Download as pptx, pdf, or txt
You might also like
- Jesus The Liberator - Jon SorbinoDocument321 pagesJesus The Liberator - Jon SorbinoavaMotivatorije94% (16)
- Mercruiser Service Manual #14 Alpha I Gen II Outdrives 1991-NewerDocument715 pagesMercruiser Service Manual #14 Alpha I Gen II Outdrives 1991-NewerM5Melo100% (10)
- Ophthalmic Dispensing Revision Guide: First Year Part OneFrom EverandOphthalmic Dispensing Revision Guide: First Year Part OneRating: 4 out of 5 stars4/5 (3)
- SS Number State CodesDocument5 pagesSS Number State CodesCharles Kimbrough Sr.0% (1)
- Tropical SoilsDocument88 pagesTropical SoilsBernard Kipng'eno100% (1)
- 057 PDFDocument15 pages057 PDFVương BanNo ratings yet
- Laser and Its ApplicationsDocument50 pagesLaser and Its ApplicationsmadangkNo ratings yet
- Spanish 155 WorksheetDocument3 pagesSpanish 155 WorksheetJaiza Kathrina BaylosisNo ratings yet
- Laser in OperativeDocument99 pagesLaser in OperativeAnisha AnilNo ratings yet
- LaserDocument15 pagesLaserVibek GuptaNo ratings yet
- LasersDocument22 pagesLasersAtul KhattarNo ratings yet
- Laser BasicsDocument8 pagesLaser BasicsVishali RayapudiNo ratings yet
- Akhil Laser.maxDocument20 pagesAkhil Laser.maxAkhil KashYapNo ratings yet
- LaserDocument22 pagesLaserRaghuveer ReddyNo ratings yet
- Modern Physics and Electronics: TopicDocument31 pagesModern Physics and Electronics: TopicAmandeep Singh KheraNo ratings yet
- Laser Wps OfficeDocument11 pagesLaser Wps Officeshibi chakkravathi K.TNo ratings yet
- Lasers in DentistryDocument53 pagesLasers in DentistryDr. Nikhil saranNo ratings yet
- Laser CharacteristicsDocument5 pagesLaser Characteristics20S027 - SANJAY SNEHAN SNo ratings yet
- Laser Scanner TechnologyDocument22 pagesLaser Scanner TechnologyEng M G ElkhateebNo ratings yet
- Light: Modern PhysicsDocument5 pagesLight: Modern PhysicsJef PerezNo ratings yet
- Light: Electromagnetic Radiation Light (Disambiguation) Visible Light (Disambiguation)Document19 pagesLight: Electromagnetic Radiation Light (Disambiguation) Visible Light (Disambiguation)AnandNo ratings yet
- Electromagnetic Spectrum and Visible LightDocument14 pagesElectromagnetic Spectrum and Visible LightDreian Calaoagan PalalayNo ratings yet
- LaserDocument20 pagesLasertsrockon28No ratings yet
- Phy 104 Atomic SpectraDocument24 pagesPhy 104 Atomic SpectraAisha abba HabibNo ratings yet
- Term Paper Laser, Action, Einstein Theory of Laser, Types, Applications in Industry & Medical FieldDocument15 pagesTerm Paper Laser, Action, Einstein Theory of Laser, Types, Applications in Industry & Medical FieldGarima SoniNo ratings yet
- LASERDocument3 pagesLASERBhaskar Rao PNo ratings yet
- Fundamentals: by Stimulated Emission of RadiationDocument8 pagesFundamentals: by Stimulated Emission of RadiationSharanjeet KaurNo ratings yet
- Lecture 3 (1) - 240324 - 205149Document11 pagesLecture 3 (1) - 240324 - 205149btwlalbwdy16No ratings yet
- Despre Lumina in Limba EnglezaDocument7 pagesDespre Lumina in Limba EnglezaDia0505No ratings yet
- Objective:: To Determine The Wavelength of Yellow Light Emitting From The Na-Lamp.Document14 pagesObjective:: To Determine The Wavelength of Yellow Light Emitting From The Na-Lamp.suleman205No ratings yet
- SpectroscopyetextDocument23 pagesSpectroscopyetextTejaswiniNo ratings yet
- 3 WDDocument5 pages3 WDMuhammed MinhajNo ratings yet
- Sonic LaserDocument17 pagesSonic LaserPawan chandra UpretiNo ratings yet
- Engineering Physics PHY-109 Laser-1: Quantum MechanicsDocument24 pagesEngineering Physics PHY-109 Laser-1: Quantum MechanicsKaburagi KazeoNo ratings yet
- Laser 1 PDFDocument17 pagesLaser 1 PDFJyotirmay VishweshNo ratings yet
- LASERDocument36 pagesLASERAnna100% (2)
- Chemistry Project On SpectrosDocument9 pagesChemistry Project On SpectrosAtul Sharma33% (3)
- Laser, Action, Einstein Theory of Laser, Types, Applications in IndustryDocument27 pagesLaser, Action, Einstein Theory of Laser, Types, Applications in IndustryChad Smith100% (5)
- Light: 1 Electromagnetic Spectrum and Visible LightDocument11 pagesLight: 1 Electromagnetic Spectrum and Visible LightAyushJaiswalNo ratings yet
- Definition of Light WavesDocument9 pagesDefinition of Light WavesJF BatucalNo ratings yet
- History: Spectrum IsDocument23 pagesHistory: Spectrum IsMuhamad NurhudayahNo ratings yet
- FOL Unit 3Document17 pagesFOL Unit 3Sudhar SanNo ratings yet
- Principii de Baza Despre LaserDocument3 pagesPrincipii de Baza Despre LaserStefan GabureanuNo ratings yet
- CBSE XII Chemistry Project Spectroscopy and Its ApplicationsDocument21 pagesCBSE XII Chemistry Project Spectroscopy and Its ApplicationsRichie SinghNo ratings yet
- Optics 1Document5 pagesOptics 1asopNo ratings yet
- Lasers Understanding The Basics Lasers Photonics Handbook Photonics MarketplaceDocument26 pagesLasers Understanding The Basics Lasers Photonics Handbook Photonics MarketplaceCarl MacCordNo ratings yet
- What Is SpectrosDocument4 pagesWhat Is SpectrosCarlton GrantNo ratings yet
- Group 8 Presentation Humss 7 Lesson 8Document32 pagesGroup 8 Presentation Humss 7 Lesson 8Princess Dianne GarciaNo ratings yet
- Spectroscopy and Its ApplicationsDocument21 pagesSpectroscopy and Its Applicationspkkalai112No ratings yet
- Description: Electromagnetic Radiation Charged ParticlesDocument8 pagesDescription: Electromagnetic Radiation Charged ParticlesfaithNo ratings yet
- Laser - WikipediaDocument148 pagesLaser - WikipediaAnkur SinghNo ratings yet
- Physics1101 - Course MaterialDocument332 pagesPhysics1101 - Course MaterialAhmad RazaNo ratings yet
- 1587138047MLS 314 Lecture Note (2019-2020)Document29 pages1587138047MLS 314 Lecture Note (2019-2020)rameezchaudhary964No ratings yet
- SpectrosDocument35 pagesSpectrosLoren Victoria AgbayNo ratings yet
- Light: Jump To Navigationjump To SearchDocument22 pagesLight: Jump To Navigationjump To SearchJohn Vincen AnastacioNo ratings yet
- EMFT Assignment 5Document48 pagesEMFT Assignment 5M. HamzaNo ratings yet
- 17th Annual World Congress On Anti-Aging Medicine 23-25 April 2009, Orlando, Florida, USADocument4 pages17th Annual World Congress On Anti-Aging Medicine 23-25 April 2009, Orlando, Florida, USAOdessa FileNo ratings yet
- Unit-1 (B - MARCH 2022Document40 pagesUnit-1 (B - MARCH 2022Vibin SimonNo ratings yet
- 01 Physics and Chemistry of Radiation AbsorptionDocument16 pages01 Physics and Chemistry of Radiation AbsorptionmonphilicalNo ratings yet
- Laser TherapyDocument8 pagesLaser Therapyinrmpt77No ratings yet
- Physics of RadiationDocument8 pagesPhysics of Radiationalialahmedy24No ratings yet
- Practical Introduction to Laser DermatologyFrom EverandPractical Introduction to Laser DermatologyVishal MadanNo ratings yet
- KPSEA NominalRoll SCHDocument3 pagesKPSEA NominalRoll SCHjared odhiamboNo ratings yet
- Workbook For Developmental Communications 1 UNIT 6Document14 pagesWorkbook For Developmental Communications 1 UNIT 6soldadodeslealNo ratings yet
- Collection of Windows 10 Hidden Secret Registry TweaksDocument9 pagesCollection of Windows 10 Hidden Secret Registry TweaksLiyoNo ratings yet
- Steamshovel Press Issue 04Document60 pagesSteamshovel Press Issue 04liondog1No ratings yet
- Dial Plan Implementation: Introducing Call RoutingDocument180 pagesDial Plan Implementation: Introducing Call RoutingGuillermo Ex TottiNo ratings yet
- Veeam Certified Engineer 9.5 U4Document270 pagesVeeam Certified Engineer 9.5 U4Federico FernandezNo ratings yet
- HahayysDocument30 pagesHahayys2BGrp3Plaza, Anna MaeNo ratings yet
- Tve 8 Shielded Metal Arc WeldingDocument11 pagesTve 8 Shielded Metal Arc WeldingJOHN ALFRED MANANGGITNo ratings yet
- About Fish Farming in GoaDocument5 pagesAbout Fish Farming in Goashashi891965No ratings yet
- Internship Report On GPDocument45 pagesInternship Report On GPpavel2051No ratings yet
- Services Provided by Merchant BanksDocument4 pagesServices Provided by Merchant BanksParul PrasadNo ratings yet
- HW On Receivables CDocument5 pagesHW On Receivables CAmjad Rian MangondatoNo ratings yet
- Law and IT Assignment SEM IXDocument18 pagesLaw and IT Assignment SEM IXrenu tomarNo ratings yet
- Wedding Vows - What Do They Really MeanDocument28 pagesWedding Vows - What Do They Really Meanpsykosomatik0% (1)
- Jumo 60.2021Document12 pagesJumo 60.2021Roderikus Rendy MNo ratings yet
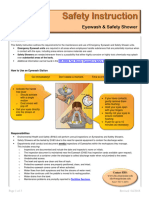
- Eyewash and Safety Shower SiDocument3 pagesEyewash and Safety Shower SiAli EsmaeilbeygiNo ratings yet
- Palanca vs. CADocument16 pagesPalanca vs. CASherwin Anoba CabutijaNo ratings yet
- Duration: 90 Days.: Fico Training ProgramDocument15 pagesDuration: 90 Days.: Fico Training ProgramMohammed Nawaz ShariffNo ratings yet
- Equinix Inc. 2022 Sustainability Report HighlightsDocument25 pagesEquinix Inc. 2022 Sustainability Report HighlightsDaniel ChuaNo ratings yet
- English Activity 1Document13 pagesEnglish Activity 1Mika ValenciaNo ratings yet
- Panadent SystemDocument70 pagesPanadent SystemDhananjay GandageNo ratings yet
- Annex VI - Final Narrative ReportDocument4 pagesAnnex VI - Final Narrative ReporttijanagruNo ratings yet
- Day 2UNQ3-1.docx..bakDocument13 pagesDay 2UNQ3-1.docx..bakAurellia Shafitri100% (1)
- Ho Yi Ying, Lau Hong Ming, Low Zi Chin, Ryan Chew Chun Nan, Sharleen Yeo YeeDocument2 pagesHo Yi Ying, Lau Hong Ming, Low Zi Chin, Ryan Chew Chun Nan, Sharleen Yeo YeesharleenNo ratings yet
- Earth and Lice Science Quarter 2 BrochureDocument2 pagesEarth and Lice Science Quarter 2 BrochureCamille NavorNo ratings yet
- Form For Scholarship From INBA PDFDocument5 pagesForm For Scholarship From INBA PDFAjay SinghNo ratings yet