Download as pptx, pdf, or txt
You might also like
- Margaret Newman TheoryDocument33 pagesMargaret Newman TheoryGracia100% (3)
- Bronchiolitis - Discharge SummaryDocument2 pagesBronchiolitis - Discharge SummaryIndranil SinhaNo ratings yet
- Medicinal Plants of BalochistanDocument39 pagesMedicinal Plants of Balochistanfatmanscooby86% (7)
- Isoenzyme ClassifiedDocument33 pagesIsoenzyme Classifiedsayush754No ratings yet
- IsoenzymesDocument10 pagesIsoenzymesAbhayNo ratings yet
- Biochem IsoenzymesDocument21 pagesBiochem IsoenzymesGor ShreyashNo ratings yet
- Isoenzymes-Multienzyme Complex PDFDocument20 pagesIsoenzymes-Multienzyme Complex PDFintaliallitaNo ratings yet
- Isoenzyme - Lactate Dehydrogenase: By, Ishaque P K Biochemistry Pondicherry UniversityDocument17 pagesIsoenzyme - Lactate Dehydrogenase: By, Ishaque P K Biochemistry Pondicherry UniversityBETTYNo ratings yet
- Enzymology: Cardiac Markers Pancreatic Markers Prostate MarkersDocument48 pagesEnzymology: Cardiac Markers Pancreatic Markers Prostate MarkersValdez Francis ZaccheauNo ratings yet
- Zymogen, Isozymes, Abzymes, RibozymesDocument9 pagesZymogen, Isozymes, Abzymes, Ribozymesr6jxkkg7nqNo ratings yet
- Isoenzymes Multienzyme ComplexDocument20 pagesIsoenzymes Multienzyme ComplexAnisam Abhi100% (2)
- Isoenzymes: Plasma EnzymesDocument47 pagesIsoenzymes: Plasma Enzymesbushra vainceNo ratings yet
- LECTURE 6 - Clinical Significance of EnzymesDocument3 pagesLECTURE 6 - Clinical Significance of EnzymesDoreenNo ratings yet
- Enzim CardiovascularDocument64 pagesEnzim Cardiovascularandre kesumaNo ratings yet
- Markers of Muscle Damage - Recorde - June 020Document28 pagesMarkers of Muscle Damage - Recorde - June 020Abhishek PandeyNo ratings yet
- PBL Enzymes 1Document40 pagesPBL Enzymes 1cityNo ratings yet
- Blood (Autosaved)Document24 pagesBlood (Autosaved)jay daxiniNo ratings yet
- Clinical Enzymology: (Clinical Biochemistry of Enzymes)Document10 pagesClinical Enzymology: (Clinical Biochemistry of Enzymes)Dawlat SalamaNo ratings yet
- Clinical EnzymologyDocument28 pagesClinical EnzymologySparrowNo ratings yet
- Lecture 2 Biochemistry of Enzyme and Clinical EnzymologyDocument24 pagesLecture 2 Biochemistry of Enzyme and Clinical Enzymologybeneficialboxer9237No ratings yet
- AnaPhyLc - 2.1 Chemistry of LifeDocument36 pagesAnaPhyLc - 2.1 Chemistry of LifeKyarra MedenillaNo ratings yet
- EnzymesDocument18 pagesEnzymesRichard PoonNo ratings yet
- Clinical Importance of EnzymesDocument37 pagesClinical Importance of Enzymesdhatriharsh.13No ratings yet
- Enzymes: M. Zaharna Clin. Chem. 2009Document33 pagesEnzymes: M. Zaharna Clin. Chem. 2009Ahmed GaberNo ratings yet
- Iso Enzymes & Clinical Importance of EnzymesDocument33 pagesIso Enzymes & Clinical Importance of EnzymesLakshman Raj50% (2)
- PDF Enzymes of Clinical ImportanceDocument8 pagesPDF Enzymes of Clinical Importancemohamedmasry014No ratings yet
- Class-14 - Plasma Lipoproteins - EnzymesDocument39 pagesClass-14 - Plasma Lipoproteins - EnzymesAyi FurqonNo ratings yet
- Clinical Enzymology 5Document15 pagesClinical Enzymology 5Tooba SdNo ratings yet
- Bio-Chemistry 2 MarksDocument49 pagesBio-Chemistry 2 Marksdevilcobra68No ratings yet
- The Foundations of Structure:: Organelles, Cells and TissuesDocument52 pagesThe Foundations of Structure:: Organelles, Cells and TissuesNimit JindalNo ratings yet
- Instructor's Presentation-Lipids and LipoproteinsDocument43 pagesInstructor's Presentation-Lipids and Lipoproteinsjomel rondinaNo ratings yet
- PhysiologyDocument71 pagesPhysiologysalah.shashoraNo ratings yet
- BloodDocument76 pagesBloodKerby Dela Fuente Alison100% (1)
- 439 en Intro 1Document74 pages439 en Intro 1Omotosho DavidNo ratings yet
- Plasma EnzymesDocument13 pagesPlasma EnzymesBobskinnyNo ratings yet
- What Do You Need To Know About Organic Chemistry?Document25 pagesWhat Do You Need To Know About Organic Chemistry?YoAmoNYCNo ratings yet
- 1 Enzymes PDFDocument63 pages1 Enzymes PDFkunoz masrNo ratings yet
- Enzymes ClassificationDocument53 pagesEnzymes ClassificationAlok DhelditNo ratings yet
- Biologic AL: MoleculesDocument18 pagesBiologic AL: MoleculesDaniella Pasilbas SabacNo ratings yet
- Biological Molecules RealnarealDocument19 pagesBiological Molecules RealnarealOyenx Garrix SulatorioNo ratings yet
- Enzymology Medics 2011 5 (Compatibility Mode)Document8 pagesEnzymology Medics 2011 5 (Compatibility Mode)TennidoxNo ratings yet
- 15 Biochemistry Lecture - Enzymes 4Document42 pages15 Biochemistry Lecture - Enzymes 4AMIRA HELAYELNo ratings yet
- GB1 - S2 Proteins and Nucleic Acids - EnzymesDocument88 pagesGB1 - S2 Proteins and Nucleic Acids - EnzymesAndreau GranadaNo ratings yet
- KRV, PLAZMA, HEMATOPOEZADocument35 pagesKRV, PLAZMA, HEMATOPOEZASinisa RisticNo ratings yet
- IsoenzymesDocument10 pagesIsoenzymesاسلام خالدNo ratings yet
- Cardiovascular Physiology 4Document7 pagesCardiovascular Physiology 4lenoNo ratings yet
- Enzim Penyakit Jantung: Dr. Evi Kurniawaty, M.SCDocument28 pagesEnzim Penyakit Jantung: Dr. Evi Kurniawaty, M.SCRestu PamanggihNo ratings yet
- ProteinsDocument59 pagesProteinsCraig MitchellNo ratings yet
- Lecture 9 CVSDocument118 pagesLecture 9 CVSMuhammad Abbas WaliNo ratings yet
- Lecture 9 Physiology of BloodDocument125 pagesLecture 9 Physiology of BloodAhmed MohammedNo ratings yet
- CHAPTER 10 ANAPHY TransesDocument8 pagesCHAPTER 10 ANAPHY TransesHoly HaeinNo ratings yet
- Blood Physiology 2022Document116 pagesBlood Physiology 2022Gurmessa FekaduNo ratings yet
- BLOODDocument37 pagesBLOODelliot kafumukacheNo ratings yet
- Chapter 4 Blood Coagulation and Coagulation DisordersDocument27 pagesChapter 4 Blood Coagulation and Coagulation DisordersdaisysintszwaiNo ratings yet
- Enzymes in Diagnosis: Prof. Dr. N. Leyla Açan Hacettepe University Faculty of Medicine Department of Medical BiochemistryDocument4 pagesEnzymes in Diagnosis: Prof. Dr. N. Leyla Açan Hacettepe University Faculty of Medicine Department of Medical Biochemistryedh labNo ratings yet
- Gen - Bio Week 1Document62 pagesGen - Bio Week 1yahnie ًNo ratings yet
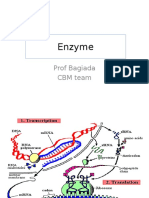
- Enzyme: Prof Bagiada CBM TeamDocument30 pagesEnzyme: Prof Bagiada CBM TeamPande Indra PremanaNo ratings yet
- BloodDocument32 pagesBloodPushpa AdhikariNo ratings yet
- Basics of Hematology Cell Counting: Agile - Affordable - AccurateDocument16 pagesBasics of Hematology Cell Counting: Agile - Affordable - AccurateYaser AlaniNo ratings yet
- Clinicalenzymology 220623200711 Deeb284aDocument8 pagesClinicalenzymology 220623200711 Deeb284aRahul guptaNo ratings yet
- ENDOCRINE FinalDocument68 pagesENDOCRINE FinalJerick Sevilla SearesNo ratings yet
- Fast Facts: Long-Chain Fatty Acid Oxidation Disorders for PatientsFrom EverandFast Facts: Long-Chain Fatty Acid Oxidation Disorders for PatientsNo ratings yet
- Fast Facts pour les patients: Les troubles d'oxydation des acides gras à chaîne longueFrom EverandFast Facts pour les patients: Les troubles d'oxydation des acides gras à chaîne longueNo ratings yet
- Tissue NematodesDocument30 pagesTissue NematodesGIST (Gujarat Institute of Science & Technology)No ratings yet
- J Deutsche Derma Gesell - 2020 - Gross - S2k Guidelines For The Diagnosis and Treatment of Herpes Zoster and PostherpeticDocument24 pagesJ Deutsche Derma Gesell - 2020 - Gross - S2k Guidelines For The Diagnosis and Treatment of Herpes Zoster and PostherpeticMUHAMMAD ALFANDARI GIBRANNo ratings yet
- Drugs in The Neonatal Unit: 1 Julia PettyDocument5 pagesDrugs in The Neonatal Unit: 1 Julia PettyMarjoNo ratings yet
- Case - Based Pathophysiology of Type 1 Hyperlipidemia - Familial HyperchylomicronemiaDocument1 pageCase - Based Pathophysiology of Type 1 Hyperlipidemia - Familial HyperchylomicronemiaMae Rose Charlene MendozaNo ratings yet
- Inclusiveness PPT AbenetW.Document152 pagesInclusiveness PPT AbenetW.sosina eseyew100% (1)
- Essay Questions For Medipro Offshore Medics Refresher CourseDocument5 pagesEssay Questions For Medipro Offshore Medics Refresher CourseRobert TurnerNo ratings yet
- Drug Study DRDocument3 pagesDrug Study DRGershom Perez AcaboNo ratings yet
- National Mental Health ProgrammeDocument36 pagesNational Mental Health ProgrammeSusmita Halder100% (1)
- Krok 1 - 2016 (General Medicine) - EneutronDocument58 pagesKrok 1 - 2016 (General Medicine) - EneutronHarsh NimavatNo ratings yet
- Department of Laboratory Medicine: Critical Care ServicesDocument2 pagesDepartment of Laboratory Medicine: Critical Care ServicesRTI ACTNo ratings yet
- Bone and Joint InfectionDocument43 pagesBone and Joint Infectionraheeg siddigNo ratings yet
- Tugas Eng KaniaDocument3 pagesTugas Eng KaniaKania Ishlah ZhafiraNo ratings yet
- Civ 1Document5 pagesCiv 1waseem555No ratings yet
- Complete List of Ms Thesis Sr. No. Students'Name Topic SupervisorDocument10 pagesComplete List of Ms Thesis Sr. No. Students'Name Topic SupervisorsanaNo ratings yet
- 18 "Bahay Kubo" Plants: Name: SingkamasDocument4 pages18 "Bahay Kubo" Plants: Name: SingkamasAria DomingoNo ratings yet
- Modular Instruction Manual FOR English 5 (Reading Remediation) S.Y.:2021-2022Document18 pagesModular Instruction Manual FOR English 5 (Reading Remediation) S.Y.:2021-2022Pandaog Al-hadzrieNo ratings yet
- Boccaccio-The Decameron - Short Intro - Excerpt - On The Black-DeathDocument6 pagesBoccaccio-The Decameron - Short Intro - Excerpt - On The Black-DeathBassem KamelNo ratings yet
- 1..report On Application of Ordinary Differential Equations in Analysing The Growth of DiseaseDocument5 pages1..report On Application of Ordinary Differential Equations in Analysing The Growth of Disease8103 Suyash DewanganNo ratings yet
- Unit 1 - Introduction To OSH Module 2: Osh Situation in The Global and Local LevelsDocument11 pagesUnit 1 - Introduction To OSH Module 2: Osh Situation in The Global and Local LevelsEustace TrifalgarNo ratings yet
- Blood Disorders LimmerEducationDocument1 pageBlood Disorders LimmerEducationrehaan662No ratings yet
- Ischemic Heart DiseaseDocument116 pagesIschemic Heart DiseaseAndrew OrlovNo ratings yet
- Heart Failure NCLEX QuestionsDocument5 pagesHeart Failure NCLEX QuestionsMelodia Turqueza GandezaNo ratings yet
- Visual Mnemonics Microbiology 40 Medical Mnemonics 41 40 Mar 4 2019 41 40 b07pgfhwm3 41 40 Independently Published 41Document68 pagesVisual Mnemonics Microbiology 40 Medical Mnemonics 41 40 Mar 4 2019 41 40 b07pgfhwm3 41 40 Independently Published 41Hisham Sabry100% (1)
- Suspecting and Diagnosing Arachnoiditis 2017Document22 pagesSuspecting and Diagnosing Arachnoiditis 2017Martha OktaviaNo ratings yet
- MAPEH (Music) : Quarter 3: Week 1 & 2Document23 pagesMAPEH (Music) : Quarter 3: Week 1 & 2Allinas NathalieNo ratings yet
- All Questions Med SurgDocument8 pagesAll Questions Med SurgShreya ShindeNo ratings yet
- IANs Presentation - Atrial Fibrillation (RMO Kerenga)Document26 pagesIANs Presentation - Atrial Fibrillation (RMO Kerenga)Samuel.MoriNo ratings yet