Download as pptx, pdf, or txt
You might also like
- Top 300 Drugs Pocket Reference Guide (2021 Edition)From EverandTop 300 Drugs Pocket Reference Guide (2021 Edition)Rating: 5 out of 5 stars5/5 (1)
- Pharm Drug ListDocument17 pagesPharm Drug Listanon_523534678No ratings yet
- Antibiotics - Compleate ClassificationDocument2 pagesAntibiotics - Compleate ClassificationNeal Gupta83% (12)
- Revision Guide Made Simple For Pharmacy Technicians 2nd EditionFrom EverandRevision Guide Made Simple For Pharmacy Technicians 2nd EditionNo ratings yet
- ESMO Examination Answers To Trial QuestionsDocument32 pagesESMO Examination Answers To Trial QuestionsVlad Croitoru100% (1)
- Harrison TablesDocument163 pagesHarrison Tablesfrancieudo1No ratings yet
- Cancer Foye's Principles of Medicinal Chemistry-1219-1286Document68 pagesCancer Foye's Principles of Medicinal Chemistry-1219-1286minhxuan100% (3)
- Tomotherapy PresentationDocument26 pagesTomotherapy Presentationapi-24740282767% (3)
- Anti Cancer DrugsDocument3 pagesAnti Cancer DrugsDheaNo ratings yet
- Chemotherapeutic FamiliesDocument6 pagesChemotherapeutic FamiliesRice CookerNo ratings yet
- Drugs For Cancer TherapyDocument102 pagesDrugs For Cancer TherapyPUTRI CHRISTIANTI TELAUMBANUA 1No ratings yet
- Anti Cancer ChemotherapyDocument103 pagesAnti Cancer ChemotherapyMourian AmanNo ratings yet
- AnticancerDocument27 pagesAnticancerLoreine Jane ClaritoNo ratings yet
- DrugsDocument3 pagesDrugsxsuilujxNo ratings yet
- Kontraindikasi Obat MGDocument2 pagesKontraindikasi Obat MGMuhammad Naqvi Al FarisiNo ratings yet
- AntibioticsDocument5 pagesAntibioticsLaureece Salm ApduhanNo ratings yet
- Cancer Drugs Pharmacology TableDocument11 pagesCancer Drugs Pharmacology TableAmin InanNo ratings yet
- Pharmacology TableDocument9 pagesPharmacology TableMaryam KhushbakhatNo ratings yet
- Fixed Drug EruptionsDocument16 pagesFixed Drug EruptionsAnonymous 2BC7omLaWCNo ratings yet
- Mission & Vision: ProductsDocument5 pagesMission & Vision: Productsradheshyam882No ratings yet
- Chemotherapy ToxicityDocument37 pagesChemotherapy ToxicityCarlos Eduardo Cadu100% (1)
- Review Handouts For Medical Pharmacology PDFDocument21 pagesReview Handouts For Medical Pharmacology PDFAndres F. TorresNo ratings yet
- Abvd Beacopp Stanford V Mopp: Chlvpp/EvaDocument4 pagesAbvd Beacopp Stanford V Mopp: Chlvpp/EvapallavberiNo ratings yet
- Pharmacology: Andrea Q. Carigma, R.PH., M.D. May 2015Document46 pagesPharmacology: Andrea Q. Carigma, R.PH., M.D. May 2015Leonibel GhloeNo ratings yet
- KU PPB 423 Lesson 2 - Introduction To Antineoplastic AgentsDocument9 pagesKU PPB 423 Lesson 2 - Introduction To Antineoplastic AgentsPharmswipe KenyaNo ratings yet
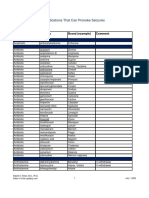
- Medications That Can Provoke Seizures: Main Usage Generic Brand (Example) CommentDocument6 pagesMedications That Can Provoke Seizures: Main Usage Generic Brand (Example) CommentKrasna VolkNo ratings yet
- Review Handouts For Medical Pharmacology: Terriann Crisp, PH.DDocument28 pagesReview Handouts For Medical Pharmacology: Terriann Crisp, PH.Dmus zaharaNo ratings yet
- Veterinary Drugs - Usage, Dosage, Species, and More.Document15 pagesVeterinary Drugs - Usage, Dosage, Species, and More.cocopandanenakNo ratings yet
- 3 - Clinical Pharmacology of ChemotherapyDocument111 pages3 - Clinical Pharmacology of ChemotherapyChinIsiangSocitoNo ratings yet
- Anticancer DrugsDocument33 pagesAnticancer Drugsalihyderabro166No ratings yet
- Classification of Drugs PDFDocument15 pagesClassification of Drugs PDFmuhammad ihtisham ul hassanNo ratings yet
- Pharmayield: Must Know Pharmacology NotesDocument2 pagesPharmayield: Must Know Pharmacology NotesBianca Desiree VergaraNo ratings yet
- Antineoplastic AgentsDocument2 pagesAntineoplastic AgentsgargabhinabNo ratings yet
- Cology 3Document6 pagesCology 3arsalankhan8626No ratings yet
- Drugs Cards 208Document11 pagesDrugs Cards 208SOOOS94100% (3)
- Pemberian Obat Pada Kelainan Fungsi HeparDocument21 pagesPemberian Obat Pada Kelainan Fungsi Heparari rujatiNo ratings yet
- Antiparasitic & Antifungal DrugsDocument30 pagesAntiparasitic & Antifungal DrugsAbdullah AlkharsNo ratings yet
- Anticancer Drugs: Nur PermatasariDocument67 pagesAnticancer Drugs: Nur Permatasari0910720085No ratings yet
- PharmaDocument60 pagesPharmash99sharedNo ratings yet
- 909-Hazardous Drugs Table - EviqDocument9 pages909-Hazardous Drugs Table - EviqMd Al AminNo ratings yet
- Obat-Obat Pada Mata: Jimmy PosangiDocument31 pagesObat-Obat Pada Mata: Jimmy Posangimuhammad satriNo ratings yet
- 100 DrugsDocument3 pages100 Drugsp0theads015No ratings yet
- FungalDocument19 pagesFungalSparks Francis EzikaNo ratings yet
- Obat-Obat Pada Mata: Jimmy PosangiDocument33 pagesObat-Obat Pada Mata: Jimmy PosangiNovita NoviNo ratings yet
- Pharmacology ReviewDocument172 pagesPharmacology ReviewJan Patrick Arrieta100% (1)
- 21 Anti-NeoplasticDocument11 pages21 Anti-NeoplasticMuhammad Amin BozdarNo ratings yet
- Drug of Choice List PDFDocument2 pagesDrug of Choice List PDFHeceas Heceas0% (1)
- Therapi Antibiotik 1Document7 pagesTherapi Antibiotik 1Muhammad RaflyNo ratings yet
- Common Drugs - Med WardDocument1 pageCommon Drugs - Med WardRohannah D. MalawadNo ratings yet
- Antibiotics, The Basics: Classification of Veterinary AntibioticsDocument2 pagesAntibiotics, The Basics: Classification of Veterinary Antibioticsgalihja100% (1)
- PHARMACOLOGY HighlightedDocument37 pagesPHARMACOLOGY HighlightedEmeroot RootNo ratings yet
- Pharm C Exam 10 Drug ListDocument2 pagesPharm C Exam 10 Drug ListVokdadaNo ratings yet
- Drugs PharmaDocument3 pagesDrugs PharmaCheenee AmilbangsaNo ratings yet
- Toxicology and AntidoteDocument6 pagesToxicology and AntidoteVikash KushwahaNo ratings yet
- NCLEX Pharmacology: Mary Whyte Marshall, MSN, RN, BCDocument58 pagesNCLEX Pharmacology: Mary Whyte Marshall, MSN, RN, BCPeiling LiangNo ratings yet
- Lange Smart Charts: Pharmacology, 2e Pharmacologic SuffixesDocument2 pagesLange Smart Charts: Pharmacology, 2e Pharmacologic SuffixesSolNo ratings yet
- Anti-Tb Drugs: Moderator-Dr - Sheik Mohammed Raja M - D Chief DR - Senthamaraimd., M5 UnitDocument34 pagesAnti-Tb Drugs: Moderator-Dr - Sheik Mohammed Raja M - D Chief DR - Senthamaraimd., M5 UnitSivaramkumar JNo ratings yet
- Poison & Antidote Chart IWK Regional Poison Cen PDFDocument1 pagePoison & Antidote Chart IWK Regional Poison Cen PDFdeeptiNo ratings yet
- Revision Guide Made Simple For Pharmacy Technicians 3rd Edition: 3rd EditionFrom EverandRevision Guide Made Simple For Pharmacy Technicians 3rd Edition: 3rd EditionNo ratings yet
- Basic Pharmacology And Drug Calculations [Practice Questions And Answers]From EverandBasic Pharmacology And Drug Calculations [Practice Questions And Answers]Rating: 4 out of 5 stars4/5 (1)
- Revision Guide Made Simple For Pharmacy Technicians - PTCB: 4th EditionFrom EverandRevision Guide Made Simple For Pharmacy Technicians - PTCB: 4th EditionNo ratings yet
- Learn Pharmacology Using Classes Clinical Placement GuideFrom EverandLearn Pharmacology Using Classes Clinical Placement GuideNo ratings yet
- School of Nursing & Midwifery Department of Emergency & Critical Care NursingDocument16 pagesSchool of Nursing & Midwifery Department of Emergency & Critical Care NursingTilaye GebruNo ratings yet
- School of Nursing & Midwifery Department of Emergency & Critical Care NursingDocument29 pagesSchool of Nursing & Midwifery Department of Emergency & Critical Care NursingTilaye GebruNo ratings yet
- FeverDocument27 pagesFeverTilaye GebruNo ratings yet
- New CDDCDocument44 pagesNew CDDCTilaye GebruNo ratings yet
- Safehandling of Cytotoxic Drugs 2020Document56 pagesSafehandling of Cytotoxic Drugs 2020Tilaye GebruNo ratings yet
- Pediatrics MlignancyDocument112 pagesPediatrics MlignancyTilaye GebruNo ratings yet
- 10 Pharmaceutical Calculations inDocument27 pages10 Pharmaceutical Calculations inTilaye GebruNo ratings yet
- Stability and Shelf Life of Drugs 2020Document23 pagesStability and Shelf Life of Drugs 2020Tilaye GebruNo ratings yet
- Children CancerDocument6 pagesChildren CancerTilaye GebruNo ratings yet
- OncoEmer 2Document9 pagesOncoEmer 2Tilaye GebruNo ratings yet
- Childhood Cancer, Incidence, Survival and MortalityDocument26 pagesChildhood Cancer, Incidence, Survival and MortalityTilaye GebruNo ratings yet
- Steps Involved in Clinical Radiation TherapyDocument6 pagesSteps Involved in Clinical Radiation TherapyvorisNo ratings yet
- Z - Ding Cyberknife Vs LinacDocument26 pagesZ - Ding Cyberknife Vs Linacraheel252No ratings yet
- Monday KordeDocument19 pagesMonday KordeNational Press FoundationNo ratings yet
- Principles of Cancer TreatmentDocument7 pagesPrinciples of Cancer TreatmentRenatoCosmeGalvanJuniorNo ratings yet
- 2019E 11 - Adjuvant Cytotoxic and Targeted TherapyDocument15 pages2019E 11 - Adjuvant Cytotoxic and Targeted Therapyrusgal8992No ratings yet
- 10 Intraoperative RadiotherapyDocument11 pages10 Intraoperative RadiotherapyDgek LondonNo ratings yet
- Pivas 2018Document46 pagesPivas 2018Denny PaatNo ratings yet
- Medicamentos Antineoplásicos 27.08.2018Document6 pagesMedicamentos Antineoplásicos 27.08.2018Vagner CardosoNo ratings yet
- JR Kemo TitaDocument21 pagesJR Kemo TitaTitaPuspitasariNo ratings yet
- Linfoma de Hodgkin: Enfermedad en Relapso/RecaídaDocument31 pagesLinfoma de Hodgkin: Enfermedad en Relapso/RecaídaDANIEL JAIR ENRIQUEZ VERANo ratings yet
- Medicament OsDocument8 pagesMedicament OsAlfredo SalarNo ratings yet
- Atezolizumab Plus Chemo Improves PFS in Frontline Squamous NSCLCDocument18 pagesAtezolizumab Plus Chemo Improves PFS in Frontline Squamous NSCLC29milce17No ratings yet
- ImmunotherapyDocument2 pagesImmunotherapymaty.visintainerNo ratings yet
- ISODOSEDocument2 pagesISODOSEArun AdhikariNo ratings yet
- Curs VII - Terapii SistemiceDocument229 pagesCurs VII - Terapii SistemiceHucay EduardNo ratings yet
- SARMS Powders Prices - David FromDocument1 pageSARMS Powders Prices - David FromOld World OrderNo ratings yet
- Bfco193 Radiotherapy Dose Fractionation Third-Edition-Lung-Cancer 0Document9 pagesBfco193 Radiotherapy Dose Fractionation Third-Edition-Lung-Cancer 0Dwi PutriNo ratings yet
- Oncology Scope of ServicesDocument2 pagesOncology Scope of ServicesJaisurya SharmaNo ratings yet
- Some of The Oncology Best-Sellers Silver Pharma TurkeyDocument2 pagesSome of The Oncology Best-Sellers Silver Pharma TurkeyArchil PochkhuaNo ratings yet
- Presentation Brain Metastasis CancerDocument26 pagesPresentation Brain Metastasis CancerAnugrah WulanNo ratings yet
- ChemotherapyDocument1 pageChemotherapyGerardLum100% (2)
- Adjuvant and Neoadjuvant ChemotherapyDocument22 pagesAdjuvant and Neoadjuvant Chemotherapyprabushankar7No ratings yet
- Anticancer DrugsDocument117 pagesAnticancer DrugsKishore Chandra Korada100% (2)
- Accure Labs Pvt. Products PDFDocument2 pagesAccure Labs Pvt. Products PDFYoussef KaidNo ratings yet
- The Breast Journal - 2021 - Al Naqqash - Trastuzumab Beyond Progression in HER2 Positive Metastatic Breast CancerDocument3 pagesThe Breast Journal - 2021 - Al Naqqash - Trastuzumab Beyond Progression in HER2 Positive Metastatic Breast CancerhamzaNo ratings yet
- Production of Affordable ChemotherapyDocument27 pagesProduction of Affordable ChemotherapyIndonesian Journal of CancerNo ratings yet
- Kegunaan LinacDocument2 pagesKegunaan LinaccicichepiNo ratings yet
- Neoadjuvant Treatment Strategies For HER2 Positive Breast Cancer: Cost Effectiveness and Quality of Life OutcomesDocument9 pagesNeoadjuvant Treatment Strategies For HER2 Positive Breast Cancer: Cost Effectiveness and Quality of Life Outcomesfaris nagibNo ratings yet

























































![Basic Pharmacology And Drug Calculations [Practice Questions And Answers]](https://imgv2-1-f.scribdassets.com/img/word_document/475660044/149x198/2c7fc45015/1691161640?v=1)