For Investigation of SuspectedDocument8 pagesInfectious Diarrhea: Ordering Stool Test For Investigation of SuspectedBenny TrisaktyariNo ratings yet
- Jurnal 882Document1 pageJurnal 882saddamNo ratings yet
- C. Difficile-4Document3 pagesC. Difficile-4Suprakkash DasNo ratings yet
- Neonatal SepsisDocument7 pagesNeonatal Sepsispaningbatan.kristine.bNo ratings yet
- CHAPTER 9 ReviewerDocument4 pagesCHAPTER 9 ReviewerHannah BuquironNo ratings yet
- 2.04 Surgical Illness in PregnancyDocument6 pages2.04 Surgical Illness in PregnancyRaquel ReyesNo ratings yet
- Infectious Diarrhoea: Laboratory Investigation ofDocument36 pagesInfectious Diarrhoea: Laboratory Investigation ofputra nisaNo ratings yet
- General Characteristics of VirusesDocument3 pagesGeneral Characteristics of VirusesS. C.No ratings yet
- 10.1007@s00247 020 04656 7 PDFDocument4 pages10.1007@s00247 020 04656 7 PDFRoberto AmayaNo ratings yet
- Management of Neonatal Sepsis: Niki Kosmetatos, MD Anthony Piazza, MD J. Devn Cornish, MDDocument30 pagesManagement of Neonatal Sepsis: Niki Kosmetatos, MD Anthony Piazza, MD J. Devn Cornish, MDiniidzniNo ratings yet
- Urinary Tract Infections in ChildrenDocument6 pagesUrinary Tract Infections in ChildrenMarianNo ratings yet
- UTI - Practical ApproachDocument35 pagesUTI - Practical ApproachJustine Frances CabalayNo ratings yet
- Soal Dan Pembahasan Pretest IRDocument16 pagesSoal Dan Pembahasan Pretest IRSummer SnowNo ratings yet
- Dialysis Inovative Facility Policies and ProceduresDocument3 pagesDialysis Inovative Facility Policies and ProceduresFrancis Marven Lee LocsinNo ratings yet
- MEDF1120 Global PH EID Student v2Document32 pagesMEDF1120 Global PH EID Student v2denisemywongNo ratings yet
- Period of Communicability: ChloramphenicolDocument10 pagesPeriod of Communicability: ChloramphenicolDona Mae TaberaNo ratings yet
- Recommendations For Covid 19 PCR TestingDocument4 pagesRecommendations For Covid 19 PCR TestingDipa Zoda Helfando100% (1)
- COVID-19 MoHP Protocol May 2020Document14 pagesCOVID-19 MoHP Protocol May 2020BARAKA ROKANo ratings yet
- Elanco Parvovirus DXTX GDocument2 pagesElanco Parvovirus DXTX Gazamkhan60No ratings yet
- tpmd170465 PDFDocument5 pagestpmd170465 PDFWaradhamma MatchimaNo ratings yet
- FWBD MOP Laboratory Managementasof13Apr2023Document12 pagesFWBD MOP Laboratory Managementasof13Apr2023sharmaine peroNo ratings yet
- Febrile Neutropenia Topic DiscussionDocument42 pagesFebrile Neutropenia Topic Discussionapi-647904873No ratings yet
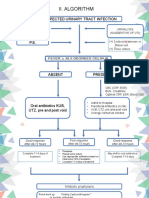
- Ii. Algorithm: Suspected Urinary Tract Infection HistoryDocument6 pagesIi. Algorithm: Suspected Urinary Tract Infection HistoryTaeyomiNo ratings yet
- Basnyat 2021Document7 pagesBasnyat 2021nathanaellee92No ratings yet
- Topic - Neutropenic Fever OutlineDocument5 pagesTopic - Neutropenic Fever Outlineapi-549451092No ratings yet
- Guía Rápida StanfordDocument6 pagesGuía Rápida StanfordDr. Victor Adolfo RochaNo ratings yet
- Vrebsc 180521172503Document16 pagesVrebsc 180521172503D. Melba S.S ChinnaNo ratings yet
- 3b. Diagnosis Non InfeksiDocument46 pages3b. Diagnosis Non Infeksimoadh ayashiNo ratings yet
- Practical Manual for Detection of Parasites in Feces, Blood and Urine SamplesFrom EverandPractical Manual for Detection of Parasites in Feces, Blood and Urine SamplesNo ratings yet
- 6 Cognitive Behavioral Therapy Techniques For Bipolar DisorderDocument7 pages6 Cognitive Behavioral Therapy Techniques For Bipolar Disorderprabha50% (2)
- Sheets For Hospital, Lama Adnan Tawili, 438004498, G2Document5 pagesSheets For Hospital, Lama Adnan Tawili, 438004498, G2lamaNo ratings yet
- PPT Case NephrolithiasisDocument45 pagesPPT Case NephrolithiasisRifka Anisa0% (1)
- Clinical CodingDocument40 pagesClinical CodingEndla NavyasreeNo ratings yet
- Gene TherapyDocument19 pagesGene TherapyJhayce Christian S. CapanayanNo ratings yet
- Acute Pain Nursing Care PlanDocument3 pagesAcute Pain Nursing Care PlanSiafei RabeNo ratings yet
- Onions: The Talmud Further Elucidates The Benefits of Onions With Regard To The Treatment of WoundsDocument2 pagesOnions: The Talmud Further Elucidates The Benefits of Onions With Regard To The Treatment of Woundsoutdash2No ratings yet
- Nested Case Control StudyDocument16 pagesNested Case Control Studyqtftwkwlf100% (1)
- March 2022 RecallsDocument292 pagesMarch 2022 RecallsNguyễn Nhật HoàngNo ratings yet
- Herbs MedicineDocument237 pagesHerbs MedicineSih Kir Nugroho100% (13)
- Periop 8Document18 pagesPeriop 8Bern GervacioNo ratings yet
- Cough, Cold and AllergiesDocument68 pagesCough, Cold and AllergiesLeonardo RanderNo ratings yet
- Phrenic Nerve DamageDocument15 pagesPhrenic Nerve DamageIzza Mae Ferrancol PastranaNo ratings yet
- Gynecology & Obstetrics Medical Conferences-The Ovary UnraveledDocument12 pagesGynecology & Obstetrics Medical Conferences-The Ovary Unraveledovary2009No ratings yet
- Treatment Management Between Orthodontists and General Practitioners Performing Clear Aligner TherapyDocument8 pagesTreatment Management Between Orthodontists and General Practitioners Performing Clear Aligner TherapyAmadeaNo ratings yet
- Thornwaldt Cyst - A Disease or AnomalyDocument4 pagesThornwaldt Cyst - A Disease or AnomalyresearchparksNo ratings yet
- Myoma Pathophysio, Gordon's NCPDocument13 pagesMyoma Pathophysio, Gordon's NCPicesexy100% (1)
- ATMIS Troops Provide Medical Supplies To Dhobley General HospitalDocument3 pagesATMIS Troops Provide Medical Supplies To Dhobley General HospitalAMISOM Public Information ServicesNo ratings yet
- MMMH-M-PAL-QP-003 Form1 Rev.1-Clinical Laboratory Request: City of Batac, Ilocos Norte, PhilippinesDocument1 pageMMMH-M-PAL-QP-003 Form1 Rev.1-Clinical Laboratory Request: City of Batac, Ilocos Norte, PhilippinesWyn AgustinNo ratings yet
- 20 Catalogue 2012Document33 pages20 Catalogue 2012Obehi EromoseleNo ratings yet
- Management For CTD - MsDocument63 pagesManagement For CTD - MsNarz CupahanNo ratings yet
- Endodontic Diagnosis, Pathology, and Treatment PlanningDocument17 pagesEndodontic Diagnosis, Pathology, and Treatment Planningrasagna reddyNo ratings yet
- PrakritiDocument3 pagesPrakritiSaini VarunNo ratings yet
- The National Academies Press: Emerging Needs and Opportunities For Human Factors Research (1995)Document28 pagesThe National Academies Press: Emerging Needs and Opportunities For Human Factors Research (1995)Darylle Ann MateroNo ratings yet
- Allegations Against The Princess Alexandra Hospital by DR Romesh SenewiratneDocument17 pagesAllegations Against The Princess Alexandra Hospital by DR Romesh SenewiratneDr Romesh Arya ChakravartiNo ratings yet
- The Pathophysiology & Practical Management of Diabetic KetoacidosisDocument45 pagesThe Pathophysiology & Practical Management of Diabetic KetoacidosisPreetibah PatelNo ratings yet
- Dermatotoxicology of Microneedles (MNS) in ManDocument8 pagesDermatotoxicology of Microneedles (MNS) in MansovalaxNo ratings yet
- Report On AmoebiasisDocument36 pagesReport On Amoebiasisrhimineecat71No ratings yet
- Case Write-Up 1 Obstructive Jaundice With Cholecystitis Secondary To Ampullary TumorDocument21 pagesCase Write-Up 1 Obstructive Jaundice With Cholecystitis Secondary To Ampullary TumorwhosenahNo ratings yet
- Polycythemia VeraDocument22 pagesPolycythemia VeraMelisande Rae CiruelaNo ratings yet