Download as pptx, pdf, or txt
You might also like
- Mms Protocol 2000Document2 pagesMms Protocol 2000bagus918No ratings yet
- Fit To Fly Certificate Proforma For Pregnant WomenDocument2 pagesFit To Fly Certificate Proforma For Pregnant Womenbaggagematters50% (6)
- Diabetes Mellitus Type 2 Schematic DiagramDocument1 pageDiabetes Mellitus Type 2 Schematic DiagramJhe Lyn82% (11)
- Gestational Diabetes Mellitus: Case PresentationDocument46 pagesGestational Diabetes Mellitus: Case PresentationATEHAN BORDSNo ratings yet
- Fetal ImagingDocument102 pagesFetal ImagingDameNo ratings yet
- Dminpregnancy 201109140122Document73 pagesDminpregnancy 201109140122EndaleNo ratings yet
- DM in PregnancyDocument11 pagesDM in Pregnancyميمونه عبد الرحيم مصطفىNo ratings yet
- MEDICAL COMPLICATIONS OF PREGNANCY ModuleDocument12 pagesMEDICAL COMPLICATIONS OF PREGNANCY ModuleWynjoy NebresNo ratings yet
- Diabetes in PregnancyDocument35 pagesDiabetes in PregnancySaladin AbrahimNo ratings yet
- Gestational Diabetes MellitusDocument16 pagesGestational Diabetes Mellitusarjunr19910% (1)
- GDM (Gestational Diabetes Mellitus) PresentationDocument32 pagesGDM (Gestational Diabetes Mellitus) PresentationMovies 4 YouNo ratings yet
- DR Farah Deeba Nasrullah Asst Prof Dept of Obgyn Unit Ii Chk/DuhsDocument14 pagesDR Farah Deeba Nasrullah Asst Prof Dept of Obgyn Unit Ii Chk/DuhsUloko ChristopherNo ratings yet
- Clecture 2Document20 pagesClecture 2zahrabokerNo ratings yet
- DM in PregnancyDocument35 pagesDM in Pregnancyapule geraldhumbleNo ratings yet
- Ayesha Khatun 15A, Topic - Diabetes and PregnancyDocument40 pagesAyesha Khatun 15A, Topic - Diabetes and PregnancyAyesha KhatunNo ratings yet
- Diabetes Mellitus in Pregnancy: DR - Shameem R. AlaasamDocument39 pagesDiabetes Mellitus in Pregnancy: DR - Shameem R. Alaasamhacker ammerNo ratings yet
- Gestational DiabetesDocument14 pagesGestational Diabetesamena mahmoudNo ratings yet
- Diabetes PregnancyDocument65 pagesDiabetes PregnancyJohn Christopher LucesNo ratings yet
- GDIABETUS MELITUS EyobDocument60 pagesGDIABETUS MELITUS Eyobm.pfortress.ojNo ratings yet
- Keya Thesis Updated 1Document40 pagesKeya Thesis Updated 1Noyon sheikhNo ratings yet
- Gestational Diabetes Mellitus (GDM) .TriceDocument47 pagesGestational Diabetes Mellitus (GDM) .TricejerrydanfordfxNo ratings yet
- Diabetes in PregnancyDocument23 pagesDiabetes in PregnancyMuratNo ratings yet
- GDMDocument38 pagesGDMAbhishiktaAbhi100% (1)
- DM InpregnancyDocument16 pagesDM Inpregnancyliathmahmood15No ratings yet
- Diabetes and Pregnancy: Syamel Muhammad, Dr. Spog K.OnkDocument41 pagesDiabetes and Pregnancy: Syamel Muhammad, Dr. Spog K.Onkyessy tamaraNo ratings yet
- Diabetes in Pregnancy: Supervisor: DR Rathimalar By: DR Ashwini Arumugam & DR Laily MokhtarDocument21 pagesDiabetes in Pregnancy: Supervisor: DR Rathimalar By: DR Ashwini Arumugam & DR Laily MokhtarHarleyquinn96 DrNo ratings yet
- Diabetes in Pregnancy: Umar Zein FK Unpri MedanDocument22 pagesDiabetes in Pregnancy: Umar Zein FK Unpri Medanyukmin rotamaNo ratings yet
- Diabetes and Pregnancy - SpencerDocument59 pagesDiabetes and Pregnancy - SpencerZH. omg sarNo ratings yet
- 14. DIP (1)Document20 pages14. DIP (1)sehamabdalsalam985No ratings yet
- Nutricare in Diabetes With Special ConditionsDocument40 pagesNutricare in Diabetes With Special ConditionsNudrat KhanNo ratings yet
- Gestational DiabetesDocument24 pagesGestational Diabeteshhpr9709No ratings yet
- Gestational Diabetes MellitusDocument4 pagesGestational Diabetes MellitusMaykel de GuzmanNo ratings yet
- Type1Diabetesinpregnancy: David R. Mccance,, Claire CaseyDocument15 pagesType1Diabetesinpregnancy: David R. Mccance,, Claire Caseyjose ricardo escalante perezNo ratings yet
- 11.pregnancy & Diabetes MellitusDocument23 pages11.pregnancy & Diabetes Mellituskume senbetaNo ratings yet
- Recent Advances in Management of Gestational Diabetes and Pre-EclampsiaDocument36 pagesRecent Advances in Management of Gestational Diabetes and Pre-EclampsiaSyed Zahed AliNo ratings yet
- Diabetes Mellitus During PregnancyDocument47 pagesDiabetes Mellitus During PregnancyFarida MohamedNo ratings yet
- Gestational Diabetes: Key PointsDocument5 pagesGestational Diabetes: Key PointsMayra PereiraNo ratings yet
- Inpatient Glycemic ManagementDocument13 pagesInpatient Glycemic Managementmiss betawiNo ratings yet
- Gestational Diabetes Mellitus Case Study AUG.17, 2021Document28 pagesGestational Diabetes Mellitus Case Study AUG.17, 2021Cruz, Donna Angela M.No ratings yet
- Gestational Diabetes MellitusDocument3 pagesGestational Diabetes MellitusJustine DumaguinNo ratings yet
- Complications Delivery InformationDocument22 pagesComplications Delivery Informationdiabetes asiaNo ratings yet
- Gestational Diabetes: Dr. Oyeyiola Oyebode Registrar Obstetrics and Gynaecology Ola Catholic Hospital, Oluyoro IbadanDocument40 pagesGestational Diabetes: Dr. Oyeyiola Oyebode Registrar Obstetrics and Gynaecology Ola Catholic Hospital, Oluyoro Ibadanoyebode oyeyiolaNo ratings yet
- Pregnant Woman Diabeties ComplicationsDocument3 pagesPregnant Woman Diabeties ComplicationsAdvanced Research PublicationsNo ratings yet
- Gestational Diabetes Mellitus (GDM) : Current Concept and A Short ReviewDocument1 pageGestational Diabetes Mellitus (GDM) : Current Concept and A Short ReviewTimothy Ho IINo ratings yet
- GDM FOGSI Text Book FinalDocument29 pagesGDM FOGSI Text Book FinalKruthika Devaraja GowdaNo ratings yet
- Gestational Diabetes and Diabetes in PregnancyDocument4 pagesGestational Diabetes and Diabetes in PregnancyIbrar AliNo ratings yet
- 21.diabetes Mellitus in PregnancyDocument47 pages21.diabetes Mellitus in Pregnancydeneke100% (1)
- Gestational Diabetes MellitusDocument21 pagesGestational Diabetes MellitusGlen Jacobs SumadihardjaNo ratings yet
- Diabetes in PregnancyDocument5 pagesDiabetes in Pregnancybluecrush1No ratings yet
- Diabetes Mellitus & Pregnancy by D.a.mehtaDocument31 pagesDiabetes Mellitus & Pregnancy by D.a.mehtadr.d.a.mehta11No ratings yet
- Gestational Diabetes MellitusDocument43 pagesGestational Diabetes MellitusDeepa Saravan100% (1)
- Diabetes in PregnancyDocument66 pagesDiabetes in PregnancySuhashis MukherjeeNo ratings yet
- Gestational Diabetes Mellitus: New Diagnostic CriteriaDocument7 pagesGestational Diabetes Mellitus: New Diagnostic CriteriaRambuNo ratings yet
- Ministry of Education and Scientific Research) ) Al-Muthanna University College of Medicine) )Document22 pagesMinistry of Education and Scientific Research) ) Al-Muthanna University College of Medicine) )Hussein H. MahmoodNo ratings yet
- Diabetes Mellitus in Pregnancy (Int)Document27 pagesDiabetes Mellitus in Pregnancy (Int)zizsatriaNo ratings yet
- Overt Diabetes: Diabetes Mellitus in PregnancyDocument3 pagesOvert Diabetes: Diabetes Mellitus in PregnancyBrian TiopengcoNo ratings yet
- The Implications of Obesity On Pregnancy Outcome 2015 Obstetrics Gynaecology Reproductive MedicineDocument4 pagesThe Implications of Obesity On Pregnancy Outcome 2015 Obstetrics Gynaecology Reproductive MedicineNora100% (1)
- Gestational DiabetesDocument21 pagesGestational DiabetesRiko Sampurna SimatupangNo ratings yet
- Diabetes in PregnancyDocument11 pagesDiabetes in PregnancyAlana CaballeroNo ratings yet
- GDMDocument66 pagesGDMpooja singhNo ratings yet
- DM in PregDocument32 pagesDM in Pregbryanpei23No ratings yet
- Diabetes in Pregnancy: Ryan Agema MS IIIDocument23 pagesDiabetes in Pregnancy: Ryan Agema MS IIIAkshat Goel100% (1)
- Conquering Diabetes: Fenugreek Success in Regulating Blood Sugar LevelsFrom EverandConquering Diabetes: Fenugreek Success in Regulating Blood Sugar LevelsNo ratings yet
- Syphilislecturepp 180719075049Document30 pagesSyphilislecturepp 180719075049EndaleNo ratings yet
- Syphilislecturepp 180719075049Document32 pagesSyphilislecturepp 180719075049EndaleNo ratings yet
- Management of Hepatitis B in Pregnancy C Obs 50Document17 pagesManagement of Hepatitis B in Pregnancy C Obs 50EndaleNo ratings yet
- VIRAL HEPATITIS IN PREGNANCY Copy 1Document48 pagesVIRAL HEPATITIS IN PREGNANCY Copy 1EndaleNo ratings yet
- Biostatistics-Haramaya University Full - Aug 25 2008Document88 pagesBiostatistics-Haramaya University Full - Aug 25 2008EndaleNo ratings yet
- Newborn AssessmentDocument6 pagesNewborn AssessmentAyuni Salleh100% (1)
- Hypertension in PregnancyDocument20 pagesHypertension in PregnancyRelly Arevalo-AramNo ratings yet
- PRESENTASIDocument25 pagesPRESENTASIEko andryNo ratings yet
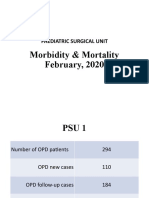
- Morbidity & Mortality (February, 2020)Document14 pagesMorbidity & Mortality (February, 2020)Wai GyiNo ratings yet
- Dr. Muneera GhaithanDocument44 pagesDr. Muneera GhaithanAli MezaalNo ratings yet
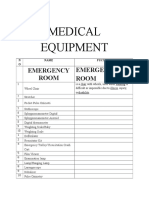
- Medical Equipment: Emergency Room Emergency RoomDocument7 pagesMedical Equipment: Emergency Room Emergency RoomNila CakepNo ratings yet
- Using PCL5Document5 pagesUsing PCL5Lorena Teodora Cazacu100% (1)
- Diarrhea: 1 DefinitionDocument13 pagesDiarrhea: 1 DefinitionZiedTriki100% (1)
- Kontrak Belajar Gadar Igd BaruDocument14 pagesKontrak Belajar Gadar Igd BaruAstridNo ratings yet
- THBT Woman Older Than 40 Should Not Have ChildrenDocument2 pagesTHBT Woman Older Than 40 Should Not Have ChildrenElma Nur HafizahNo ratings yet
- Criteria For MV WeaningDocument7 pagesCriteria For MV Weaning4g5xwdvh9sNo ratings yet
- Infections of The Eyes and The Central Nervous System by Dr. Joan E. CerradaDocument68 pagesInfections of The Eyes and The Central Nervous System by Dr. Joan E. CerradaMonique BorresNo ratings yet
- SIM 6 Circulatory SystemDocument1 pageSIM 6 Circulatory SystemJelly Flores100% (1)
- Basics Mechanical VentilationDocument51 pagesBasics Mechanical VentilationademNo ratings yet
- Intellicare - ACCREDITED SPECIALTYCLINICS As of June 2010Document3 pagesIntellicare - ACCREDITED SPECIALTYCLINICS As of June 2010Dey Ferrer OliveraNo ratings yet
- By: Dr. Safinaz Hamdy El Khoulany Lecturer of Medical Biochemistry and Molecular BiologyDocument13 pagesBy: Dr. Safinaz Hamdy El Khoulany Lecturer of Medical Biochemistry and Molecular BiologyEbtihal AboelfadlNo ratings yet
- Getting Started With Homeopathy - Find A RemedyDocument52 pagesGetting Started With Homeopathy - Find A Remedymadhavkrishna garg100% (1)
- Methanol Poisoning at A Glance PDFDocument2 pagesMethanol Poisoning at A Glance PDFAmeer MattaNo ratings yet
- Refractive Amblyopia: I Wayan Ardy Paribrajaka (1871122001)Document17 pagesRefractive Amblyopia: I Wayan Ardy Paribrajaka (1871122001)ratihpdewiNo ratings yet
- TB Child ExtrapulmonaryDocument9 pagesTB Child Extrapulmonarygiant nitaNo ratings yet
- Full Ebook of Physical Activity and Health The Evidence Explained 3Rd Edition Adrianne E Hardman Online PDF All ChapterDocument69 pagesFull Ebook of Physical Activity and Health The Evidence Explained 3Rd Edition Adrianne E Hardman Online PDF All Chaptergailadkerson379914100% (7)
- Prevention of Lifestyle Diseases Through Asbab-E-Sitta Zarooriyah (Six Essential Factors) of Unani Medicine: A ReviewDocument8 pagesPrevention of Lifestyle Diseases Through Asbab-E-Sitta Zarooriyah (Six Essential Factors) of Unani Medicine: A Reviewdrraja543No ratings yet
- Bladder CancerDocument57 pagesBladder CancerBANAWAN TRESHIA MAE D.No ratings yet
- Efn Topic 10 - Sulfi Nurafifah 1020031181Document10 pagesEfn Topic 10 - Sulfi Nurafifah 1020031181Erdin TriansyahNo ratings yet
- Hospitalisation Claim Form: Borang Tuntutan HospitalDocument2 pagesHospitalisation Claim Form: Borang Tuntutan HospitalMohd Azizee Bin SukorNo ratings yet
- Block C OSPE BPDocument2 pagesBlock C OSPE BPIrum RafeeqNo ratings yet