Download as pptx, pdf, or txt
You might also like
- ENDOSCoPIC SURGERY IN GYNAECOLOGYDocument64 pagesENDOSCoPIC SURGERY IN GYNAECOLOGYSurya TejaNo ratings yet
- Permanent Tunnel CatheterDocument52 pagesPermanent Tunnel CatheterJanice MuliadiNo ratings yet
- Intervetional Radiology PresentationDocument24 pagesIntervetional Radiology Presentationmalueth jacobNo ratings yet
- Central Venous Pressure BY: Ma. Victoria E. Martinez ER DepartmentDocument13 pagesCentral Venous Pressure BY: Ma. Victoria E. Martinez ER DepartmentMavic Martinez BuntalesNo ratings yet
- by Group C Bibin .C, Idrees .H, Shruti .IDocument36 pagesby Group C Bibin .C, Idrees .H, Shruti .IArie Angkiriwang0% (1)
- Intravenous CannulizationDocument78 pagesIntravenous CannulizationSandhya BasnetNo ratings yet
- Central Lines AND Arterial LinesDocument41 pagesCentral Lines AND Arterial LinesSalinKaurNo ratings yet
- Catheters and PortsDocument9 pagesCatheters and PortsPiyush AroraNo ratings yet
- A Procedural Guide To Midline InsertionDocument5 pagesA Procedural Guide To Midline InsertionLaurie RandleNo ratings yet
- Seldinger-Technique - Interventional RadiologyDocument13 pagesSeldinger-Technique - Interventional Radiologypntrdzj75wNo ratings yet
- Fundamentals of Pediatric Central Venous AccessDocument38 pagesFundamentals of Pediatric Central Venous AccesssirrfsNo ratings yet
- Angiography Materials-1: Lailatul Muqmiroh Prodi D-IV RadiologiDocument24 pagesAngiography Materials-1: Lailatul Muqmiroh Prodi D-IV RadiologiShelaErlanggaPutriNo ratings yet
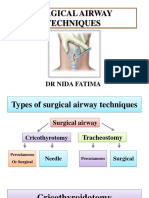
- Surgicalairwaytechniques 180526060828 PDFDocument72 pagesSurgicalairwaytechniques 180526060828 PDFWael ShamyNo ratings yet
- Anesthesia For ENT& Maxillofacial SurgeryDocument327 pagesAnesthesia For ENT& Maxillofacial SurgeryseetokindNo ratings yet
- Konsep Akses Vaskuler HD Temporary Dan Permanent Access Methods (Jugularis, Subklavia Dan Femoralis)Document74 pagesKonsep Akses Vaskuler HD Temporary Dan Permanent Access Methods (Jugularis, Subklavia Dan Femoralis)Ale PanjaitanNo ratings yet
- Venous and Arterial Catheterization: General PrinciplesDocument22 pagesVenous and Arterial Catheterization: General PrinciplesTibin JosephNo ratings yet
- Basics of Microvascular SurgeryDocument33 pagesBasics of Microvascular SurgeryPratikshya KothiaNo ratings yet
- Central Venous Access: Vic V. Vernenkar, D.O. Dept. of Surgery St. Barnabas HospitalDocument29 pagesCentral Venous Access: Vic V. Vernenkar, D.O. Dept. of Surgery St. Barnabas HospitalLouis FortunatoNo ratings yet
- RadiologyDocument46 pagesRadiologyitho23100% (1)
- Coronary AngiogramDocument58 pagesCoronary AngiogramEllaine Jennel100% (3)
- Central Venous Access: RSUD Duren SawitDocument48 pagesCentral Venous Access: RSUD Duren SawitMonica HerdiatiNo ratings yet
- PhlebotomyDocument62 pagesPhlebotomyKristinaNo ratings yet
- CVP Line CareDocument37 pagesCVP Line CareArvindJoshiNo ratings yet
- LP 8 Orif FemurDocument42 pagesLP 8 Orif FemurdaliaberseNo ratings yet
- Central Venous Catheterization: Maret 2021Document39 pagesCentral Venous Catheterization: Maret 2021Rudy SiahaanNo ratings yet
- LaserDocument17 pagesLasergeeth074No ratings yet
- ThyroidectomyDocument41 pagesThyroidectomyNguyen Thanh HuyenNo ratings yet
- Assessment Pre Op Dan USG - DR MursidDocument27 pagesAssessment Pre Op Dan USG - DR MursidSyarif MalawatNo ratings yet
- Intro To Specialized Nursing ProceduresDocument156 pagesIntro To Specialized Nursing ProceduresJimmy MainaNo ratings yet
- Angiographic ThoracalisDocument22 pagesAngiographic ThoracalisermaendahNo ratings yet
- Access SheathDocument22 pagesAccess SheathSri HariNo ratings yet
- CanulationDocument21 pagesCanulationJason Liando100% (1)
- Endoscopy Layth Mahmoud HussainDocument15 pagesEndoscopy Layth Mahmoud Hussainnoor deenNo ratings yet
- Emergency Procedures: - Defibrillation in CPRDocument20 pagesEmergency Procedures: - Defibrillation in CPRDuy Phương NguyễnNo ratings yet
- IV TherapyDocument39 pagesIV TherapyChannelGNo ratings yet
- Endoscopy in Neurosurgery SeminarDocument85 pagesEndoscopy in Neurosurgery SeminarRamjas ChoudharyNo ratings yet
- Peripheral Venous AccessDocument23 pagesPeripheral Venous AccessIan RochaNo ratings yet
- (RADIO 250) LEC 08 Introduction To Interventional RadiologyDocument4 pages(RADIO 250) LEC 08 Introduction To Interventional RadiologyWilliam PinzonNo ratings yet
- CH 2 SuctioningDocument90 pagesCH 2 SuctioningMaherNo ratings yet
- Vascular Surgical ProceduresDocument10 pagesVascular Surgical Proceduresafeekhan0007No ratings yet
- ProceduresDocument23 pagesProceduresivan KeshariNo ratings yet
- Central Venous LinesDocument34 pagesCentral Venous LinesManny TrujilloNo ratings yet
- Saphenousveinharvestingpresentation 150824151458 Lva1 App6892Document46 pagesSaphenousveinharvestingpresentation 150824151458 Lva1 App6892Maryasi PanjaitanNo ratings yet
- O o o o o o o o o o o oDocument9 pagesO o o o o o o o o o o oAshish PandeyNo ratings yet
- Iv Cannulation: Dr. Carla O. Pandrya, Span FK UphDocument21 pagesIv Cannulation: Dr. Carla O. Pandrya, Span FK UphCandice LavigneNo ratings yet
- Needle Cricothyroidotomy 2 - Hatem AlsrourDocument32 pagesNeedle Cricothyroidotomy 2 - Hatem Alsrourhatem alsrour100% (3)
- Vascular AccessDocument48 pagesVascular AccessJason Samuel Fredrick80% (5)
- Subclavian Centraline ManualDocument12 pagesSubclavian Centraline Manualqc.carcinovaNo ratings yet
- Akses Vaskular Yang Aman Untuk HD - DR Dedi A ZaelaniDocument25 pagesAkses Vaskular Yang Aman Untuk HD - DR Dedi A ZaelaniSyarif MalawatNo ratings yet
- Insertion and Operation of IABP-1Document10 pagesInsertion and Operation of IABP-1Atia KiranNo ratings yet
- Angioplasty and Vascular StentingDocument8 pagesAngioplasty and Vascular Stentingrajnishpathak648No ratings yet
- CricothyroidotomyDocument41 pagesCricothyroidotomyNur SusiawantyNo ratings yet
- SuctioningDocument28 pagesSuctioningRalph Emerson RatonNo ratings yet
- Intravenous FluidsDocument3 pagesIntravenous FluidsKristine Artes AguilarNo ratings yet
- Catheters and Guide Wires: Presenter: Omkar Gaonkar Course: M.SC., Mit 2 SEM Moderator: Kayalvizhi R DATE:26/03/2019Document42 pagesCatheters and Guide Wires: Presenter: Omkar Gaonkar Course: M.SC., Mit 2 SEM Moderator: Kayalvizhi R DATE:26/03/2019Omkar GaonkarNo ratings yet
- Harvesting SVGDocument26 pagesHarvesting SVGSamuel Hotma Rotua Sinaga100% (1)
- AngioplastyDocument29 pagesAngioplastyaramatharaNo ratings yet
- Basic Invasive ProceduresDocument39 pagesBasic Invasive ProceduresLucas AresNo ratings yet
- Cardiac Surgical Operative AtlasFrom EverandCardiac Surgical Operative AtlasThorsten WahlersNo ratings yet
- CT ProtocolsDocument62 pagesCT ProtocolssanyengereNo ratings yet
- Sample Bottle CleaningDocument6 pagesSample Bottle CleaningsanyengereNo ratings yet
- Imaging Assignment 01Document13 pagesImaging Assignment 01sanyengereNo ratings yet
- Special Needs FinalDocument46 pagesSpecial Needs FinalsanyengereNo ratings yet
- EquipDocument40 pagesEquipsanyengereNo ratings yet
- 297 FullDocument7 pages297 FullsanyengereNo ratings yet
- Radiology Instrumentation: Mahidol UniversityDocument281 pagesRadiology Instrumentation: Mahidol UniversitysanyengereNo ratings yet
- 44b2967d-fdc0-4db7-8674-d1fba260d1d4Document3 pages44b2967d-fdc0-4db7-8674-d1fba260d1d4sanyengereNo ratings yet
- MUCLecture 2021 112449616Document7 pagesMUCLecture 2021 112449616sanyengereNo ratings yet
- Final Equipment AssignmentDocument14 pagesFinal Equipment AssignmentsanyengereNo ratings yet
- Data Acquisition-1Document23 pagesData Acquisition-1sanyengereNo ratings yet
- Radiation Dosimetry Presentation-2Document49 pagesRadiation Dosimetry Presentation-2sanyengereNo ratings yet
- Intrinsic Flood-Field Uniformity EvaluationDocument10 pagesIntrinsic Flood-Field Uniformity EvaluationsanyengereNo ratings yet
- Edited CT Pres GRP 3Document37 pagesEdited CT Pres GRP 3sanyengereNo ratings yet
- Introduction To Contrast InjectorsDocument22 pagesIntroduction To Contrast InjectorssanyengereNo ratings yet
- Extraoral 2018Document14 pagesExtraoral 2018sanyengereNo ratings yet
- BETHEL RARAMI Big Data AssignmentDocument11 pagesBETHEL RARAMI Big Data AssignmentsanyengereNo ratings yet
- Rehabilitation Care of Women With PCOS ADocument3 pagesRehabilitation Care of Women With PCOS AsanyengereNo ratings yet
- CT GenerationsDocument3 pagesCT GenerationssanyengereNo ratings yet
- 2024 Market Basket AnalysisDocument30 pages2024 Market Basket AnalysissanyengereNo ratings yet
- MUCLecture 2022 56897Document8 pagesMUCLecture 2022 56897sanyengereNo ratings yet
- Hit 2203-Big Data & Data Analytics - Lecture - 3Document10 pagesHit 2203-Big Data & Data Analytics - Lecture - 3sanyengereNo ratings yet
- Fractura de Un Pilar PPFDocument3 pagesFractura de Un Pilar PPFCarlos NaupariNo ratings yet
- Systemic Mycoses: Blastomyces DermatitidisDocument12 pagesSystemic Mycoses: Blastomyces Dermatitidisredz_ekg619No ratings yet
- Interface Such As A Zoo, Farm or Animal Market.: CarriersDocument3 pagesInterface Such As A Zoo, Farm or Animal Market.: CarriersGuga MamiseishviliNo ratings yet
- Immediate Dental Implant 1Document13 pagesImmediate Dental Implant 1alkhalijia dentalNo ratings yet
- Spek Ven Avea Full ClioDocument3 pagesSpek Ven Avea Full ClioRinawatiNo ratings yet
- WOC CKD NewDocument1 pageWOC CKD Newaris novenNo ratings yet
- Hospital Transfusion Committee Manual-20170508Document6 pagesHospital Transfusion Committee Manual-20170508ACEDD BSF LABNo ratings yet
- Cardiac Embryology 1Document18 pagesCardiac Embryology 1Natalia IhalauwNo ratings yet
- Thesis ProtocolDocument7 pagesThesis ProtocolhoneyworksNo ratings yet
- Ovarian Cancer: Presented By-Vaishnavi Saxena B.SC Nursing 3 YearDocument17 pagesOvarian Cancer: Presented By-Vaishnavi Saxena B.SC Nursing 3 YearVaishnavi Saxena100% (2)
- 21-4019 R210463 Add05-22 2023-09Document2 pages21-4019 R210463 Add05-22 2023-09Mima HamiciNo ratings yet
- Dapaglifozin A Review in Type 2 DiabetesDocument12 pagesDapaglifozin A Review in Type 2 DiabetesDaniel CastanNo ratings yet
- Puritan Bennett 980 Ventilator Clinical Applications Lesson Plan PresentationDocument102 pagesPuritan Bennett 980 Ventilator Clinical Applications Lesson Plan Presentationbilal ahmad100% (1)
- Mastitis Prevention and TreatmentDocument52 pagesMastitis Prevention and TreatmentIbrahim Elkamash0% (1)
- Adv Vs DisadvDocument6 pagesAdv Vs DisadvD BNo ratings yet
- Cone CuttingDocument7 pagesCone CuttingAnonymous aoKk1TSDNo ratings yet
- Biliary Cast Syndrome in Portal Hypertensive Biliopathy: Direct Cholangioscopic Findings and Endoscopic Therapy With Metal StentDocument3 pagesBiliary Cast Syndrome in Portal Hypertensive Biliopathy: Direct Cholangioscopic Findings and Endoscopic Therapy With Metal StentMarcelo CalossoNo ratings yet
- RTPCRDocument2 pagesRTPCRAaqib KhanNo ratings yet
- DEAR YIN LING 2nd - CompressedDocument282 pagesDEAR YIN LING 2nd - CompressedSunn Ren TeeNo ratings yet
- Mix Questions PDFDocument40 pagesMix Questions PDFZazo RawashdehNo ratings yet
- Part 2 Evidence Evaluation PDFDocument8 pagesPart 2 Evidence Evaluation PDFNurul RafahNo ratings yet
- Radiologic TechnologistDocument4 pagesRadiologic Technologistapi-78781330No ratings yet
- Lec 8 Ulcerative Vesicular & Bullous LesionsDocument6 pagesLec 8 Ulcerative Vesicular & Bullous LesionsAbd 9961No ratings yet
- Resume 2023 Misty Armstrong Mar 17Document3 pagesResume 2023 Misty Armstrong Mar 17api-706914975No ratings yet
- Aace - Ace - 2016 - Comprehensive Clinical Practice Guidelines For Medical Care of Patients With ObesityDocument203 pagesAace - Ace - 2016 - Comprehensive Clinical Practice Guidelines For Medical Care of Patients With ObesityLintang AdhiNo ratings yet
- NadlfdiskshcDocument7 pagesNadlfdiskshcIndra PratamaNo ratings yet
- Monocyte Activation Test A New Pharmacoepial Quality Control Test For Pyrogens - A ReviewDocument11 pagesMonocyte Activation Test A New Pharmacoepial Quality Control Test For Pyrogens - A Reviewscientific trainingNo ratings yet
- Hasler 2004 Prochaska Eating DisordersDocument7 pagesHasler 2004 Prochaska Eating Disordersandra_coralia9112No ratings yet
- Test Report Gupta DiagnosisDocument17 pagesTest Report Gupta Diagnosisdrblgupta1973100% (1)
- Alzheimers Facts and FiguresDocument108 pagesAlzheimers Facts and FiguresMayco BiasibettiNo ratings yet