
Poisoning in Children
Poisoning in Children
You might also like
- Taei ManualDocument126 pagesTaei Manualsenthil rajaNo ratings yet
- Forensic ToxicologyDocument165 pagesForensic Toxicologyapi-3763814100% (5)
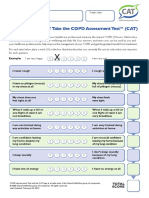
- How Is Your Copd? Take The Copd Assessmenttest (Cat) : Your Name: Today'S DateDocument1 pageHow Is Your Copd? Take The Copd Assessmenttest (Cat) : Your Name: Today'S DateAndreea BurceaNo ratings yet
- Acute Respiratory Failure CPDocument89 pagesAcute Respiratory Failure CPandymaze50% (2)
- PoisoningDocument103 pagesPoisoningC Hendra Wijaya100% (2)
- Poisoning in Children 3Document47 pagesPoisoning in Children 3HussamNo ratings yet
- General ToxicologyDocument57 pagesGeneral ToxicologyOhoodNo ratings yet
- Teacher In-Charge Dr. A. PRAKASH, M.Pharm (Pharmacology), PHD (Nitc)Document34 pagesTeacher In-Charge Dr. A. PRAKASH, M.Pharm (Pharmacology), PHD (Nitc)Prakash AppaNo ratings yet
- A IntroductionDocument55 pagesA IntroductionYohanes FirmansyahNo ratings yet
- Title Layout: SubtitleDocument73 pagesTitle Layout: Subtitlenaila100% (1)
- 1-Poisoning in Children Revised 2021Document63 pages1-Poisoning in Children Revised 2021Jawaher AbdullahNo ratings yet
- 2019 Purdue Tox LectureDocument138 pages2019 Purdue Tox Lectureapi-665372449No ratings yet
- Accidental Poisoning in Children: AbstractDocument6 pagesAccidental Poisoning in Children: Abstractkenikirkucing2No ratings yet
- Introduction To Toxicology: Richard R. Rediske, Ph.D. Annis Water Resources Institute Grand Valley State UniversityDocument57 pagesIntroduction To Toxicology: Richard R. Rediske, Ph.D. Annis Water Resources Institute Grand Valley State UniversityDyah Ayu pramoda wardaniNo ratings yet
- Forensic ToxicologyDocument165 pagesForensic ToxicologyRoman Mamun100% (2)
- ENV 107 Env HLTH & Toxicology FinalDocument36 pagesENV 107 Env HLTH & Toxicology FinalNumayer Ahmed ChaudhuriNo ratings yet
- Forensic ToxicologyDocument165 pagesForensic ToxicologyAnonymous 6QBs1MSiNo ratings yet
- Medip, IJCP-808 O-1Document6 pagesMedip, IJCP-808 O-1KaleEgziabher LukasNo ratings yet
- R.P 5Document6 pagesR.P 5Poma PanezaiNo ratings yet
- Lec1 PDFDocument45 pagesLec1 PDFMichael Andre CorosNo ratings yet
- Year 10 Medicinal Chemistry: The Research and Development of New DrugsDocument14 pagesYear 10 Medicinal Chemistry: The Research and Development of New DrugsParsnip with ParsleyNo ratings yet
- Fundamentals of Toxicology: Sri Hainil, S.Si, M.farm, AptDocument39 pagesFundamentals of Toxicology: Sri Hainil, S.Si, M.farm, AptlyanaNo ratings yet
- Introduction To ToxicologyDocument18 pagesIntroduction To ToxicologyMompati Letsweletse100% (1)
- General Considerations On Toxicology - To Send For 2021admDocument66 pagesGeneral Considerations On Toxicology - To Send For 2021admhadiyaNo ratings yet
- Clinical ToxicologyDocument36 pagesClinical ToxicologyMuhammad FawadNo ratings yet
- Rahul Kamble Pediatrics Article 1Document9 pagesRahul Kamble Pediatrics Article 1Rahul KambleNo ratings yet
- PoisoningDocument35 pagesPoisoningMUKESH SUNDARARAJANNo ratings yet
- Pediatric PoisoningsDocument45 pagesPediatric PoisoningsErwin Jake Taguba100% (1)
- Lesson 8 Envi SciDocument29 pagesLesson 8 Envi SciJoven EstebanNo ratings yet
- Poison ResearchDocument6 pagesPoison Researchjosephbal948No ratings yet
- Poisoning: Risk FactorsDocument2 pagesPoisoning: Risk FactorsPauline Mae RobertoNo ratings yet
- Testing For Pesticides in Food and Supplements Is Necessary by Teri ArrangaDocument6 pagesTesting For Pesticides in Food and Supplements Is Necessary by Teri ArrangaautismoneNo ratings yet
- NSTP Finals1Document244 pagesNSTP Finals1Rei EnclonaNo ratings yet
- Toxicology S16Document67 pagesToxicology S16Smiley MinkeyNo ratings yet
- 10 Emergency TreatmentDocument62 pages10 Emergency TreatmentShah NAWAZNo ratings yet
- Principles of ToxicologyDocument64 pagesPrinciples of ToxicologyMarie SarangayaNo ratings yet
- Drugs and Substance AbuseDocument15 pagesDrugs and Substance AbuseEve Lexy MutituNo ratings yet
- Emergency Poisoning FinalDocument81 pagesEmergency Poisoning FinalMohammed Gazo100% (2)
- Spraying Pesticides HazardDocument15 pagesSpraying Pesticides HazardJulio PutraNo ratings yet
- 1 Introduction PDFDocument20 pages1 Introduction PDFAll Furqaniya ChannelNo ratings yet
- 65 249 1 PBDocument4 pages65 249 1 PBJatin SinghNo ratings yet
- Presented by Malar Kodi. S M.SC (N) Ii Year DR - Syamala Reedy College of NursingDocument40 pagesPresented by Malar Kodi. S M.SC (N) Ii Year DR - Syamala Reedy College of NursingamulaathiNo ratings yet
- Sharma Et Al PDFDocument5 pagesSharma Et Al PDFKiki KikukNo ratings yet
- Cdi 5 PresentationDocument108 pagesCdi 5 PresentationJoann JacobNo ratings yet
- Is Poisoning A Problem in South Sudan?: Main ArticlesDocument2 pagesIs Poisoning A Problem in South Sudan?: Main ArticlesSwetank SinghNo ratings yet
- Nicolas, Krizha Assignment EdDocument1 pageNicolas, Krizha Assignment EdKrizha Angela NicolasNo ratings yet
- ToxicityDocument28 pagesToxicitymonasteriomatthew7No ratings yet
- Process Biochemistry: Nigar Anzar, Shariq Suleman, Suhel Parvez, Jagriti NarangDocument12 pagesProcess Biochemistry: Nigar Anzar, Shariq Suleman, Suhel Parvez, Jagriti NarangVivek MehtaNo ratings yet
- Presentation Hamed (Pesticide)Document27 pagesPresentation Hamed (Pesticide)Hamed GharibiNo ratings yet
- Practical ToxicologyDocument28 pagesPractical ToxicologyEm SimantaNo ratings yet
- General Approach 1 الدلتاDocument104 pagesGeneral Approach 1 الدلتاDr Mokhtar MokhtarNo ratings yet
- Original Research Paper Community MedicineDocument2 pagesOriginal Research Paper Community MedicinekouserNo ratings yet
- TextDocument91 pagesTextvinoth7437100% (1)
- Review PaperDocument7 pagesReview Papers3351415057No ratings yet
- Scenario of Poisoning Cases in Adults Admitted in Manipal Teaching Hospital, Pokhara, NepalDocument4 pagesScenario of Poisoning Cases in Adults Admitted in Manipal Teaching Hospital, Pokhara, NepalAzman HakimNo ratings yet
- Factor Affecting Poisoning: Submitted To: Dr. Muhammad Fawad Rasool Submitted byDocument18 pagesFactor Affecting Poisoning: Submitted To: Dr. Muhammad Fawad Rasool Submitted byXtylish RajpootNo ratings yet
- Drug-Addiction-Biology ProjectDocument37 pagesDrug-Addiction-Biology ProjectAhalya Bai SahooNo ratings yet
- Drug Addiction - Biology Science Fair Project IdeasDocument11 pagesDrug Addiction - Biology Science Fair Project IdeasSwaraj KhedekarNo ratings yet
- Inhalant-Related Disorders (Pathology A2)Document15 pagesInhalant-Related Disorders (Pathology A2)Aliza AliNo ratings yet
- NSTP 2: Cwts Part 6 - Part 12Document36 pagesNSTP 2: Cwts Part 6 - Part 12Carl GilNo ratings yet
- W13 Environmental Risk - PPTDocument26 pagesW13 Environmental Risk - PPTelforest07No ratings yet
- Healthy, Happy Baby: The essential guide to raising a toxin-free babyFrom EverandHealthy, Happy Baby: The essential guide to raising a toxin-free babyNo ratings yet
- Acute Management of StrokeDocument19 pagesAcute Management of StrokeBKGUBIONo ratings yet
- Management of Cardiac Emergencies in Dental PracticeDocument112 pagesManagement of Cardiac Emergencies in Dental PracticeMNSNo ratings yet
- Ebook Kanskis Synopsis of Clinical Ophthalmology PDF Full Chapter PDFDocument67 pagesEbook Kanskis Synopsis of Clinical Ophthalmology PDF Full Chapter PDFarchie.abney272100% (37)
- Abnormal Constituents of UrineDocument6 pagesAbnormal Constituents of UrinePurnima VermaNo ratings yet
- Spontaneous Coronary Artery Dissection With Clinical Presentation of Acute Myocardial InfarctionDocument3 pagesSpontaneous Coronary Artery Dissection With Clinical Presentation of Acute Myocardial InfarctionSabrina JonesNo ratings yet
- Seminar On PacemakerDocument14 pagesSeminar On Pacemakerjyothi50% (4)
- Clinical Manifestations of Antiphospholipid Syndrome - UpToDateDocument28 pagesClinical Manifestations of Antiphospholipid Syndrome - UpToDateBernas Arion NapitupuluNo ratings yet
- Clinph2 Amya Polytechnic College Inc 1Document3 pagesClinph2 Amya Polytechnic College Inc 1blehhh080No ratings yet
- AIT Convulsion FocalDocument2 pagesAIT Convulsion FocalOscar Alejandro Cardenas QuinteroNo ratings yet
- Assisting Central Venous Catheter (CVC) Insertion (Procedure1)Document7 pagesAssisting Central Venous Catheter (CVC) Insertion (Procedure1)BsBs A7medNo ratings yet
- JournalDocument4 pagesJournalfinity de diosNo ratings yet
- Neuro-Ophthalmology ICD-10 Quick Reference GuideDocument4 pagesNeuro-Ophthalmology ICD-10 Quick Reference GuideFaisal ApendixNo ratings yet
- C. Common Cardinal VeinsDocument6 pagesC. Common Cardinal VeinsTofik MohammedNo ratings yet
- Malkoff-x-Noninvasive BP-mice&rats PDFDocument12 pagesMalkoff-x-Noninvasive BP-mice&rats PDFMuhammadSajjadSarwarNo ratings yet
- Basic Life Support: Based On Guidelines byDocument28 pagesBasic Life Support: Based On Guidelines byshrithyNo ratings yet
- Sodium and PotassiumDocument4 pagesSodium and PotassiumLUALHATI VILLASNo ratings yet
- Personalized Acute Kidney Injury TreatmentDocument8 pagesPersonalized Acute Kidney Injury TreatmentGabriela PachecoNo ratings yet
- Hypoplastic Left Heart Syndrome - Group ProjectDocument24 pagesHypoplastic Left Heart Syndrome - Group Projectapi-301611629No ratings yet
- Cardiology - Corrected AhmedDocument23 pagesCardiology - Corrected AhmedHanadi UmhanayNo ratings yet
- Module - 6.advance 12 Lead InterpretationDocument30 pagesModule - 6.advance 12 Lead InterpretationFerry SofyanriNo ratings yet
- Aortic Stenosis: Measures of AS Severity Obtained by Doppler-EchocardiographyDocument1 pageAortic Stenosis: Measures of AS Severity Obtained by Doppler-EchocardiographyWayan GunawanNo ratings yet
- Basic Ecg: A Report By: Clinical Clerk Mary Hazel TeDocument74 pagesBasic Ecg: A Report By: Clinical Clerk Mary Hazel TeHazel Arcosa100% (1)
- HER CCB in Crisis HypertensionDocument22 pagesHER CCB in Crisis HypertensionHandi Wijaya HasanNo ratings yet
- NCLEX Review: Pharmacology Charlene Natale, BSN, RNDocument43 pagesNCLEX Review: Pharmacology Charlene Natale, BSN, RNMenly Susada100% (1)
- Hema 2Document31 pagesHema 2Mark SyNo ratings yet
- Physical Examination Techniques and ManueversDocument160 pagesPhysical Examination Techniques and ManueversMa-anJaneDiamosNo ratings yet
- Aortic Valve RegurgitationDocument3 pagesAortic Valve RegurgitationMarky StrikerNo ratings yet




















































































Download as ppt, pdf, or txt
You might also like
- Taei ManualDocument126 pagesTaei Manualsenthil rajaNo ratings yet
- Forensic ToxicologyDocument165 pagesForensic Toxicologyapi-3763814100% (5)
- How Is Your Copd? Take The Copd Assessmenttest (Cat) : Your Name: Today'S DateDocument1 pageHow Is Your Copd? Take The Copd Assessmenttest (Cat) : Your Name: Today'S DateAndreea BurceaNo ratings yet
- Acute Respiratory Failure CPDocument89 pagesAcute Respiratory Failure CPandymaze50% (2)
- PoisoningDocument103 pagesPoisoningC Hendra Wijaya100% (2)
- Poisoning in Children 3Document47 pagesPoisoning in Children 3HussamNo ratings yet
- General ToxicologyDocument57 pagesGeneral ToxicologyOhoodNo ratings yet
- Teacher In-Charge Dr. A. PRAKASH, M.Pharm (Pharmacology), PHD (Nitc)Document34 pagesTeacher In-Charge Dr. A. PRAKASH, M.Pharm (Pharmacology), PHD (Nitc)Prakash AppaNo ratings yet
- A IntroductionDocument55 pagesA IntroductionYohanes FirmansyahNo ratings yet
- Title Layout: SubtitleDocument73 pagesTitle Layout: Subtitlenaila100% (1)
- 1-Poisoning in Children Revised 2021Document63 pages1-Poisoning in Children Revised 2021Jawaher AbdullahNo ratings yet
- 2019 Purdue Tox LectureDocument138 pages2019 Purdue Tox Lectureapi-665372449No ratings yet
- Accidental Poisoning in Children: AbstractDocument6 pagesAccidental Poisoning in Children: Abstractkenikirkucing2No ratings yet
- Introduction To Toxicology: Richard R. Rediske, Ph.D. Annis Water Resources Institute Grand Valley State UniversityDocument57 pagesIntroduction To Toxicology: Richard R. Rediske, Ph.D. Annis Water Resources Institute Grand Valley State UniversityDyah Ayu pramoda wardaniNo ratings yet
- Forensic ToxicologyDocument165 pagesForensic ToxicologyRoman Mamun100% (2)
- ENV 107 Env HLTH & Toxicology FinalDocument36 pagesENV 107 Env HLTH & Toxicology FinalNumayer Ahmed ChaudhuriNo ratings yet
- Forensic ToxicologyDocument165 pagesForensic ToxicologyAnonymous 6QBs1MSiNo ratings yet
- Medip, IJCP-808 O-1Document6 pagesMedip, IJCP-808 O-1KaleEgziabher LukasNo ratings yet
- R.P 5Document6 pagesR.P 5Poma PanezaiNo ratings yet
- Lec1 PDFDocument45 pagesLec1 PDFMichael Andre CorosNo ratings yet
- Year 10 Medicinal Chemistry: The Research and Development of New DrugsDocument14 pagesYear 10 Medicinal Chemistry: The Research and Development of New DrugsParsnip with ParsleyNo ratings yet
- Fundamentals of Toxicology: Sri Hainil, S.Si, M.farm, AptDocument39 pagesFundamentals of Toxicology: Sri Hainil, S.Si, M.farm, AptlyanaNo ratings yet
- Introduction To ToxicologyDocument18 pagesIntroduction To ToxicologyMompati Letsweletse100% (1)
- General Considerations On Toxicology - To Send For 2021admDocument66 pagesGeneral Considerations On Toxicology - To Send For 2021admhadiyaNo ratings yet
- Clinical ToxicologyDocument36 pagesClinical ToxicologyMuhammad FawadNo ratings yet
- Rahul Kamble Pediatrics Article 1Document9 pagesRahul Kamble Pediatrics Article 1Rahul KambleNo ratings yet
- PoisoningDocument35 pagesPoisoningMUKESH SUNDARARAJANNo ratings yet
- Pediatric PoisoningsDocument45 pagesPediatric PoisoningsErwin Jake Taguba100% (1)
- Lesson 8 Envi SciDocument29 pagesLesson 8 Envi SciJoven EstebanNo ratings yet
- Poison ResearchDocument6 pagesPoison Researchjosephbal948No ratings yet
- Poisoning: Risk FactorsDocument2 pagesPoisoning: Risk FactorsPauline Mae RobertoNo ratings yet
- Testing For Pesticides in Food and Supplements Is Necessary by Teri ArrangaDocument6 pagesTesting For Pesticides in Food and Supplements Is Necessary by Teri ArrangaautismoneNo ratings yet
- NSTP Finals1Document244 pagesNSTP Finals1Rei EnclonaNo ratings yet
- Toxicology S16Document67 pagesToxicology S16Smiley MinkeyNo ratings yet
- 10 Emergency TreatmentDocument62 pages10 Emergency TreatmentShah NAWAZNo ratings yet
- Principles of ToxicologyDocument64 pagesPrinciples of ToxicologyMarie SarangayaNo ratings yet
- Drugs and Substance AbuseDocument15 pagesDrugs and Substance AbuseEve Lexy MutituNo ratings yet
- Emergency Poisoning FinalDocument81 pagesEmergency Poisoning FinalMohammed Gazo100% (2)
- Spraying Pesticides HazardDocument15 pagesSpraying Pesticides HazardJulio PutraNo ratings yet
- 1 Introduction PDFDocument20 pages1 Introduction PDFAll Furqaniya ChannelNo ratings yet
- 65 249 1 PBDocument4 pages65 249 1 PBJatin SinghNo ratings yet
- Presented by Malar Kodi. S M.SC (N) Ii Year DR - Syamala Reedy College of NursingDocument40 pagesPresented by Malar Kodi. S M.SC (N) Ii Year DR - Syamala Reedy College of NursingamulaathiNo ratings yet
- Sharma Et Al PDFDocument5 pagesSharma Et Al PDFKiki KikukNo ratings yet
- Cdi 5 PresentationDocument108 pagesCdi 5 PresentationJoann JacobNo ratings yet
- Is Poisoning A Problem in South Sudan?: Main ArticlesDocument2 pagesIs Poisoning A Problem in South Sudan?: Main ArticlesSwetank SinghNo ratings yet
- Nicolas, Krizha Assignment EdDocument1 pageNicolas, Krizha Assignment EdKrizha Angela NicolasNo ratings yet
- ToxicityDocument28 pagesToxicitymonasteriomatthew7No ratings yet
- Process Biochemistry: Nigar Anzar, Shariq Suleman, Suhel Parvez, Jagriti NarangDocument12 pagesProcess Biochemistry: Nigar Anzar, Shariq Suleman, Suhel Parvez, Jagriti NarangVivek MehtaNo ratings yet
- Presentation Hamed (Pesticide)Document27 pagesPresentation Hamed (Pesticide)Hamed GharibiNo ratings yet
- Practical ToxicologyDocument28 pagesPractical ToxicologyEm SimantaNo ratings yet
- General Approach 1 الدلتاDocument104 pagesGeneral Approach 1 الدلتاDr Mokhtar MokhtarNo ratings yet
- Original Research Paper Community MedicineDocument2 pagesOriginal Research Paper Community MedicinekouserNo ratings yet
- TextDocument91 pagesTextvinoth7437100% (1)
- Review PaperDocument7 pagesReview Papers3351415057No ratings yet
- Scenario of Poisoning Cases in Adults Admitted in Manipal Teaching Hospital, Pokhara, NepalDocument4 pagesScenario of Poisoning Cases in Adults Admitted in Manipal Teaching Hospital, Pokhara, NepalAzman HakimNo ratings yet
- Factor Affecting Poisoning: Submitted To: Dr. Muhammad Fawad Rasool Submitted byDocument18 pagesFactor Affecting Poisoning: Submitted To: Dr. Muhammad Fawad Rasool Submitted byXtylish RajpootNo ratings yet
- Drug-Addiction-Biology ProjectDocument37 pagesDrug-Addiction-Biology ProjectAhalya Bai SahooNo ratings yet
- Drug Addiction - Biology Science Fair Project IdeasDocument11 pagesDrug Addiction - Biology Science Fair Project IdeasSwaraj KhedekarNo ratings yet
- Inhalant-Related Disorders (Pathology A2)Document15 pagesInhalant-Related Disorders (Pathology A2)Aliza AliNo ratings yet
- NSTP 2: Cwts Part 6 - Part 12Document36 pagesNSTP 2: Cwts Part 6 - Part 12Carl GilNo ratings yet
- W13 Environmental Risk - PPTDocument26 pagesW13 Environmental Risk - PPTelforest07No ratings yet
- Healthy, Happy Baby: The essential guide to raising a toxin-free babyFrom EverandHealthy, Happy Baby: The essential guide to raising a toxin-free babyNo ratings yet
- Acute Management of StrokeDocument19 pagesAcute Management of StrokeBKGUBIONo ratings yet
- Management of Cardiac Emergencies in Dental PracticeDocument112 pagesManagement of Cardiac Emergencies in Dental PracticeMNSNo ratings yet
- Ebook Kanskis Synopsis of Clinical Ophthalmology PDF Full Chapter PDFDocument67 pagesEbook Kanskis Synopsis of Clinical Ophthalmology PDF Full Chapter PDFarchie.abney272100% (37)
- Abnormal Constituents of UrineDocument6 pagesAbnormal Constituents of UrinePurnima VermaNo ratings yet
- Spontaneous Coronary Artery Dissection With Clinical Presentation of Acute Myocardial InfarctionDocument3 pagesSpontaneous Coronary Artery Dissection With Clinical Presentation of Acute Myocardial InfarctionSabrina JonesNo ratings yet
- Seminar On PacemakerDocument14 pagesSeminar On Pacemakerjyothi50% (4)
- Clinical Manifestations of Antiphospholipid Syndrome - UpToDateDocument28 pagesClinical Manifestations of Antiphospholipid Syndrome - UpToDateBernas Arion NapitupuluNo ratings yet
- Clinph2 Amya Polytechnic College Inc 1Document3 pagesClinph2 Amya Polytechnic College Inc 1blehhh080No ratings yet
- AIT Convulsion FocalDocument2 pagesAIT Convulsion FocalOscar Alejandro Cardenas QuinteroNo ratings yet
- Assisting Central Venous Catheter (CVC) Insertion (Procedure1)Document7 pagesAssisting Central Venous Catheter (CVC) Insertion (Procedure1)BsBs A7medNo ratings yet
- JournalDocument4 pagesJournalfinity de diosNo ratings yet
- Neuro-Ophthalmology ICD-10 Quick Reference GuideDocument4 pagesNeuro-Ophthalmology ICD-10 Quick Reference GuideFaisal ApendixNo ratings yet
- C. Common Cardinal VeinsDocument6 pagesC. Common Cardinal VeinsTofik MohammedNo ratings yet
- Malkoff-x-Noninvasive BP-mice&rats PDFDocument12 pagesMalkoff-x-Noninvasive BP-mice&rats PDFMuhammadSajjadSarwarNo ratings yet
- Basic Life Support: Based On Guidelines byDocument28 pagesBasic Life Support: Based On Guidelines byshrithyNo ratings yet
- Sodium and PotassiumDocument4 pagesSodium and PotassiumLUALHATI VILLASNo ratings yet
- Personalized Acute Kidney Injury TreatmentDocument8 pagesPersonalized Acute Kidney Injury TreatmentGabriela PachecoNo ratings yet
- Hypoplastic Left Heart Syndrome - Group ProjectDocument24 pagesHypoplastic Left Heart Syndrome - Group Projectapi-301611629No ratings yet
- Cardiology - Corrected AhmedDocument23 pagesCardiology - Corrected AhmedHanadi UmhanayNo ratings yet
- Module - 6.advance 12 Lead InterpretationDocument30 pagesModule - 6.advance 12 Lead InterpretationFerry SofyanriNo ratings yet
- Aortic Stenosis: Measures of AS Severity Obtained by Doppler-EchocardiographyDocument1 pageAortic Stenosis: Measures of AS Severity Obtained by Doppler-EchocardiographyWayan GunawanNo ratings yet
- Basic Ecg: A Report By: Clinical Clerk Mary Hazel TeDocument74 pagesBasic Ecg: A Report By: Clinical Clerk Mary Hazel TeHazel Arcosa100% (1)
- HER CCB in Crisis HypertensionDocument22 pagesHER CCB in Crisis HypertensionHandi Wijaya HasanNo ratings yet
- NCLEX Review: Pharmacology Charlene Natale, BSN, RNDocument43 pagesNCLEX Review: Pharmacology Charlene Natale, BSN, RNMenly Susada100% (1)
- Hema 2Document31 pagesHema 2Mark SyNo ratings yet
- Physical Examination Techniques and ManueversDocument160 pagesPhysical Examination Techniques and ManueversMa-anJaneDiamosNo ratings yet
- Aortic Valve RegurgitationDocument3 pagesAortic Valve RegurgitationMarky StrikerNo ratings yet