
Multiplepregnancy 131213091755 Phpapp02
Multiplepregnancy 131213091755 Phpapp02
You might also like
- Pharmacology For Nurses Third Canadian Edition 3Rd Edition Full ChapterDocument41 pagesPharmacology For Nurses Third Canadian Edition 3Rd Edition Full Chaptermuriel.moreno949100% (26)
- Case Studies Accommodations2Document4 pagesCase Studies Accommodations2api-325828984No ratings yet
- Understanding ViolenceDocument232 pagesUnderstanding ViolenceBenchea Silvestru100% (6)
- Multiple Pregnancy - PPTX Md3Document41 pagesMultiple Pregnancy - PPTX Md3Brother George100% (1)
- Multiple Pregnancy LectureDocument33 pagesMultiple Pregnancy Lecturefarid_nchep100% (1)
- Roles and Responsibilities of Local DRRM OfficersDocument22 pagesRoles and Responsibilities of Local DRRM OfficersErnan Baldomero92% (12)
- (BS 1133-6.1-1991) - Packaging Code. Protection of Metal Surfaces Against Corrosion During Transport and Storage. Cleaning and Drying of Metal SurfacesDocument34 pages(BS 1133-6.1-1991) - Packaging Code. Protection of Metal Surfaces Against Corrosion During Transport and Storage. Cleaning and Drying of Metal SurfacesTowkir AhmmadNo ratings yet
- Global Natural Source Vitamin E Market - 2018 To 2024 (Tocopherols and Tocotrienols)Document5 pagesGlobal Natural Source Vitamin E Market - 2018 To 2024 (Tocopherols and Tocotrienols)Industry Experts, Inc.No ratings yet
- Multiple Pregnancy 1Document56 pagesMultiple Pregnancy 1angel panchalNo ratings yet
- 4th Year Multiple PregnancyDocument57 pages4th Year Multiple PregnancyKingsley Calex100% (2)
- Multiple Pregnancy1Document57 pagesMultiple Pregnancy1Muhammad Abeesh100% (1)
- Multiple GestationDocument24 pagesMultiple GestationNura BamaiyiNo ratings yet
- MK Multiple Gestation (OBGY)Document16 pagesMK Multiple Gestation (OBGY)Moses Jr KazevuNo ratings yet
- Multiple Pregnancy: Fahad ZakwanDocument60 pagesMultiple Pregnancy: Fahad Zakwanhaisuresh100% (1)
- Multiple Pregnancy: Prof Uma SinghDocument53 pagesMultiple Pregnancy: Prof Uma Singhgeng gengNo ratings yet
- Multiple Gestation: Dr. Hotma Partogi Pasaribu Spog Sub Division of Fetomaternal Medical Faculty - Usu Rsham - RSPM MedanDocument47 pagesMultiple Gestation: Dr. Hotma Partogi Pasaribu Spog Sub Division of Fetomaternal Medical Faculty - Usu Rsham - RSPM MedanSyarifah KhamsiawanNo ratings yet
- Multifetal Pregnancy: Dr. Hani MahdiDocument59 pagesMultifetal Pregnancy: Dr. Hani MahdiArwa QishtaNo ratings yet
- Multifetal Pregnancy: Amr Nadim, MDDocument36 pagesMultifetal Pregnancy: Amr Nadim, MDsharenNo ratings yet
- Multiple Pregnancy: Prof Uma SinghDocument53 pagesMultiple Pregnancy: Prof Uma Singhpok yeahNo ratings yet
- Multiple Pregnancy: Kevin AndrewDocument36 pagesMultiple Pregnancy: Kevin AndrewintanpurnNo ratings yet
- Twin TDocument30 pagesTwin TmaezuNo ratings yet
- Multiple Pregnancy HatimDocument22 pagesMultiple Pregnancy HatimHatim AbdellateifNo ratings yet
- 2 Multiple - Pregnancy - Lecture 2018Document48 pages2 Multiple - Pregnancy - Lecture 2018abrhamNo ratings yet
- Multiple Births - Embryology of TwinningDocument24 pagesMultiple Births - Embryology of TwinningtawandarukwavamadisonNo ratings yet
- Multiple PregnanciesDocument36 pagesMultiple PregnanciesBasudev ch100% (1)
- Multiple PXDocument46 pagesMultiple PXBetelhem EjiguNo ratings yet
- A Multiple Birth Occurs When More ThanDocument16 pagesA Multiple Birth Occurs When More ThanVaibhav BhatiaNo ratings yet
- Breech PresentationDocument16 pagesBreech Presentationkhadija falakNo ratings yet
- Malpresntation, Malposition and Breech Presentation 2022 BayisaDocument45 pagesMalpresntation, Malposition and Breech Presentation 2022 BayisaHile ShaNo ratings yet
- Multiple PregnancyDocument52 pagesMultiple Pregnancyazida90100% (4)
- Multiple Fetal Pregnancy: Riza SufriadiDocument20 pagesMultiple Fetal Pregnancy: Riza SufriadiRizur SufisonNo ratings yet
- Multiple PregnancyDocument83 pagesMultiple PregnancyAmna MaqboolNo ratings yet
- Multiple PregnancyDocument32 pagesMultiple PregnancyRebbeccah NafulaNo ratings yet
- Multiple PregnancyDocument28 pagesMultiple PregnancyFarxan Da Napolian BwoyNo ratings yet
- Multiplepregnancy 100515015745 Phpapp01Document29 pagesMultiplepregnancy 100515015745 Phpapp01haisureshNo ratings yet
- Multifetal PregnancyDocument68 pagesMultifetal PregnancyHoque Mohammed Newaz ShorifulNo ratings yet
- SEMINAR ON MULTIPLE PREGNANCY ContentDocument21 pagesSEMINAR ON MULTIPLE PREGNANCY ContentMonika shankar0% (1)
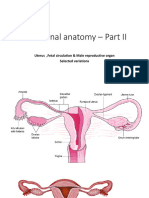
- Functional Anatomy - Part II: Uterus, Fetal Circulation & Male Reproductive Organ Selected VariationsDocument69 pagesFunctional Anatomy - Part II: Uterus, Fetal Circulation & Male Reproductive Organ Selected Variationshfkxbbbty2No ratings yet
- Multiple Pregnancy 2008Document61 pagesMultiple Pregnancy 2008Dagnachew kasayeNo ratings yet
- Prenatal DevelopmentDocument30 pagesPrenatal DevelopmentAnu ChauhanNo ratings yet
- Twin Pregnancy: Dr. Girishankar Samarasam Supervised By: DR Rathimalar DR Mohd Faizal Bin Nor AzmiDocument56 pagesTwin Pregnancy: Dr. Girishankar Samarasam Supervised By: DR Rathimalar DR Mohd Faizal Bin Nor AzmiShre RanjithamNo ratings yet
- Twins: SupervisorDocument10 pagesTwins: Supervisorكيرلس مجدىNo ratings yet
- Understanding Multiple Pregnancy: Maternal & Fetal ComplicationsDocument69 pagesUnderstanding Multiple Pregnancy: Maternal & Fetal Complications966342No ratings yet
- Multiple Pregnancy: Dr. A. Farid Abdullah, SP - OG, M.KesDocument33 pagesMultiple Pregnancy: Dr. A. Farid Abdullah, SP - OG, M.KesAndi Farid A100% (1)
- Antepartum Hemorrhage: Placental CausesDocument9 pagesAntepartum Hemorrhage: Placental CausesadiNo ratings yet
- Multiple PregnancyDocument71 pagesMultiple PregnancyAndre PutraNo ratings yet
- Abnormal Lie: - Abnormal Lie Consists of Two Types: Transverse Lie Oblique LieDocument21 pagesAbnormal Lie: - Abnormal Lie Consists of Two Types: Transverse Lie Oblique LieBharat ThapaNo ratings yet
- علاااءDocument21 pagesعلاااءalaazeez2000No ratings yet
- Kehamilan Ganda1Document54 pagesKehamilan Ganda1rizmaNo ratings yet
- Book ReportDocument69 pagesBook ReportBarangay MotibotNo ratings yet
- Multiple PregnancyDocument23 pagesMultiple Pregnancy19 KomalNo ratings yet
- Multiple PregnancyDocument20 pagesMultiple PregnancyNurul Fahmiza TumiranNo ratings yet
- Multifetal PintDocument51 pagesMultifetal PintLeikkaNo ratings yet
- Muhammad Redzwan Bin Abdullah: 081303583 Batch 25 Group E2Document66 pagesMuhammad Redzwan Bin Abdullah: 081303583 Batch 25 Group E2Suyajna JoshiNo ratings yet
- Abnormal Labor Lec 1Document34 pagesAbnormal Labor Lec 1Zahraa HasanNo ratings yet
- Multiple Pregnancy: Nirav Hitesh Kumar ValandDocument28 pagesMultiple Pregnancy: Nirav Hitesh Kumar ValandNirav SharmaNo ratings yet
- 08 Twins Birth DiagnosticDocument6 pages08 Twins Birth DiagnosticElliotPianoNo ratings yet
- Placental PathologyDocument465 pagesPlacental PathologyOana Roxana PuscasNo ratings yet
- Multiple PregnancesssssDocument29 pagesMultiple PregnancesssssNajjemba ShanitahNo ratings yet
- MCN Lect Multiple Pregnancy Hydramnios PosttermDocument5 pagesMCN Lect Multiple Pregnancy Hydramnios PosttermAmethystNo ratings yet
- Abortion KuliahDocument38 pagesAbortion KuliahElsa Hasibuan100% (1)
- Problems With The PassengerDocument58 pagesProblems With The PassengerJim NavarroNo ratings yet
- Embryology, Pathophysiology, and Ultrasound Characteristics of The Placenta ObjectivesDocument13 pagesEmbryology, Pathophysiology, and Ultrasound Characteristics of The Placenta ObjectivesAudrey100% (5)
- MC Pregnancy Version 12 17 5 10Document13 pagesMC Pregnancy Version 12 17 5 10Ram ParepalliNo ratings yet
- On Autumn's Wing, A Story of Birth Trauma, Brain Injury and Miracles.From EverandOn Autumn's Wing, A Story of Birth Trauma, Brain Injury and Miracles.No ratings yet
- Đáp Án ReadingDocument2 pagesĐáp Án ReadingLanAnhNo ratings yet
- What Is A Good Thesis Statement For The Black DeathDocument8 pagesWhat Is A Good Thesis Statement For The Black Deathdwsmjsqy100% (1)
- Tribal Development Through Five Year Plans in India - An Overview PDFDocument23 pagesTribal Development Through Five Year Plans in India - An Overview PDFdevath sureshNo ratings yet
- Research Final Draft (Part2)Document28 pagesResearch Final Draft (Part2)Mae Colmenares100% (10)
- Safety Data Sheet Winsor & Newton Artist Acrylic Gloss Uv Varnish (Us MSDS)Document3 pagesSafety Data Sheet Winsor & Newton Artist Acrylic Gloss Uv Varnish (Us MSDS)zaryab khanNo ratings yet
- ITC - Indian Tobacco Company: FMCG IndustryDocument35 pagesITC - Indian Tobacco Company: FMCG IndustryAbhinav SinghNo ratings yet
- Original Article: Laparoscopic Inguinal Lymphadenectomy: A New Minimally Invasive Technique To Treat Vulva CarcinomaDocument6 pagesOriginal Article: Laparoscopic Inguinal Lymphadenectomy: A New Minimally Invasive Technique To Treat Vulva CarcinomaVlad GrigoreNo ratings yet
- California Long-Term Care Programs: Recommendations To Improve Access For CaliforniansDocument329 pagesCalifornia Long-Term Care Programs: Recommendations To Improve Access For CaliforniansLeslie HendricksonNo ratings yet
- What Is PPE (Personal Protective Equipment) - The PM HQ PDFDocument18 pagesWhat Is PPE (Personal Protective Equipment) - The PM HQ PDFshreyas100% (1)
- Documentation of Nursing CareDocument58 pagesDocumentation of Nursing CareValence Mfitumukiza88% (8)
- DDA Strategic PlanDocument92 pagesDDA Strategic PlanJudith AinembabaziNo ratings yet
- A Comparative Study of Prison Systems in African Countries (O.A.Stephens, 2018)Document374 pagesA Comparative Study of Prison Systems in African Countries (O.A.Stephens, 2018)Razi MahriNo ratings yet
- AIQ English Version 2021Document159 pagesAIQ English Version 2021FxhTDhNo ratings yet
- Bowel Incontinence ConstipationDocument3 pagesBowel Incontinence ConstipationMatty-b AskalaniNo ratings yet
- Ls4 Elem Las21 To-Las50-MergedDocument31 pagesLs4 Elem Las21 To-Las50-MergedJaypee Aturo100% (2)
- Forensic Toxicology HDocument18 pagesForensic Toxicology Hq_onda_fhonixNo ratings yet
- Beware of Sexually Transmitted DemonsDocument12 pagesBeware of Sexually Transmitted DemonsOyunbileg Baatar100% (4)
- Travel Insurance: Travel Insurance Benefits: Healthcare Is Expensive in Most Parts of The World, EspeciallyDocument3 pagesTravel Insurance: Travel Insurance Benefits: Healthcare Is Expensive in Most Parts of The World, Especiallycover360.inNo ratings yet
- Rapidpoint 400Document4 pagesRapidpoint 400Oo Kenx OoNo ratings yet
- Republic Act No 5527Document7 pagesRepublic Act No 5527jennahmontoya5No ratings yet
- Urinalysis Interpretation and Clinical CorrelationsDocument21 pagesUrinalysis Interpretation and Clinical CorrelationsFercho MedNo ratings yet
- THORACOTOMYDocument3 pagesTHORACOTOMYConnie May Fernando Evangelio100% (1)
- Municipal Ordinance No. 284 S. 2010Document8 pagesMunicipal Ordinance No. 284 S. 2010Michelle J UrbodaNo ratings yet
- Chemical Pathology 5 - HypoglycaemiaDocument10 pagesChemical Pathology 5 - HypoglycaemiaaNo ratings yet

























































































Download as pptx, pdf, or txt
You might also like
- Pharmacology For Nurses Third Canadian Edition 3Rd Edition Full ChapterDocument41 pagesPharmacology For Nurses Third Canadian Edition 3Rd Edition Full Chaptermuriel.moreno949100% (26)
- Case Studies Accommodations2Document4 pagesCase Studies Accommodations2api-325828984No ratings yet
- Understanding ViolenceDocument232 pagesUnderstanding ViolenceBenchea Silvestru100% (6)
- Multiple Pregnancy - PPTX Md3Document41 pagesMultiple Pregnancy - PPTX Md3Brother George100% (1)
- Multiple Pregnancy LectureDocument33 pagesMultiple Pregnancy Lecturefarid_nchep100% (1)
- Roles and Responsibilities of Local DRRM OfficersDocument22 pagesRoles and Responsibilities of Local DRRM OfficersErnan Baldomero92% (12)
- (BS 1133-6.1-1991) - Packaging Code. Protection of Metal Surfaces Against Corrosion During Transport and Storage. Cleaning and Drying of Metal SurfacesDocument34 pages(BS 1133-6.1-1991) - Packaging Code. Protection of Metal Surfaces Against Corrosion During Transport and Storage. Cleaning and Drying of Metal SurfacesTowkir AhmmadNo ratings yet
- Global Natural Source Vitamin E Market - 2018 To 2024 (Tocopherols and Tocotrienols)Document5 pagesGlobal Natural Source Vitamin E Market - 2018 To 2024 (Tocopherols and Tocotrienols)Industry Experts, Inc.No ratings yet
- Multiple Pregnancy 1Document56 pagesMultiple Pregnancy 1angel panchalNo ratings yet
- 4th Year Multiple PregnancyDocument57 pages4th Year Multiple PregnancyKingsley Calex100% (2)
- Multiple Pregnancy1Document57 pagesMultiple Pregnancy1Muhammad Abeesh100% (1)
- Multiple GestationDocument24 pagesMultiple GestationNura BamaiyiNo ratings yet
- MK Multiple Gestation (OBGY)Document16 pagesMK Multiple Gestation (OBGY)Moses Jr KazevuNo ratings yet
- Multiple Pregnancy: Fahad ZakwanDocument60 pagesMultiple Pregnancy: Fahad Zakwanhaisuresh100% (1)
- Multiple Pregnancy: Prof Uma SinghDocument53 pagesMultiple Pregnancy: Prof Uma Singhgeng gengNo ratings yet
- Multiple Gestation: Dr. Hotma Partogi Pasaribu Spog Sub Division of Fetomaternal Medical Faculty - Usu Rsham - RSPM MedanDocument47 pagesMultiple Gestation: Dr. Hotma Partogi Pasaribu Spog Sub Division of Fetomaternal Medical Faculty - Usu Rsham - RSPM MedanSyarifah KhamsiawanNo ratings yet
- Multifetal Pregnancy: Dr. Hani MahdiDocument59 pagesMultifetal Pregnancy: Dr. Hani MahdiArwa QishtaNo ratings yet
- Multifetal Pregnancy: Amr Nadim, MDDocument36 pagesMultifetal Pregnancy: Amr Nadim, MDsharenNo ratings yet
- Multiple Pregnancy: Prof Uma SinghDocument53 pagesMultiple Pregnancy: Prof Uma Singhpok yeahNo ratings yet
- Multiple Pregnancy: Kevin AndrewDocument36 pagesMultiple Pregnancy: Kevin AndrewintanpurnNo ratings yet
- Twin TDocument30 pagesTwin TmaezuNo ratings yet
- Multiple Pregnancy HatimDocument22 pagesMultiple Pregnancy HatimHatim AbdellateifNo ratings yet
- 2 Multiple - Pregnancy - Lecture 2018Document48 pages2 Multiple - Pregnancy - Lecture 2018abrhamNo ratings yet
- Multiple Births - Embryology of TwinningDocument24 pagesMultiple Births - Embryology of TwinningtawandarukwavamadisonNo ratings yet
- Multiple PregnanciesDocument36 pagesMultiple PregnanciesBasudev ch100% (1)
- Multiple PXDocument46 pagesMultiple PXBetelhem EjiguNo ratings yet
- A Multiple Birth Occurs When More ThanDocument16 pagesA Multiple Birth Occurs When More ThanVaibhav BhatiaNo ratings yet
- Breech PresentationDocument16 pagesBreech Presentationkhadija falakNo ratings yet
- Malpresntation, Malposition and Breech Presentation 2022 BayisaDocument45 pagesMalpresntation, Malposition and Breech Presentation 2022 BayisaHile ShaNo ratings yet
- Multiple PregnancyDocument52 pagesMultiple Pregnancyazida90100% (4)
- Multiple Fetal Pregnancy: Riza SufriadiDocument20 pagesMultiple Fetal Pregnancy: Riza SufriadiRizur SufisonNo ratings yet
- Multiple PregnancyDocument83 pagesMultiple PregnancyAmna MaqboolNo ratings yet
- Multiple PregnancyDocument32 pagesMultiple PregnancyRebbeccah NafulaNo ratings yet
- Multiple PregnancyDocument28 pagesMultiple PregnancyFarxan Da Napolian BwoyNo ratings yet
- Multiplepregnancy 100515015745 Phpapp01Document29 pagesMultiplepregnancy 100515015745 Phpapp01haisureshNo ratings yet
- Multifetal PregnancyDocument68 pagesMultifetal PregnancyHoque Mohammed Newaz ShorifulNo ratings yet
- SEMINAR ON MULTIPLE PREGNANCY ContentDocument21 pagesSEMINAR ON MULTIPLE PREGNANCY ContentMonika shankar0% (1)
- Functional Anatomy - Part II: Uterus, Fetal Circulation & Male Reproductive Organ Selected VariationsDocument69 pagesFunctional Anatomy - Part II: Uterus, Fetal Circulation & Male Reproductive Organ Selected Variationshfkxbbbty2No ratings yet
- Multiple Pregnancy 2008Document61 pagesMultiple Pregnancy 2008Dagnachew kasayeNo ratings yet
- Prenatal DevelopmentDocument30 pagesPrenatal DevelopmentAnu ChauhanNo ratings yet
- Twin Pregnancy: Dr. Girishankar Samarasam Supervised By: DR Rathimalar DR Mohd Faizal Bin Nor AzmiDocument56 pagesTwin Pregnancy: Dr. Girishankar Samarasam Supervised By: DR Rathimalar DR Mohd Faizal Bin Nor AzmiShre RanjithamNo ratings yet
- Twins: SupervisorDocument10 pagesTwins: Supervisorكيرلس مجدىNo ratings yet
- Understanding Multiple Pregnancy: Maternal & Fetal ComplicationsDocument69 pagesUnderstanding Multiple Pregnancy: Maternal & Fetal Complications966342No ratings yet
- Multiple Pregnancy: Dr. A. Farid Abdullah, SP - OG, M.KesDocument33 pagesMultiple Pregnancy: Dr. A. Farid Abdullah, SP - OG, M.KesAndi Farid A100% (1)
- Antepartum Hemorrhage: Placental CausesDocument9 pagesAntepartum Hemorrhage: Placental CausesadiNo ratings yet
- Multiple PregnancyDocument71 pagesMultiple PregnancyAndre PutraNo ratings yet
- Abnormal Lie: - Abnormal Lie Consists of Two Types: Transverse Lie Oblique LieDocument21 pagesAbnormal Lie: - Abnormal Lie Consists of Two Types: Transverse Lie Oblique LieBharat ThapaNo ratings yet
- علاااءDocument21 pagesعلاااءalaazeez2000No ratings yet
- Kehamilan Ganda1Document54 pagesKehamilan Ganda1rizmaNo ratings yet
- Book ReportDocument69 pagesBook ReportBarangay MotibotNo ratings yet
- Multiple PregnancyDocument23 pagesMultiple Pregnancy19 KomalNo ratings yet
- Multiple PregnancyDocument20 pagesMultiple PregnancyNurul Fahmiza TumiranNo ratings yet
- Multifetal PintDocument51 pagesMultifetal PintLeikkaNo ratings yet
- Muhammad Redzwan Bin Abdullah: 081303583 Batch 25 Group E2Document66 pagesMuhammad Redzwan Bin Abdullah: 081303583 Batch 25 Group E2Suyajna JoshiNo ratings yet
- Abnormal Labor Lec 1Document34 pagesAbnormal Labor Lec 1Zahraa HasanNo ratings yet
- Multiple Pregnancy: Nirav Hitesh Kumar ValandDocument28 pagesMultiple Pregnancy: Nirav Hitesh Kumar ValandNirav SharmaNo ratings yet
- 08 Twins Birth DiagnosticDocument6 pages08 Twins Birth DiagnosticElliotPianoNo ratings yet
- Placental PathologyDocument465 pagesPlacental PathologyOana Roxana PuscasNo ratings yet
- Multiple PregnancesssssDocument29 pagesMultiple PregnancesssssNajjemba ShanitahNo ratings yet
- MCN Lect Multiple Pregnancy Hydramnios PosttermDocument5 pagesMCN Lect Multiple Pregnancy Hydramnios PosttermAmethystNo ratings yet
- Abortion KuliahDocument38 pagesAbortion KuliahElsa Hasibuan100% (1)
- Problems With The PassengerDocument58 pagesProblems With The PassengerJim NavarroNo ratings yet
- Embryology, Pathophysiology, and Ultrasound Characteristics of The Placenta ObjectivesDocument13 pagesEmbryology, Pathophysiology, and Ultrasound Characteristics of The Placenta ObjectivesAudrey100% (5)
- MC Pregnancy Version 12 17 5 10Document13 pagesMC Pregnancy Version 12 17 5 10Ram ParepalliNo ratings yet
- On Autumn's Wing, A Story of Birth Trauma, Brain Injury and Miracles.From EverandOn Autumn's Wing, A Story of Birth Trauma, Brain Injury and Miracles.No ratings yet
- Đáp Án ReadingDocument2 pagesĐáp Án ReadingLanAnhNo ratings yet
- What Is A Good Thesis Statement For The Black DeathDocument8 pagesWhat Is A Good Thesis Statement For The Black Deathdwsmjsqy100% (1)
- Tribal Development Through Five Year Plans in India - An Overview PDFDocument23 pagesTribal Development Through Five Year Plans in India - An Overview PDFdevath sureshNo ratings yet
- Research Final Draft (Part2)Document28 pagesResearch Final Draft (Part2)Mae Colmenares100% (10)
- Safety Data Sheet Winsor & Newton Artist Acrylic Gloss Uv Varnish (Us MSDS)Document3 pagesSafety Data Sheet Winsor & Newton Artist Acrylic Gloss Uv Varnish (Us MSDS)zaryab khanNo ratings yet
- ITC - Indian Tobacco Company: FMCG IndustryDocument35 pagesITC - Indian Tobacco Company: FMCG IndustryAbhinav SinghNo ratings yet
- Original Article: Laparoscopic Inguinal Lymphadenectomy: A New Minimally Invasive Technique To Treat Vulva CarcinomaDocument6 pagesOriginal Article: Laparoscopic Inguinal Lymphadenectomy: A New Minimally Invasive Technique To Treat Vulva CarcinomaVlad GrigoreNo ratings yet
- California Long-Term Care Programs: Recommendations To Improve Access For CaliforniansDocument329 pagesCalifornia Long-Term Care Programs: Recommendations To Improve Access For CaliforniansLeslie HendricksonNo ratings yet
- What Is PPE (Personal Protective Equipment) - The PM HQ PDFDocument18 pagesWhat Is PPE (Personal Protective Equipment) - The PM HQ PDFshreyas100% (1)
- Documentation of Nursing CareDocument58 pagesDocumentation of Nursing CareValence Mfitumukiza88% (8)
- DDA Strategic PlanDocument92 pagesDDA Strategic PlanJudith AinembabaziNo ratings yet
- A Comparative Study of Prison Systems in African Countries (O.A.Stephens, 2018)Document374 pagesA Comparative Study of Prison Systems in African Countries (O.A.Stephens, 2018)Razi MahriNo ratings yet
- AIQ English Version 2021Document159 pagesAIQ English Version 2021FxhTDhNo ratings yet
- Bowel Incontinence ConstipationDocument3 pagesBowel Incontinence ConstipationMatty-b AskalaniNo ratings yet
- Ls4 Elem Las21 To-Las50-MergedDocument31 pagesLs4 Elem Las21 To-Las50-MergedJaypee Aturo100% (2)
- Forensic Toxicology HDocument18 pagesForensic Toxicology Hq_onda_fhonixNo ratings yet
- Beware of Sexually Transmitted DemonsDocument12 pagesBeware of Sexually Transmitted DemonsOyunbileg Baatar100% (4)
- Travel Insurance: Travel Insurance Benefits: Healthcare Is Expensive in Most Parts of The World, EspeciallyDocument3 pagesTravel Insurance: Travel Insurance Benefits: Healthcare Is Expensive in Most Parts of The World, Especiallycover360.inNo ratings yet
- Rapidpoint 400Document4 pagesRapidpoint 400Oo Kenx OoNo ratings yet
- Republic Act No 5527Document7 pagesRepublic Act No 5527jennahmontoya5No ratings yet
- Urinalysis Interpretation and Clinical CorrelationsDocument21 pagesUrinalysis Interpretation and Clinical CorrelationsFercho MedNo ratings yet
- THORACOTOMYDocument3 pagesTHORACOTOMYConnie May Fernando Evangelio100% (1)
- Municipal Ordinance No. 284 S. 2010Document8 pagesMunicipal Ordinance No. 284 S. 2010Michelle J UrbodaNo ratings yet
- Chemical Pathology 5 - HypoglycaemiaDocument10 pagesChemical Pathology 5 - HypoglycaemiaaNo ratings yet