
Neonatal Chest X-Ray-2019
Neonatal Chest X-Ray-2019
You might also like
- Existential Therapies by Mick CooperDocument379 pagesExistential Therapies by Mick Cooperclive76100% (3)
- Genogram Assignment Mathews MarkDocument5 pagesGenogram Assignment Mathews Markapi-664106052No ratings yet
- Chest X-RayDocument101 pagesChest X-RayYuke04No ratings yet
- Pectus Carinatum, (Pigeon Chest) A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPectus Carinatum, (Pigeon Chest) A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Breast Feeding: OM Nursing Academy Anil Kantiwal GudhaDocument3 pagesBreast Feeding: OM Nursing Academy Anil Kantiwal GudhaBijay Kumar MahatoNo ratings yet
- Neonatal Chest X Ray 2019Document11 pagesNeonatal Chest X Ray 2019Ahmad ApriansahNo ratings yet
- Chest X-Ray Interpretation A Structured Approach Radiology OSCEDocument1 pageChest X-Ray Interpretation A Structured Approach Radiology OSCEValentina SepúlvedaNo ratings yet
- Adult Chest X-RayDocument60 pagesAdult Chest X-RayAnil DasNo ratings yet
- Interpretando RX PediatricoDocument10 pagesInterpretando RX PediatricosuzukishareNo ratings yet
- X Thorax BeoordelenDocument135 pagesX Thorax BeoordelenmtescasuraNo ratings yet
- Chest X-Rays: Phillip Smith, BA, RRTDocument29 pagesChest X-Rays: Phillip Smith, BA, RRTAlexandra PopaNo ratings yet
- Interpretasi Foto DadaDocument137 pagesInterpretasi Foto DadaRofi Irman100% (1)
- Basics of Chest X-RayDocument44 pagesBasics of Chest X-RayMelissa Aina Mohd YusofNo ratings yet
- Plain Chest X RayDocument154 pagesPlain Chest X RaySamuel Gamadey100% (3)
- Chest AssessmentDocument5 pagesChest Assessmentرحاب المريNo ratings yet
- Basic Chest Imaging and Heart FailureDocument57 pagesBasic Chest Imaging and Heart FailureKiaa auliaNo ratings yet
- Chest Xray BasicsDocument47 pagesChest Xray BasicsPartha GanesanNo ratings yet
- Topic 20. X-RayDocument4 pagesTopic 20. X-RayMadeline WanhartNo ratings yet
- Interpretation of Chest Imaging1Document91 pagesInterpretation of Chest Imaging1Brooke TurnerNo ratings yet
- Thoracic Imaging Radiographic BasicsDocument130 pagesThoracic Imaging Radiographic BasicsIsak ShatikaNo ratings yet
- Chest X-Ray CXR InterpretationDocument13 pagesChest X-Ray CXR InterpretationduncanNo ratings yet
- 2 1 Diseases of The Respiratory System Radiological Pathology DRDocument43 pages2 1 Diseases of The Respiratory System Radiological Pathology DRNatnael GetahunNo ratings yet
- Chest X-Ray ReviewDocument145 pagesChest X-Ray ReviewHamid ShaalanNo ratings yet
- Chest X-Ray GuideDocument26 pagesChest X-Ray GuideRizky Ayu WirdaningsiNo ratings yet
- Basics of Chest X-RayDocument44 pagesBasics of Chest X-RayvmamikonNo ratings yet
- RadioDocument58 pagesRadioMohSallakNo ratings yet
- Diagnostic Imaging - 8 - Radiological Pathology - Lung Pathologies and Radiology in Specific Cases - Prof - Dr.i̇smet TAMERDocument35 pagesDiagnostic Imaging - 8 - Radiological Pathology - Lung Pathologies and Radiology in Specific Cases - Prof - Dr.i̇smet TAMERAly MssreNo ratings yet
- Normal Chest RadiographDocument108 pagesNormal Chest RadiographVenu Madhav100% (1)
- Pemeriksaan Radiologi Pada Sistem Respirasi01Document115 pagesPemeriksaan Radiologi Pada Sistem Respirasi01Rendy NunuhituNo ratings yet
- Imaging of The Respiratory SystemDocument105 pagesImaging of The Respiratory SystemMizrab Nadeem100% (1)
- Neonatal Chest X-Ray Interpretation: Prof. Praveen KumarDocument7 pagesNeonatal Chest X-Ray Interpretation: Prof. Praveen KumarRaji MohanNo ratings yet
- Chest İmagi̇ngDocument83 pagesChest İmagi̇ngHamza EljoeidiNo ratings yet
- Cara Baca Foto ThoraxDocument23 pagesCara Baca Foto ThoraxNofilia Citra CandraNo ratings yet
- Basic Chest RadDocument112 pagesBasic Chest Radtesfayegermame95.tgNo ratings yet
- Basic Interpretation of CXRDocument84 pagesBasic Interpretation of CXRAbdiqani Mohamed AdanNo ratings yet
- Gambaran Radiologis Pada Kegawatan Paru: Farah Fatma WatiDocument42 pagesGambaran Radiologis Pada Kegawatan Paru: Farah Fatma WatisabariaNo ratings yet
- Chest X Ray SessionDocument110 pagesChest X Ray SessionzakiyaNo ratings yet
- CXR Reading Made EasyDocument94 pagesCXR Reading Made EasyMiaMDNo ratings yet
- Paediatric Chest X-RayDocument10 pagesPaediatric Chest X-Raypheeplukz100% (1)
- Pleural PathologiesDocument49 pagesPleural PathologiesIsaac ShirimaNo ratings yet
- Bonus Learning Chest X-RaysDocument13 pagesBonus Learning Chest X-RaysdeehteeNo ratings yet
- DR Hamdi's Cases 52.compressedDocument159 pagesDR Hamdi's Cases 52.compressedSlm BngshNo ratings yet
- 4 Respiratory ExaminationsDocument53 pages4 Respiratory Examinationscawsey mohamedNo ratings yet
- Pleural PathologiesDocument34 pagesPleural PathologiesAshwani RamawatNo ratings yet
- 3.the Respiratory SystemDocument29 pages3.the Respiratory SystemMUHAMMAD SAFWAN SUILENo ratings yet
- Radiology CWRU Medical Student Elective Week 1Document112 pagesRadiology CWRU Medical Student Elective Week 1Yopi SimargiNo ratings yet
- What Is Ultrasound?Document15 pagesWhat Is Ultrasound?Al-Mukashfi TahaNo ratings yet
- Chest X-Ray: Confirm DetailsDocument14 pagesChest X-Ray: Confirm DetailsNosheen HafeezNo ratings yet
- Basicinterpretationofcxr 110913060449 Phpapp01Document84 pagesBasicinterpretationofcxr 110913060449 Phpapp01Alexandra DîrțuNo ratings yet
- RT 321 Chest and AbdomenDocument85 pagesRT 321 Chest and Abdomenpntrdzj75wNo ratings yet
- Dr. Dicky SP.P Materi Gawat Darurat ParuDocument41 pagesDr. Dicky SP.P Materi Gawat Darurat ParuYuni SaviraNo ratings yet
- Chest X-RaysDocument39 pagesChest X-RaysDian Oktaria SafitriNo ratings yet
- Chest Radiography For InternsDocument42 pagesChest Radiography For InternsRose ValeNo ratings yet
- Chest Introduction: Technical AdequacyDocument28 pagesChest Introduction: Technical AdequacyAnshul JainNo ratings yet
- ABC ChestDocument4 pagesABC ChestSintounNo ratings yet
- Chest ImagingDocument51 pagesChest ImagingMikhayla ANo ratings yet
- Radiology AssignmentDocument27 pagesRadiology AssignmentRoyce GonzagaNo ratings yet
- Chest X-Ray Interpretation: Bucky Boaz, ARNP-CDocument101 pagesChest X-Ray Interpretation: Bucky Boaz, ARNP-CAnna DiaconuNo ratings yet
- IImage Critique &pattern Recognition-1Document52 pagesIImage Critique &pattern Recognition-1Rabiu Salisu yunusaNo ratings yet
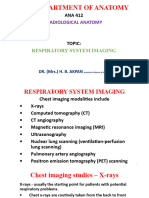
- ANA 412 Respiratory System ImagingDocument48 pagesANA 412 Respiratory System Imagingconqueror12345678No ratings yet
- Chest Radiology Med Students2Document137 pagesChest Radiology Med Students2Mike Oluwaseun AmooNo ratings yet
- Chest X-ray Interpretation for Radiographers, Nurses and Allied Health ProfessionalsFrom EverandChest X-ray Interpretation for Radiographers, Nurses and Allied Health ProfessionalsNo ratings yet
- Ihermanto, 1-WahdiDocument11 pagesIhermanto, 1-WahdiRipo Andi SaputraNo ratings yet
- JOURNAL CalpiDocument2 pagesJOURNAL CalpiBfpcar K PasilNo ratings yet
- Fundamentals of Cavity PreparationDocument76 pagesFundamentals of Cavity Preparationragakodali0% (1)
- Diagnostic Approach To The Patient With Newly Identified Chronic Kidney DiseaseDocument1 pageDiagnostic Approach To The Patient With Newly Identified Chronic Kidney DiseaseLauraNo ratings yet
- Final English Diary - 18062016Document437 pagesFinal English Diary - 18062016Aryan kumarNo ratings yet
- New Psycho ReportDocument18 pagesNew Psycho ReportnavquaNo ratings yet
- Anzir Zero DischargeDocument7 pagesAnzir Zero DischargeMohammad MahediNo ratings yet
- KlienDocument47 pagesKlientareq.sefatNo ratings yet
- Cannabis Withdrawal Scale PDFDocument1 pageCannabis Withdrawal Scale PDFSaya MenangNo ratings yet
- Consent Form PDFDocument2 pagesConsent Form PDFJhonalyn Laurio EstreraNo ratings yet
- AtelectasisDocument26 pagesAtelectasisArini NurlelaNo ratings yet
- Acquired Coagulation DisordersDocument11 pagesAcquired Coagulation DisordersAli AhmedNo ratings yet
- Đề Thi Anh Văn Chuyên Ngành Quản TrịDocument86 pagesĐề Thi Anh Văn Chuyên Ngành Quản TrịHiếu NguyễnNo ratings yet
- Federal Register / Vol. 73, No. 63 / Tuesday, April 1, 2008 / Proposed RulesDocument2 pagesFederal Register / Vol. 73, No. 63 / Tuesday, April 1, 2008 / Proposed Rulesj millerNo ratings yet
- DesignDocument2 pagesDesignPugazh enthiNo ratings yet
- NimbexDocument35 pagesNimbexfad12345No ratings yet
- Recruitment & SelectionDocument74 pagesRecruitment & SelectionNavneet Kumar0% (1)
- Research Proposal On Antimicrobial and Antioxidant Properties of Kiwi FruitDocument25 pagesResearch Proposal On Antimicrobial and Antioxidant Properties of Kiwi FruitCatherine100% (2)
- College of Criminal Justice Education Professor: Subject Code & Descriptive Title: Section: ScheduleDocument24 pagesCollege of Criminal Justice Education Professor: Subject Code & Descriptive Title: Section: ScheduleFranco Angelo ReyesNo ratings yet
- Fluoxetine in The Management of Pornography Addiction: Case ReportDocument3 pagesFluoxetine in The Management of Pornography Addiction: Case ReportRajat ChandelNo ratings yet
- Med AdmissionDocument3 pagesMed Admissionrujean romy p guisandoNo ratings yet
- Whipple Procedure and Its Complications: What Every Radiologist Should KnowDocument17 pagesWhipple Procedure and Its Complications: What Every Radiologist Should KnowYacine Tarik AizelNo ratings yet
- Guilford Child & Adolescent Psychology Chapter SamplerDocument97 pagesGuilford Child & Adolescent Psychology Chapter SamplerAdelaKočanBahtoNo ratings yet
- API Versus OSHADocument6 pagesAPI Versus OSHAGMSNo ratings yet
- IDLAR October 2021 Maam Marisa 2Document15 pagesIDLAR October 2021 Maam Marisa 2Llemor Soled SeyerNo ratings yet
- A Practical Handbook of Pancha Karma ProceduresDocument92 pagesA Practical Handbook of Pancha Karma ProceduresHari100% (1)
- Drug Calc Sample QuestionsDocument12 pagesDrug Calc Sample QuestionsRastie MendozaNo ratings yet























































































Download as pptx, pdf, or txt
You might also like
- Existential Therapies by Mick CooperDocument379 pagesExistential Therapies by Mick Cooperclive76100% (3)
- Genogram Assignment Mathews MarkDocument5 pagesGenogram Assignment Mathews Markapi-664106052No ratings yet
- Chest X-RayDocument101 pagesChest X-RayYuke04No ratings yet
- Pectus Carinatum, (Pigeon Chest) A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPectus Carinatum, (Pigeon Chest) A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Breast Feeding: OM Nursing Academy Anil Kantiwal GudhaDocument3 pagesBreast Feeding: OM Nursing Academy Anil Kantiwal GudhaBijay Kumar MahatoNo ratings yet
- Neonatal Chest X Ray 2019Document11 pagesNeonatal Chest X Ray 2019Ahmad ApriansahNo ratings yet
- Chest X-Ray Interpretation A Structured Approach Radiology OSCEDocument1 pageChest X-Ray Interpretation A Structured Approach Radiology OSCEValentina SepúlvedaNo ratings yet
- Adult Chest X-RayDocument60 pagesAdult Chest X-RayAnil DasNo ratings yet
- Interpretando RX PediatricoDocument10 pagesInterpretando RX PediatricosuzukishareNo ratings yet
- X Thorax BeoordelenDocument135 pagesX Thorax BeoordelenmtescasuraNo ratings yet
- Chest X-Rays: Phillip Smith, BA, RRTDocument29 pagesChest X-Rays: Phillip Smith, BA, RRTAlexandra PopaNo ratings yet
- Interpretasi Foto DadaDocument137 pagesInterpretasi Foto DadaRofi Irman100% (1)
- Basics of Chest X-RayDocument44 pagesBasics of Chest X-RayMelissa Aina Mohd YusofNo ratings yet
- Plain Chest X RayDocument154 pagesPlain Chest X RaySamuel Gamadey100% (3)
- Chest AssessmentDocument5 pagesChest Assessmentرحاب المريNo ratings yet
- Basic Chest Imaging and Heart FailureDocument57 pagesBasic Chest Imaging and Heart FailureKiaa auliaNo ratings yet
- Chest Xray BasicsDocument47 pagesChest Xray BasicsPartha GanesanNo ratings yet
- Topic 20. X-RayDocument4 pagesTopic 20. X-RayMadeline WanhartNo ratings yet
- Interpretation of Chest Imaging1Document91 pagesInterpretation of Chest Imaging1Brooke TurnerNo ratings yet
- Thoracic Imaging Radiographic BasicsDocument130 pagesThoracic Imaging Radiographic BasicsIsak ShatikaNo ratings yet
- Chest X-Ray CXR InterpretationDocument13 pagesChest X-Ray CXR InterpretationduncanNo ratings yet
- 2 1 Diseases of The Respiratory System Radiological Pathology DRDocument43 pages2 1 Diseases of The Respiratory System Radiological Pathology DRNatnael GetahunNo ratings yet
- Chest X-Ray ReviewDocument145 pagesChest X-Ray ReviewHamid ShaalanNo ratings yet
- Chest X-Ray GuideDocument26 pagesChest X-Ray GuideRizky Ayu WirdaningsiNo ratings yet
- Basics of Chest X-RayDocument44 pagesBasics of Chest X-RayvmamikonNo ratings yet
- RadioDocument58 pagesRadioMohSallakNo ratings yet
- Diagnostic Imaging - 8 - Radiological Pathology - Lung Pathologies and Radiology in Specific Cases - Prof - Dr.i̇smet TAMERDocument35 pagesDiagnostic Imaging - 8 - Radiological Pathology - Lung Pathologies and Radiology in Specific Cases - Prof - Dr.i̇smet TAMERAly MssreNo ratings yet
- Normal Chest RadiographDocument108 pagesNormal Chest RadiographVenu Madhav100% (1)
- Pemeriksaan Radiologi Pada Sistem Respirasi01Document115 pagesPemeriksaan Radiologi Pada Sistem Respirasi01Rendy NunuhituNo ratings yet
- Imaging of The Respiratory SystemDocument105 pagesImaging of The Respiratory SystemMizrab Nadeem100% (1)
- Neonatal Chest X-Ray Interpretation: Prof. Praveen KumarDocument7 pagesNeonatal Chest X-Ray Interpretation: Prof. Praveen KumarRaji MohanNo ratings yet
- Chest İmagi̇ngDocument83 pagesChest İmagi̇ngHamza EljoeidiNo ratings yet
- Cara Baca Foto ThoraxDocument23 pagesCara Baca Foto ThoraxNofilia Citra CandraNo ratings yet
- Basic Chest RadDocument112 pagesBasic Chest Radtesfayegermame95.tgNo ratings yet
- Basic Interpretation of CXRDocument84 pagesBasic Interpretation of CXRAbdiqani Mohamed AdanNo ratings yet
- Gambaran Radiologis Pada Kegawatan Paru: Farah Fatma WatiDocument42 pagesGambaran Radiologis Pada Kegawatan Paru: Farah Fatma WatisabariaNo ratings yet
- Chest X Ray SessionDocument110 pagesChest X Ray SessionzakiyaNo ratings yet
- CXR Reading Made EasyDocument94 pagesCXR Reading Made EasyMiaMDNo ratings yet
- Paediatric Chest X-RayDocument10 pagesPaediatric Chest X-Raypheeplukz100% (1)
- Pleural PathologiesDocument49 pagesPleural PathologiesIsaac ShirimaNo ratings yet
- Bonus Learning Chest X-RaysDocument13 pagesBonus Learning Chest X-RaysdeehteeNo ratings yet
- DR Hamdi's Cases 52.compressedDocument159 pagesDR Hamdi's Cases 52.compressedSlm BngshNo ratings yet
- 4 Respiratory ExaminationsDocument53 pages4 Respiratory Examinationscawsey mohamedNo ratings yet
- Pleural PathologiesDocument34 pagesPleural PathologiesAshwani RamawatNo ratings yet
- 3.the Respiratory SystemDocument29 pages3.the Respiratory SystemMUHAMMAD SAFWAN SUILENo ratings yet
- Radiology CWRU Medical Student Elective Week 1Document112 pagesRadiology CWRU Medical Student Elective Week 1Yopi SimargiNo ratings yet
- What Is Ultrasound?Document15 pagesWhat Is Ultrasound?Al-Mukashfi TahaNo ratings yet
- Chest X-Ray: Confirm DetailsDocument14 pagesChest X-Ray: Confirm DetailsNosheen HafeezNo ratings yet
- Basicinterpretationofcxr 110913060449 Phpapp01Document84 pagesBasicinterpretationofcxr 110913060449 Phpapp01Alexandra DîrțuNo ratings yet
- RT 321 Chest and AbdomenDocument85 pagesRT 321 Chest and Abdomenpntrdzj75wNo ratings yet
- Dr. Dicky SP.P Materi Gawat Darurat ParuDocument41 pagesDr. Dicky SP.P Materi Gawat Darurat ParuYuni SaviraNo ratings yet
- Chest X-RaysDocument39 pagesChest X-RaysDian Oktaria SafitriNo ratings yet
- Chest Radiography For InternsDocument42 pagesChest Radiography For InternsRose ValeNo ratings yet
- Chest Introduction: Technical AdequacyDocument28 pagesChest Introduction: Technical AdequacyAnshul JainNo ratings yet
- ABC ChestDocument4 pagesABC ChestSintounNo ratings yet
- Chest ImagingDocument51 pagesChest ImagingMikhayla ANo ratings yet
- Radiology AssignmentDocument27 pagesRadiology AssignmentRoyce GonzagaNo ratings yet
- Chest X-Ray Interpretation: Bucky Boaz, ARNP-CDocument101 pagesChest X-Ray Interpretation: Bucky Boaz, ARNP-CAnna DiaconuNo ratings yet
- IImage Critique &pattern Recognition-1Document52 pagesIImage Critique &pattern Recognition-1Rabiu Salisu yunusaNo ratings yet
- ANA 412 Respiratory System ImagingDocument48 pagesANA 412 Respiratory System Imagingconqueror12345678No ratings yet
- Chest Radiology Med Students2Document137 pagesChest Radiology Med Students2Mike Oluwaseun AmooNo ratings yet
- Chest X-ray Interpretation for Radiographers, Nurses and Allied Health ProfessionalsFrom EverandChest X-ray Interpretation for Radiographers, Nurses and Allied Health ProfessionalsNo ratings yet
- Ihermanto, 1-WahdiDocument11 pagesIhermanto, 1-WahdiRipo Andi SaputraNo ratings yet
- JOURNAL CalpiDocument2 pagesJOURNAL CalpiBfpcar K PasilNo ratings yet
- Fundamentals of Cavity PreparationDocument76 pagesFundamentals of Cavity Preparationragakodali0% (1)
- Diagnostic Approach To The Patient With Newly Identified Chronic Kidney DiseaseDocument1 pageDiagnostic Approach To The Patient With Newly Identified Chronic Kidney DiseaseLauraNo ratings yet
- Final English Diary - 18062016Document437 pagesFinal English Diary - 18062016Aryan kumarNo ratings yet
- New Psycho ReportDocument18 pagesNew Psycho ReportnavquaNo ratings yet
- Anzir Zero DischargeDocument7 pagesAnzir Zero DischargeMohammad MahediNo ratings yet
- KlienDocument47 pagesKlientareq.sefatNo ratings yet
- Cannabis Withdrawal Scale PDFDocument1 pageCannabis Withdrawal Scale PDFSaya MenangNo ratings yet
- Consent Form PDFDocument2 pagesConsent Form PDFJhonalyn Laurio EstreraNo ratings yet
- AtelectasisDocument26 pagesAtelectasisArini NurlelaNo ratings yet
- Acquired Coagulation DisordersDocument11 pagesAcquired Coagulation DisordersAli AhmedNo ratings yet
- Đề Thi Anh Văn Chuyên Ngành Quản TrịDocument86 pagesĐề Thi Anh Văn Chuyên Ngành Quản TrịHiếu NguyễnNo ratings yet
- Federal Register / Vol. 73, No. 63 / Tuesday, April 1, 2008 / Proposed RulesDocument2 pagesFederal Register / Vol. 73, No. 63 / Tuesday, April 1, 2008 / Proposed Rulesj millerNo ratings yet
- DesignDocument2 pagesDesignPugazh enthiNo ratings yet
- NimbexDocument35 pagesNimbexfad12345No ratings yet
- Recruitment & SelectionDocument74 pagesRecruitment & SelectionNavneet Kumar0% (1)
- Research Proposal On Antimicrobial and Antioxidant Properties of Kiwi FruitDocument25 pagesResearch Proposal On Antimicrobial and Antioxidant Properties of Kiwi FruitCatherine100% (2)
- College of Criminal Justice Education Professor: Subject Code & Descriptive Title: Section: ScheduleDocument24 pagesCollege of Criminal Justice Education Professor: Subject Code & Descriptive Title: Section: ScheduleFranco Angelo ReyesNo ratings yet
- Fluoxetine in The Management of Pornography Addiction: Case ReportDocument3 pagesFluoxetine in The Management of Pornography Addiction: Case ReportRajat ChandelNo ratings yet
- Med AdmissionDocument3 pagesMed Admissionrujean romy p guisandoNo ratings yet
- Whipple Procedure and Its Complications: What Every Radiologist Should KnowDocument17 pagesWhipple Procedure and Its Complications: What Every Radiologist Should KnowYacine Tarik AizelNo ratings yet
- Guilford Child & Adolescent Psychology Chapter SamplerDocument97 pagesGuilford Child & Adolescent Psychology Chapter SamplerAdelaKočanBahtoNo ratings yet
- API Versus OSHADocument6 pagesAPI Versus OSHAGMSNo ratings yet
- IDLAR October 2021 Maam Marisa 2Document15 pagesIDLAR October 2021 Maam Marisa 2Llemor Soled SeyerNo ratings yet
- A Practical Handbook of Pancha Karma ProceduresDocument92 pagesA Practical Handbook of Pancha Karma ProceduresHari100% (1)
- Drug Calc Sample QuestionsDocument12 pagesDrug Calc Sample QuestionsRastie MendozaNo ratings yet