Download as pptx, pdf, or txt
You might also like
- Pediatric Case PresentationDocument53 pagesPediatric Case PresentationCitrus100% (6)
- 01 - Newborn Physical ExamDocument2 pages01 - Newborn Physical Examgerald_valeriano0% (1)
- Newborn ExaminationDocument45 pagesNewborn ExaminationHamka HamNo ratings yet
- Parasitology Guide Questions 1Document2 pagesParasitology Guide Questions 1Cess LacatangoNo ratings yet
- Dengue Case Pres JervyDocument40 pagesDengue Case Pres JervyJervy GarciaNo ratings yet
- Presented By: Leena Siddiqui Zahra Abbas Faiza IftikharDocument46 pagesPresented By: Leena Siddiqui Zahra Abbas Faiza IftikharZahra MotorwalaNo ratings yet
- Preskas Abses MammaeDocument40 pagesPreskas Abses MammaeGesti Pratiwi HerlambangNo ratings yet
- Pediatrics Department Case Presentation Irah Franz D. Flores Block I Group DDocument56 pagesPediatrics Department Case Presentation Irah Franz D. Flores Block I Group DIrah FloresNo ratings yet
- Typhoid Case PresentationDocument79 pagesTyphoid Case PresentationJulius Dominique L. AnjaoNo ratings yet
- Pcapreport 140325070411 Phpapp02Document65 pagesPcapreport 140325070411 Phpapp02Anton RossiniNo ratings yet
- AAA - Nelsons 20th Summary Part 2Document122 pagesAAA - Nelsons 20th Summary Part 2Jessica MarianoNo ratings yet
- Scarlet FeverDocument74 pagesScarlet FeverPerly Lao-anes Wasit RunesNo ratings yet
- Physical Examination of The NewbornDocument7 pagesPhysical Examination of The NewbornurhighnxssNo ratings yet
- Measles: BY Mudaliar, Kannaan Anandasundar Mundale, Minal Vinod Munusamy, TamilarasiDocument48 pagesMeasles: BY Mudaliar, Kannaan Anandasundar Mundale, Minal Vinod Munusamy, TamilarasiKannaanNo ratings yet
- Case (Rhinitis Alergi) 2Document38 pagesCase (Rhinitis Alergi) 2christopherNo ratings yet
- AmoebaDocument24 pagesAmoebaJameh RomancapNo ratings yet
- Demam Ruam: Della Rizki Anggilia 18105Document40 pagesDemam Ruam: Della Rizki Anggilia 18105Della Rizki AnggiliaNo ratings yet
- Pre-Operative Conference Anesthetic Considerations For Laryngectomy and Total Thyroidectomy in GeriatricsDocument4 pagesPre-Operative Conference Anesthetic Considerations For Laryngectomy and Total Thyroidectomy in GeriatricsBhi-An BatobalonosNo ratings yet
- Dengue With Warning Signs: Hazel Mae B. ValdezDocument19 pagesDengue With Warning Signs: Hazel Mae B. ValdezMichelle Vera GabunNo ratings yet
- Identifying Data: DOB: Feb. 7, 2016Document31 pagesIdentifying Data: DOB: Feb. 7, 2016Malou Yap BuotNo ratings yet
- Subcutaneous EmphysemaDocument95 pagesSubcutaneous EmphysemaRaina AbadNo ratings yet
- Group B Sub Block 1: Capuyan, Candelaria, Cariaso, Carlos, Castilllo, ClavillasDocument37 pagesGroup B Sub Block 1: Capuyan, Candelaria, Cariaso, Carlos, Castilllo, ClavillasJean Michael CastilloNo ratings yet
- Case PresentationDocument32 pagesCase PresentationAGF Pallets MakerNo ratings yet
- Dengue Pedia MMCDocument26 pagesDengue Pedia MMCPatrick DycocoNo ratings yet
- Lupus Case PresentationDocument48 pagesLupus Case PresentationRoscelie KhoNo ratings yet
- AUBNDocument54 pagesAUBNJohn Christopher LucesNo ratings yet
- DengueDocument20 pagesDenguealpha mae beltranNo ratings yet
- Presentation Title: Arcilla-Beltran-Caagbay-LinaDocument20 pagesPresentation Title: Arcilla-Beltran-Caagbay-Linaalpha mae beltranNo ratings yet
- New Born Assess PPT FrankDocument118 pagesNew Born Assess PPT FrankPooja HardiyaNo ratings yet
- Skin Case TEN NEWDocument85 pagesSkin Case TEN NEWArianne Rizamaye BaysaNo ratings yet
- Pgi Hemorrhoids PresentationDocument41 pagesPgi Hemorrhoids PresentationIkea BalhonNo ratings yet
- Case Management: Leira Dith R. Castro, MD Presentor 1 Year Im ResidentDocument64 pagesCase Management: Leira Dith R. Castro, MD Presentor 1 Year Im ResidentAlvin Germo PasuquinNo ratings yet
- Clinical Case: Section A - Group 8Document68 pagesClinical Case: Section A - Group 8madison Deli100% (1)
- Case Presentation TetanusDocument15 pagesCase Presentation TetanusukhtianitaNo ratings yet
- Futuristic Background by SlidesgoDocument35 pagesFuturistic Background by SlidesgoI.k sidneyNo ratings yet
- B6 - Surgery GS II Case IIDocument10 pagesB6 - Surgery GS II Case IIGregNo ratings yet
- Physical Examination of The NewbornDocument70 pagesPhysical Examination of The NewbornBeaflor Javier CaldozoNo ratings yet
- Clinical Case - 2019: Alvin Germo PasuquinDocument49 pagesClinical Case - 2019: Alvin Germo PasuquinAlvin Germo PasuquinNo ratings yet
- Leaflet Gizi Buruk Wi2ngDocument36 pagesLeaflet Gizi Buruk Wi2ngAngga PahNo ratings yet
- Case MalariaDocument58 pagesCase MalariaHade Guntur SNo ratings yet
- NELLIUsMEDICAL 1Document29 pagesNELLIUsMEDICAL 1nellius mutindiNo ratings yet
- Hydrops of The GB in Children-HamilDocument29 pagesHydrops of The GB in Children-HamilApmc SchwartzNo ratings yet
- Pembimbing: Dr. Fadjar Nugroho - SP ADocument40 pagesPembimbing: Dr. Fadjar Nugroho - SP Asteve daresonNo ratings yet
- A Comprehensive Neurological Examination Guide and Approach To LocalizationDocument86 pagesA Comprehensive Neurological Examination Guide and Approach To LocalizationLiberty AgcaoiliNo ratings yet
- Surgery Ww3 DoneDocument22 pagesSurgery Ww3 DoneGopagoni PrekshmaNo ratings yet
- Vertigo/dizziness, (-) EpistaxisDocument3 pagesVertigo/dizziness, (-) EpistaxisAnonymous 1PxmDkmnNo ratings yet
- Differential Diagnosis of Dengue With Rash: Illness History Exam TestsDocument1 pageDifferential Diagnosis of Dengue With Rash: Illness History Exam Testsabbhyasa5206No ratings yet
- Protocol VHD in PregnancyDocument13 pagesProtocol VHD in PregnancyAmelie Crislyd Lopez AvenidoNo ratings yet
- Case Conference Monday Night Shift, March 16 2019Document42 pagesCase Conference Monday Night Shift, March 16 2019delfiaNo ratings yet
- Synapse in My Pocket Neuro Exam & Localization - 1st Ed 2020Document63 pagesSynapse in My Pocket Neuro Exam & Localization - 1st Ed 2020SnowyNo ratings yet
- B6 - Surgery GS II Case 1Document9 pagesB6 - Surgery GS II Case 1GregNo ratings yet
- CC 14 Mei 2017 Diare AkutDocument31 pagesCC 14 Mei 2017 Diare AkutDwi Pratika AnjarwatiNo ratings yet
- Pulmonary Tuberculos IS: PGI Aquino Ruel Aldrin PGI Andaman Greg JinichiDocument79 pagesPulmonary Tuberculos IS: PGI Aquino Ruel Aldrin PGI Andaman Greg JinichiIggs AndamanNo ratings yet
- New Born AssessmentDocument42 pagesNew Born AssessmentBhawna Joshi100% (3)
- Case Presentati On: Sevilla, Loreanne Novem Silim, Miriam Grace DDocument18 pagesCase Presentati On: Sevilla, Loreanne Novem Silim, Miriam Grace DKen StarNo ratings yet
- Pedia SGD NICUDocument62 pagesPedia SGD NICUJAIRISH YZABELLE SALVADORNo ratings yet
- Team C Final Written OutputDocument22 pagesTeam C Final Written OutputCarina SuarezNo ratings yet
- Ent Case PresentationDocument21 pagesEnt Case PresentationswitimahaleNo ratings yet
- Family Medicine Eor Exam Study Guide WebsiteDocument91 pagesFamily Medicine Eor Exam Study Guide WebsiteRanjani ammuNo ratings yet
- Newborn Care LectureDocument65 pagesNewborn Care LectureNichole daFonsecaNo ratings yet
- Action with the Elderly: A Handbook for Relatives and FriendsFrom EverandAction with the Elderly: A Handbook for Relatives and FriendsNo ratings yet
- Medico-Legal Questions in Intracranial InjuriesDocument15 pagesMedico-Legal Questions in Intracranial InjuriesJervy GarciaNo ratings yet
- Family CaseDocument42 pagesFamily CaseJervy GarciaNo ratings yet
- BreastfeedingDocument12 pagesBreastfeedingJervy GarciaNo ratings yet
- Dystocia NewpptxDocument6 pagesDystocia NewpptxJervy GarciaNo ratings yet
- HYPERTHYROIDISMDocument51 pagesHYPERTHYROIDISMJervy GarciaNo ratings yet
- HPNDocument55 pagesHPNJervy GarciaNo ratings yet
- Dengue Case Pres JervyDocument40 pagesDengue Case Pres JervyJervy GarciaNo ratings yet
- Cholecystitis TXDocument6 pagesCholecystitis TXJervy GarciaNo ratings yet
- Experiment #5 - Isolation of Normal FloraDocument9 pagesExperiment #5 - Isolation of Normal FloraFrancis MagbitangNo ratings yet
- EDocument3 pagesEMạc Huyền TrânNo ratings yet
- Mantoux Test-Method, Indications, PitfallsDocument8 pagesMantoux Test-Method, Indications, PitfallsJyothika SanalNo ratings yet
- Mariano Marcos State University: College of EngineeringDocument2 pagesMariano Marcos State University: College of EngineeringElvira JuanNo ratings yet
- Time Zone, Travel Doc, Health and Safety TestDocument6 pagesTime Zone, Travel Doc, Health and Safety Testnkurisobaloyi31No ratings yet
- Streptococcus - Biochemical ReactionsDocument37 pagesStreptococcus - Biochemical Reactionsdinahzaqout100% (2)
- Krok Made SimpleDocument16 pagesKrok Made SimplePrashant Singh100% (1)
- Written by Yamin Khan, PHD and Sarah Tilly: NtroductionDocument10 pagesWritten by Yamin Khan, PHD and Sarah Tilly: NtroductionChikezie OnwukweNo ratings yet
- NematodesDocument4 pagesNematodesPrincess Shaina CanapeNo ratings yet
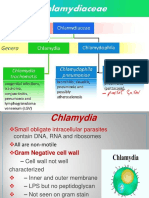
- Chlamydia&Rickettsia 2023Document29 pagesChlamydia&Rickettsia 2023Alhassn NasserNo ratings yet
- 9P-CHN, IMCI, COPAR Post Test-PrintDocument5 pages9P-CHN, IMCI, COPAR Post Test-PrintPaul Andrew VioletaNo ratings yet
- Pathogenic Microorganisms BrochureDocument2 pagesPathogenic Microorganisms Brochureapi-316071223No ratings yet
- NCM 104 Lec Syllabus MELDocument5 pagesNCM 104 Lec Syllabus MELLanz LlnsNo ratings yet
- Kenya General Travel InformationDocument2 pagesKenya General Travel InformationRaghdaNo ratings yet
- Henoch Schoenlein PurpuraDocument10 pagesHenoch Schoenlein PurpuraAlberto Kenyo Riofrio PalaciosNo ratings yet
- Mycology Reviewer 2022Document13 pagesMycology Reviewer 2022Love LeeNo ratings yet
- The Difference in Effectiveness of Increasing Doses of Cymbopogon (Lemongrass) Extract When Utilized As A Mosquito RepellentDocument22 pagesThe Difference in Effectiveness of Increasing Doses of Cymbopogon (Lemongrass) Extract When Utilized As A Mosquito RepellentKhristine GelNo ratings yet
- 2007 Sa Sawma Wound Cleansing and Dressing Procedure Nov 07Document23 pages2007 Sa Sawma Wound Cleansing and Dressing Procedure Nov 07Kristine Artes AguilarNo ratings yet
- Full Blown Porposal ManuscriptDocument29 pagesFull Blown Porposal ManuscriptJulian Valmorida Torralba IINo ratings yet
- 1996 PeterH - Duesberg Inventingthe AIDSvirusDocument724 pages1996 PeterH - Duesberg Inventingthe AIDSvirusJuan Manuel López VillatoroNo ratings yet
- Health in Germany - SummaryDocument13 pagesHealth in Germany - SummaryMb88No ratings yet
- Report-Slaughter Workshop - Richard - Klottey - BotchwayDocument11 pagesReport-Slaughter Workshop - Richard - Klottey - BotchwayRichard Klottey BotchwayNo ratings yet
- IMMUNOPROPHYLAXIS PPT PPTMDocument21 pagesIMMUNOPROPHYLAXIS PPT PPTMprerna12jainNo ratings yet
- Antifolate Drugs: Sulfonamides: Pharmacology IvDocument22 pagesAntifolate Drugs: Sulfonamides: Pharmacology IvShashidharan MenonNo ratings yet
- MCQ 14 Juli 2021 + Pembahasan FINALDocument50 pagesMCQ 14 Juli 2021 + Pembahasan FINALAnonymous pJxkvPQgNo ratings yet
- Microbiology Questions and AnswersDocument10 pagesMicrobiology Questions and AnswersFaidat AdekoyejoNo ratings yet
- AFA FoodFishProcessing7-8 Q0 LAS7 FINALDocument15 pagesAFA FoodFishProcessing7-8 Q0 LAS7 FINALMari PagxNo ratings yet
- Phylum: Sub-Phylum: (Sporozoa) Infective Agent:: Protozoa ApicomplexaDocument42 pagesPhylum: Sub-Phylum: (Sporozoa) Infective Agent:: Protozoa Apicomplexacharway_2000No ratings yet
- LMA Model Communicable Disease Clauses - August 2021Document3 pagesLMA Model Communicable Disease Clauses - August 2021Ludger MoraesNo ratings yet