Download as pptx, pdf, or txt
You might also like
- Educational Assessment Mcqs For PSC HeadmasterDocument24 pagesEducational Assessment Mcqs For PSC Headmastersrinivasana67% (132)
- Summary of BenefitsDocument4 pagesSummary of BenefitsMylene Jay PasosNo ratings yet
- Lesson Plan Nephrotic SyndromeDocument9 pagesLesson Plan Nephrotic SyndromeEllen Angel50% (2)
- 3 Step Stamina PDF EbookDocument23 pages3 Step Stamina PDF EbookFahmid Rayhan Aurin100% (1)
- Gangguan Pada Ginjal Dan UreterDocument127 pagesGangguan Pada Ginjal Dan UreterFebrina TrizaNo ratings yet
- Case Report ..Document69 pagesCase Report ..sashadilanNo ratings yet
- Disorders of The Kidneys and Ureters3962Document110 pagesDisorders of The Kidneys and Ureters3962Nikki M. Arapol100% (1)
- Nephrotic SyndromeDocument12 pagesNephrotic Syndromehusenbrz4No ratings yet
- Nephrotic SyndromeeDocument28 pagesNephrotic SyndromeeRiteka SinghNo ratings yet
- Acute GlomerulonephritisDocument6 pagesAcute GlomerulonephritisAnsu MaliyakalNo ratings yet
- Altered Genitourinary/Renal FunctionDocument14 pagesAltered Genitourinary/Renal FunctionAshleyNo ratings yet
- Nephrotic SyndromeDocument21 pagesNephrotic Syndromepreetie8750% (4)
- Urinary Tract DisordersDocument54 pagesUrinary Tract Disorderssharon ocharaNo ratings yet
- GlomerulonephritisDocument8 pagesGlomerulonephritisMatthew Ryan100% (1)
- Acute Glomerulonephritis: Reference: Wong's Nsg. Care of Infants and Children (8 Edition)Document7 pagesAcute Glomerulonephritis: Reference: Wong's Nsg. Care of Infants and Children (8 Edition)Ferna Criselda Susano ViescaNo ratings yet
- Diarrhea 1Document5 pagesDiarrhea 1Mohammed Taha Al-nuaimyNo ratings yet
- Nephrotic SyndromeDocument24 pagesNephrotic SyndromeJawad SaleemNo ratings yet
- Nephrotic SyndromeDocument28 pagesNephrotic Syndromerupali khillareNo ratings yet
- Case Study 2020 Multiple Myeloma With BMT Leak Resulting in Septic ShockDocument56 pagesCase Study 2020 Multiple Myeloma With BMT Leak Resulting in Septic Shockapi-519485865No ratings yet
- Glomerulonephritis in ChildrenDocument10 pagesGlomerulonephritis in ChildrenPGDME 20192020No ratings yet
- Nephrotic Syndrome: Prepared By: Manisha Praharaj Msc. Nursing 2Nd YearDocument28 pagesNephrotic Syndrome: Prepared By: Manisha Praharaj Msc. Nursing 2Nd YearMaria YaseenNo ratings yet
- Diarrhea: Cause Signs and Symptoms Pathophysiolog Y Prognosis StatisticsDocument13 pagesDiarrhea: Cause Signs and Symptoms Pathophysiolog Y Prognosis StatisticsRogie SaludoNo ratings yet
- ACUTE DIARRHOEA Pediatric 2024Document35 pagesACUTE DIARRHOEA Pediatric 2024richardkikondo5No ratings yet
- Causes of Henoch-Schönlein Syndrome NephritisDocument6 pagesCauses of Henoch-Schönlein Syndrome NephritisJimae Rose BaculaNo ratings yet
- Diarrheal DiseaseDocument47 pagesDiarrheal Diseasemy Lord JesusNo ratings yet
- Pediatric Renal DisordersDocument9 pagesPediatric Renal DisordersNadia AmroNo ratings yet
- Crystel Sheena Baguisa-Reyes, MDDocument30 pagesCrystel Sheena Baguisa-Reyes, MDLeslee Cruz - BernardinoNo ratings yet
- Nephrotic Syndrome FinalDocument5 pagesNephrotic Syndrome FinalAaron AntonioNo ratings yet
- Gastroenteritis in ChildrenDocument48 pagesGastroenteritis in ChildrenKelsingra FitzChivalry FarseerNo ratings yet
- Acute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CDocument29 pagesAcute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CEdelrose Lapitan100% (1)
- Acute Glomerulonephritis (AGN) : Group A Beta Hemolytic StretococcusDocument3 pagesAcute Glomerulonephritis (AGN) : Group A Beta Hemolytic StretococcusKristine Danielle DejeloNo ratings yet
- General Data: G.E.L. Male 3 Yo Roman Catholic Brgy. Dungon C. Mandurrio Iloilo CityDocument75 pagesGeneral Data: G.E.L. Male 3 Yo Roman Catholic Brgy. Dungon C. Mandurrio Iloilo CityRhaffy Bearneza RapaconNo ratings yet
- GroupA RenalDisordersDocument13 pagesGroupA RenalDisordersPaulNo ratings yet
- Urinary and Renal DisordersDocument45 pagesUrinary and Renal DisordersHarper EppsNo ratings yet
- Drug StudyDocument3 pagesDrug StudyFloribelle SamaniegoNo ratings yet
- Acute GastroenteritisDocument63 pagesAcute GastroenteritisSathya MoorthyNo ratings yet
- A 27Document10 pagesA 27NestleNo ratings yet
- Nephrotic SyndromeDocument70 pagesNephrotic SyndromeNaz Al-ShahraniNo ratings yet
- Nursing Patho CardsDocument195 pagesNursing Patho Cardsgiogmail100% (1)
- By DR - Tosif Ahmad TMO-PediatricsDocument27 pagesBy DR - Tosif Ahmad TMO-PediatricskamalNo ratings yet
- Acute GastroenteritisDocument54 pagesAcute GastroenteritisVincent LaranjoNo ratings yet
- Pediatric Osce Compiled by NoorUlAin.Document29 pagesPediatric Osce Compiled by NoorUlAin.amashooquekubarNo ratings yet
- Nephritis NephrosisDocument43 pagesNephritis NephrosisE=MC2No ratings yet
- Acute Watery Diarrhea (1399-05-22)Document31 pagesAcute Watery Diarrhea (1399-05-22)Shams Ul HaqNo ratings yet
- Acute Glomerulonephritis (Agn)Document42 pagesAcute Glomerulonephritis (Agn)Rowshon AraNo ratings yet
- Nephrotic SyndrDocument8 pagesNephrotic SyndrChioma Cynthia UdebuaniNo ratings yet
- Dental Management of Diabetic PatientsDocument30 pagesDental Management of Diabetic PatientsChitrang KolawaleNo ratings yet
- Nephrotic SyndromeDocument24 pagesNephrotic SyndromeSamah KhanNo ratings yet
- What Is Acute Glomerulonephritis?: Acute Glomerulonephritis (GN) Comprises A Specific Set of Renal Diseases inDocument6 pagesWhat Is Acute Glomerulonephritis?: Acute Glomerulonephritis (GN) Comprises A Specific Set of Renal Diseases inAnnapoorna SHNo ratings yet
- Acute GastroenteritisDocument51 pagesAcute GastroenteritisuouoNo ratings yet
- Neurological Disorders: HypertensionDocument10 pagesNeurological Disorders: HypertensionAnn ThanNo ratings yet
- Ch 54 Kidney Study GuideDocument18 pagesCh 54 Kidney Study GuideMichelle Dona MirallesNo ratings yet
- Counselling On Disorders - NotesDocument5 pagesCounselling On Disorders - NotesRichard BudNo ratings yet
- VND Openxmlformats-Officedocument PresentationmlDocument20 pagesVND Openxmlformats-Officedocument Presentationmlvirgo paigeNo ratings yet
- Clinical Features A) Upper Urinary Tract (Pyelonephritis) :: T:Marwa AL-Headri 1Document16 pagesClinical Features A) Upper Urinary Tract (Pyelonephritis) :: T:Marwa AL-Headri 1abnaltag667No ratings yet
- Diabetes Mellitus PatientsDocument33 pagesDiabetes Mellitus PatientsShabeel PnNo ratings yet
- Anatomy of The KidneysDocument7 pagesAnatomy of The KidneysSanthu SuNo ratings yet
- Folio BiologyDocument38 pagesFolio BiologySiti NurhidayuNo ratings yet
- طلاب كروب C سشنات د.ندى-1 (Muhadharaty)Document6 pagesطلاب كروب C سشنات د.ندى-1 (Muhadharaty)mohammed almaaziNo ratings yet
- Acute Glomerulonephritis: By: Jhaziel E. BermejoDocument20 pagesAcute Glomerulonephritis: By: Jhaziel E. BermejoJhaziel BermejoNo ratings yet
- NephritisDocument20 pagesNephritisSaima ParveenNo ratings yet
- Nursing Care of Clients With Urinary Tract DisordersDocument70 pagesNursing Care of Clients With Urinary Tract DisordersYuu Ayu'k LifestarNo ratings yet
- Pathology of Pulmonary TBDocument3 pagesPathology of Pulmonary TBJils SureshNo ratings yet
- ThrombosisDocument2 pagesThrombosisJils SureshNo ratings yet
- Ratng ScaleDocument6 pagesRatng ScaleJils SureshNo ratings yet
- Toddler Growth and DevelopmentDocument20 pagesToddler Growth and DevelopmentJils SureshNo ratings yet
- The Normal Toddler Growth and DevelopmentDocument8 pagesThe Normal Toddler Growth and DevelopmentJils SureshNo ratings yet
- Newborn ReflexesDocument12 pagesNewborn ReflexesJils SureshNo ratings yet
- School AgeDocument10 pagesSchool AgeJils SureshNo ratings yet
- Neurologic DisorderDocument77 pagesNeurologic DisorderJils SureshNo ratings yet
- Seminar and SymposiumDocument13 pagesSeminar and SymposiumJils SureshNo ratings yet
- WeaningDocument4 pagesWeaningJils SureshNo ratings yet
- GastroenteritisDocument14 pagesGastroenteritisJils SureshNo ratings yet
- Typhoid in ChildrenDocument3 pagesTyphoid in ChildrenJils SureshNo ratings yet
- Hirschsprung DiseaseDocument28 pagesHirschsprung DiseaseJils SureshNo ratings yet
- Oral CancerDocument11 pagesOral CancerJils SureshNo ratings yet
- Growth and Development of PreschoolerDocument6 pagesGrowth and Development of PreschoolerJils SureshNo ratings yet
- ChemotherapyDocument15 pagesChemotherapyJils SureshNo ratings yet
- OncologyDocument24 pagesOncologyJils SureshNo ratings yet
- Breast CancerDocument27 pagesBreast CancerJils SureshNo ratings yet
- Gastric CancerDocument16 pagesGastric CancerJils SureshNo ratings yet
- Bone Marrow TransplantationDocument8 pagesBone Marrow TransplantationJils SureshNo ratings yet
- Cancer of The CervixDocument14 pagesCancer of The CervixJils SureshNo ratings yet
- Radiation TherapyDocument13 pagesRadiation TherapyJils SureshNo ratings yet
- Laryngeal CancerDocument13 pagesLaryngeal CancerJils SureshNo ratings yet
- MusicStudies PDFDocument2 pagesMusicStudies PDFRosie VegaNo ratings yet
- Aip Budget 2024 Needed DataDocument22 pagesAip Budget 2024 Needed Datamoox TVNo ratings yet
- Lesson Plan 2 Ganag ModelDocument3 pagesLesson Plan 2 Ganag Modelapi-384875207No ratings yet
- Isilimela Hospital Speech Therapy DepartmentDocument2 pagesIsilimela Hospital Speech Therapy DepartmentSuné GreeffNo ratings yet
- Newport E100i Service ManualDocument86 pagesNewport E100i Service ManualleotenfenNo ratings yet
- Zeniton 70 IFUDocument292 pagesZeniton 70 IFUyoelalperinbackupNo ratings yet
- Assessing Spiritual Needs - HOPEDocument5 pagesAssessing Spiritual Needs - HOPEKrisna May Buhisan PecoreNo ratings yet
- Jurnal Surya: Pengaruh Terapi Musik Terhadap Penurunan Intensitas Nyeri Pada Pasien Post OperasiDocument18 pagesJurnal Surya: Pengaruh Terapi Musik Terhadap Penurunan Intensitas Nyeri Pada Pasien Post Operasisekarwidya putriNo ratings yet
- BU Reaction Paper ChavezDocument2 pagesBU Reaction Paper ChavezShrwn JcNo ratings yet
- Benign Lesions of Vulva and VaginaDocument34 pagesBenign Lesions of Vulva and VaginaCabdiNo ratings yet
- Contri Butions of The Psychosoc I A L SC Iences: 2.1 Jean Piaget and Cognitive DevelopmentDocument38 pagesContri Butions of The Psychosoc I A L SC Iences: 2.1 Jean Piaget and Cognitive Developmentdaily of sinta fuNo ratings yet
- Bahasa Arab Sekitar Kamar MandiDocument2 pagesBahasa Arab Sekitar Kamar MandiRizky FebrianNo ratings yet
- Ahlstrom-Reliance-Customer-Brochure (P.10 Highlight)Document12 pagesAhlstrom-Reliance-Customer-Brochure (P.10 Highlight)Panthita SrisumranNo ratings yet
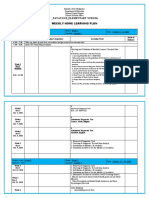
- Payatas B - Elementary School: Weekly Home Learning PlanDocument4 pagesPayatas B - Elementary School: Weekly Home Learning PlanCatherine RenanteNo ratings yet
- PDF Dove Brand Audit Report DLDocument10 pagesPDF Dove Brand Audit Report DLDuyen P TranNo ratings yet
- Operative DeliveryDocument19 pagesOperative DeliveryMtwe ZakayoNo ratings yet
- A Study On Stress ManagementDocument8 pagesA Study On Stress Managementritika rustagiNo ratings yet
- Angela & Andrei-Protocol of A LoveDocument10 pagesAngela & Andrei-Protocol of A LoveIgor Pop TrajkovNo ratings yet
- Clinical-Chemistry DHA MCQDocument27 pagesClinical-Chemistry DHA MCQAsif Newaz100% (2)
- Creolin Eco MSDSDocument9 pagesCreolin Eco MSDSMusa SabujNo ratings yet
- Ota Go Correctional FacilityDocument14 pagesOta Go Correctional FacilityKier Marcial V. Collao IVNo ratings yet
- Is Iso 10555 1 1995Document21 pagesIs Iso 10555 1 1995Hemant SharmaNo ratings yet
- DRR11/12-Ic-8. Explain The Meaning of VulnerabilityDocument6 pagesDRR11/12-Ic-8. Explain The Meaning of VulnerabilityallanrnmanalotoNo ratings yet
- Lepy 103Document19 pagesLepy 103Syed FerozNo ratings yet
- Training Manual For Mechanical Maintenance Personal: STD 4500/29,5x1,2Document63 pagesTraining Manual For Mechanical Maintenance Personal: STD 4500/29,5x1,2jhon omarNo ratings yet
- Bdo04122021 1Document52 pagesBdo04122021 1RuchiNo ratings yet
- Transitional Housing ListDocument27 pagesTransitional Housing ListA IDOHERBALIFE IDOHERBABBASLIFENo ratings yet