Download as pptx, pdf, or txt
You might also like
- NCP Formulation (Older Adult)Document3 pagesNCP Formulation (Older Adult)maria khalifa0% (1)
- Bobath Approach: Neuro-Developmental TechniquesDocument25 pagesBobath Approach: Neuro-Developmental TechniquesJAZA RIZVI100% (1)
- The Legal Epistemology of Qur'anic Variants: The Readings of Ibn Mas'ud in Kufan Fiqh and The Hanafi Madhhab - Postprint - Ramon HarveyDocument30 pagesThe Legal Epistemology of Qur'anic Variants: The Readings of Ibn Mas'ud in Kufan Fiqh and The Hanafi Madhhab - Postprint - Ramon Harveyrnharvey100% (1)
- IRAC Formulas PDFDocument7 pagesIRAC Formulas PDFroy rebosuraNo ratings yet
- Rehabilitation 10Document41 pagesRehabilitation 10njanevidepettuNo ratings yet
- Pediatric Rehabilitation FiDocument61 pagesPediatric Rehabilitation FidannisanurmiyaNo ratings yet
- Neuro-Developmental TherapyDocument28 pagesNeuro-Developmental Therapythandiwebandile2No ratings yet
- DR Luh - Role of PMR in NICUDocument50 pagesDR Luh - Role of PMR in NICUad putraNo ratings yet
- Dr.P.Udhaya Kumar MD - PM&R 1st Year PG Department of PM&R Moderator Dr.S.Chidambaranathan Department of PaediatricsDocument45 pagesDr.P.Udhaya Kumar MD - PM&R 1st Year PG Department of PM&R Moderator Dr.S.Chidambaranathan Department of PaediatricsUdhaya KumarNo ratings yet
- Motor Control Motor LearningDocument56 pagesMotor Control Motor LearningJune EpeNo ratings yet
- Neuro-Developmental Therapy/Treatment: Pediatric Physical Therapy, NDTDocument13 pagesNeuro-Developmental Therapy/Treatment: Pediatric Physical Therapy, NDTMuhamed Elsayed - Zalat100% (1)
- Cerebral Palsy (CP) (Chap21)Document30 pagesCerebral Palsy (CP) (Chap21)kashmala afzalNo ratings yet
- Treatment Approaches For A CP ChildDocument17 pagesTreatment Approaches For A CP Childpraveen0% (1)
- 2 - Bobath CoceptDocument41 pages2 - Bobath CoceptSaba Iqbal100% (2)
- Sensory Toolkit Final LS 002Document5 pagesSensory Toolkit Final LS 002Raghaveni RVNo ratings yet
- LTAD Appendix 1Document8 pagesLTAD Appendix 1Anonymous GJuRvp9A5TNo ratings yet
- Llorens Facilitation and Growth DevelopmentDocument20 pagesLlorens Facilitation and Growth DevelopmentAarthi ArumugamNo ratings yet
- DSTPaper 1Document8 pagesDSTPaper 1Suprava PatnaikNo ratings yet
- Integrating NDT and SI-Theory and PracticeDocument7 pagesIntegrating NDT and SI-Theory and PracticePaulinaNo ratings yet
- NDT in Children - Gina Rencken 2022 - PANDADocument20 pagesNDT in Children - Gina Rencken 2022 - PANDAGokul SriniNo ratings yet
- Sensory Processing Presentation February 2014Document58 pagesSensory Processing Presentation February 2014Geovanny NuñezNo ratings yet
- 6 Komponen SensoriDocument29 pages6 Komponen SensoriYusrina RahmaNo ratings yet
- Sensory Motor Approaches: Asma KhalidDocument31 pagesSensory Motor Approaches: Asma KhalidAsaad Jawed100% (1)
- Effectiveness of Sensory Integration Therapy (Vestibular & Proprioception Input) On Gross Motor Functioning in Developmental Delayed and Spastic Diplegic CP ChildrenDocument6 pagesEffectiveness of Sensory Integration Therapy (Vestibular & Proprioception Input) On Gross Motor Functioning in Developmental Delayed and Spastic Diplegic CP ChildrenYanuar Adi SanjayaNo ratings yet
- Aho - SI - Basic Guide 2022 What Is SIDocument2 pagesAho - SI - Basic Guide 2022 What Is SISaskiayusNo ratings yet
- Cerebral Palsy Note (SP Edit)Document1 pageCerebral Palsy Note (SP Edit)medical chroniclesNo ratings yet
- PT Relevance RMTDocument10 pagesPT Relevance RMTsnehanadkarni64No ratings yet
- Bobath Approach 1Document61 pagesBobath Approach 1Senthil Kumar100% (1)
- BobathDocument9 pagesBobathStratiatella Faith AnthonyNo ratings yet
- OT Relevance RMTDocument12 pagesOT Relevance RMTFredy RamoneNo ratings yet
- The Treatment Plan For Pediatric Cases in Healing Hands: DR: Moath DR: AqsaDocument28 pagesThe Treatment Plan For Pediatric Cases in Healing Hands: DR: Moath DR: AqsaArt and Fashion galleryNo ratings yet
- Bobath Approach NotesDocument5 pagesBobath Approach NotesJuling Perales100% (3)
- Neuro Developmental Treatment (NDT) : Prepared By: Akhi Mony Clinical Physiotherapist (CPT) CRP-MirpurDocument24 pagesNeuro Developmental Treatment (NDT) : Prepared By: Akhi Mony Clinical Physiotherapist (CPT) CRP-MirpurAkhi MonyNo ratings yet
- BobathDocument150 pagesBobathramesh natrayan100% (1)
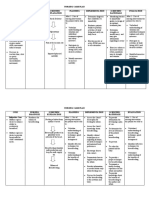
- Nursing Care Plan Cues Nursing Diagnosis Scientific Explanation Planning Implementation Scientific Rationale Evaluation Subjective CuesDocument4 pagesNursing Care Plan Cues Nursing Diagnosis Scientific Explanation Planning Implementation Scientific Rationale Evaluation Subjective Cues24 PAULINO ALDRIN MUJARNo ratings yet
- 51 55Document5 pages51 55SuniNo ratings yet
- Cerebral Palsy IDocument2 pagesCerebral Palsy Iapi-3822433No ratings yet
- Vojta at Cerebra - Org.uk PDFDocument12 pagesVojta at Cerebra - Org.uk PDFGavriela CostachiNo ratings yet
- Birchtree Sensory Presentation WebDocument17 pagesBirchtree Sensory Presentation WebMai MahmoudNo ratings yet
- Vestibular Handout FinalDocument2 pagesVestibular Handout Finalapi-414170492No ratings yet
- Sensory Diet DocumentsDocument7 pagesSensory Diet Documentspratibhaumrariya100% (1)
- Origins of Theoretical ApproachDocument15 pagesOrigins of Theoretical ApproachnrusinghNo ratings yet
- BobathDocument28 pagesBobathSaba SamimNo ratings yet
- Bobath LectureDocument25 pagesBobath Lectureみ にゅきゅ100% (3)
- Dr. Luh PPT CP 2019Document31 pagesDr. Luh PPT CP 2019Ahimsa Yoga Anindita100% (1)
- Neuro Developmental Treatment (NDT) Techniques: HistoryDocument3 pagesNeuro Developmental Treatment (NDT) Techniques: HistoryGafencu SergiuNo ratings yet
- Theories of Neurological RehabilitationDocument30 pagesTheories of Neurological Rehabilitationabdul haseebNo ratings yet
- Rehabilitation Approach of Children With Cerebral PalsyDocument55 pagesRehabilitation Approach of Children With Cerebral PalsyridaNo ratings yet
- CP PDFDocument7 pagesCP PDFannaNo ratings yet
- Assignment:: Neurological Physical TherapyDocument5 pagesAssignment:: Neurological Physical TherapyAqsa FahimNo ratings yet
- Case IcuDocument5 pagesCase IcuTrisha SuazoNo ratings yet
- Ayres Sensory Integration PrinciplesDocument25 pagesAyres Sensory Integration Principlesapi-413184352100% (3)
- Cahpater 10 ManagementofcerebralpalsyDocument71 pagesCahpater 10 Managementofcerebralpalsyashlyn granthamNo ratings yet
- Moderate Autism (NCP-Drug)Document4 pagesModerate Autism (NCP-Drug)Laila V. MananonNo ratings yet
- Neurodesarrollo: TO Maximiliano Merino S. Clase Basada en Documentos de TO Marcos Chiang y TO Cristina FernándezDocument22 pagesNeurodesarrollo: TO Maximiliano Merino S. Clase Basada en Documentos de TO Marcos Chiang y TO Cristina FernándezValeNeiraNo ratings yet
- Kids' Core: Core Strengthening Program For ChildrenDocument9 pagesKids' Core: Core Strengthening Program For ChildrenMertcan DamatNo ratings yet
- Application of Facilitatory Approaches in Developmental DysarthriaDocument22 pagesApplication of Facilitatory Approaches in Developmental Dysarthriakeihoina keihoinaNo ratings yet
- Neurodevelopmental Treatment (NDT) in Paediatrics: Victoria Prooday Manuela Ocrainschi Alda MeloDocument36 pagesNeurodevelopmental Treatment (NDT) in Paediatrics: Victoria Prooday Manuela Ocrainschi Alda MeloDnyanesh Patil100% (1)
- Environmental EnrichmentDocument11 pagesEnvironmental Enrichmentlic.lucilaalzNo ratings yet
- Brain Breakthrough: The Art of Neurological Rehabilitation: Easy and Innovative Techniques, #1From EverandBrain Breakthrough: The Art of Neurological Rehabilitation: Easy and Innovative Techniques, #1No ratings yet
- BeBalanced!: The innovative training program with Balance-pads & co.From EverandBeBalanced!: The innovative training program with Balance-pads & co.No ratings yet
- Io-Link Hub For 8 Analog Input SignalsDocument2 pagesIo-Link Hub For 8 Analog Input SignalsGabriel CardosoNo ratings yet
- Blockchain Spec PDFDocument18 pagesBlockchain Spec PDFblueNo ratings yet
- 02 Algorithm AnalysisDocument49 pages02 Algorithm AnalysisĐăng BùiNo ratings yet
- Definition of Research, Characteristics of Research, Research Process and Functions of Research Definition of ResearchDocument2 pagesDefinition of Research, Characteristics of Research, Research Process and Functions of Research Definition of ResearchNinda SNo ratings yet
- BSBTWK502 Project PortfolioDocument11 pagesBSBTWK502 Project Portfoliobarun ghimireNo ratings yet
- Ananya ROY: Software EngineerDocument1 pageAnanya ROY: Software EngineerAshishNo ratings yet
- Quick Manual To Operate Ballast Water of S615Document2 pagesQuick Manual To Operate Ballast Water of S615NikulNo ratings yet
- MGMT100S2 2019 - With Lecture Schedule PDFDocument8 pagesMGMT100S2 2019 - With Lecture Schedule PDFAkshayScamlattiNo ratings yet
- Simplifications PDF Set 5 PDFDocument22 pagesSimplifications PDF Set 5 PDFHriday MittraNo ratings yet
- Radio Link FailureDocument19 pagesRadio Link FailureDeepanshu SharmaNo ratings yet
- Solvent Extraction of Aluminium in The Presence of Cobalt, Nickel and Magnesium From Sulphate Solutions by Cyanex 272Document8 pagesSolvent Extraction of Aluminium in The Presence of Cobalt, Nickel and Magnesium From Sulphate Solutions by Cyanex 272Leda HidalgoNo ratings yet
- Biodontics: A ReviewDocument4 pagesBiodontics: A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jerome K JeromeDocument117 pagesJerome K JeromeVictoria BelundiNo ratings yet
- Laplace TransformsDocument22 pagesLaplace TransformsAustin JamesNo ratings yet
- ReadmeDocument6 pagesReadmegabyorNo ratings yet
- Elln Matrix: Valenzuela South District Ilang-Ilang St. Karuhatan, Valenzuela City Tel/fax No. 2944246Document1 pageElln Matrix: Valenzuela South District Ilang-Ilang St. Karuhatan, Valenzuela City Tel/fax No. 2944246rafaela villanuevaNo ratings yet
- Multi Inverter 4TXM6530A-SUB-1GDocument4 pagesMulti Inverter 4TXM6530A-SUB-1GOmar PiñaNo ratings yet
- Grade: 10E ROOM: 212 Homeroom Adviser: John Paolo FernandezDocument1 pageGrade: 10E ROOM: 212 Homeroom Adviser: John Paolo FernandezRangga NarindraNo ratings yet
- 1 - Introduction To Accountign - Icap - Questions and Answers PDFDocument202 pages1 - Introduction To Accountign - Icap - Questions and Answers PDFM.Abdullah MBIT100% (1)
- BRAPDocument5 pagesBRAPrkkask01No ratings yet
- Requirements For Al Ayuni Saudi Arabia: Sponsor Interview On 2Nd Week of June 2019Document3 pagesRequirements For Al Ayuni Saudi Arabia: Sponsor Interview On 2Nd Week of June 2019Tradiyo ForexNo ratings yet
- Savemyexams Igcse Biology Photosynthesis and Leaf Structure WorksheetDocument34 pagesSavemyexams Igcse Biology Photosynthesis and Leaf Structure WorksheetkatisspeedNo ratings yet
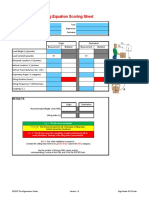
- NIOSH Lifting Equation Scoring Sheet: ResultsDocument5 pagesNIOSH Lifting Equation Scoring Sheet: ResultsLucio VieiraNo ratings yet
- Assam - WikipediaDocument32 pagesAssam - WikipediaNazrul IslamNo ratings yet
- CGC1D Assignment 2.1 Fire and Ice ArticlesDocument3 pagesCGC1D Assignment 2.1 Fire and Ice ArticlesMayaNo ratings yet
- When Textbook RSA Is Used To Protect The Privacy of Hundreds of Millions of UsersDocument9 pagesWhen Textbook RSA Is Used To Protect The Privacy of Hundreds of Millions of UsersShaanan CohneyNo ratings yet
- Single Award End of Feb 2023Document8 pagesSingle Award End of Feb 2023Lone G. MokgalagadiNo ratings yet
- Management Strategies For Primary Dysmenorrhea: 9.1 Topic OverviewDocument19 pagesManagement Strategies For Primary Dysmenorrhea: 9.1 Topic OverviewAgusdiwana SuarniNo ratings yet