
Abdo. Viscera
Abdo. Viscera
You might also like
- 4 Peritoneum PDFDocument64 pages4 Peritoneum PDFN ANo ratings yet
- Peritoneum and Peritoneal CavityDocument26 pagesPeritoneum and Peritoneal CavitytuhinsinghNo ratings yet
- Hyperthermia (Thurs)Document1 pageHyperthermia (Thurs)Christine Esguerra OrozcoNo ratings yet
- Pathophysiology of Intestinal ObstructionDocument3 pagesPathophysiology of Intestinal ObstructionJOvie Rectin100% (2)
- Small IntestineDocument34 pagesSmall IntestineIAMSANWAR019170100% (1)
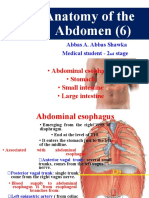
- Anatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineDocument34 pagesAnatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineBilal YimamNo ratings yet
- Abdomen - Esophagus To ColonDocument42 pagesAbdomen - Esophagus To ColonBibek GajmerNo ratings yet
- Ana SGD 15Document67 pagesAna SGD 15Bea ManzanoNo ratings yet
- Abdominal AnatomyDocument39 pagesAbdominal AnatomyRahul MandhanNo ratings yet
- 1 Abdominal VisceraDocument45 pages1 Abdominal VisceraMero HamedNo ratings yet
- Abdominal CavityDocument78 pagesAbdominal Cavitytanishapatel1005No ratings yet
- Small Intestine MMCDocument65 pagesSmall Intestine MMCWorku KifleNo ratings yet
- Abdomen Part IDocument110 pagesAbdomen Part IAbel GirmaNo ratings yet
- Anatomy of StomachDocument58 pagesAnatomy of StomachSkinny tuberNo ratings yet
- Anatomy of PeritoneumDocument61 pagesAnatomy of PeritoneumFirdaus SeptiawanNo ratings yet
- Stomach: DR Kavitha M Kjiar (Savli)Document52 pagesStomach: DR Kavitha M Kjiar (Savli)Dhaval Chauhan0% (1)
- LO1 Anatomy and Histology of Lower Gi TractDocument180 pagesLO1 Anatomy and Histology of Lower Gi TractIcarus WingsNo ratings yet
- Peritoneum 2022Document86 pagesPeritoneum 2022Tayyib KhanNo ratings yet
- 3 Stomach & Small Intestine Oct 2017Document50 pages3 Stomach & Small Intestine Oct 2017mayankNo ratings yet
- Abdomen.: Moore, Keith. Clinically Oriented Anatomy. Seventh Edition. Lippincott Williams & Wilkins. Baltimore. 2014Document58 pagesAbdomen.: Moore, Keith. Clinically Oriented Anatomy. Seventh Edition. Lippincott Williams & Wilkins. Baltimore. 2014Paola Solarte ChicaizaNo ratings yet
- The StomachDocument3 pagesThe StomachSanjay KishoreNo ratings yet
- Peritoneum: General FeaturesDocument92 pagesPeritoneum: General FeaturestuhinsinghNo ratings yet
- Duodenum and PancreaslectureDocument35 pagesDuodenum and PancreaslectureChigozie GeraldNo ratings yet
- Large IntestineDocument29 pagesLarge IntestineOlaifa victorNo ratings yet
- StomachDocument29 pagesStomachSupriti Verma Bhatnagar100% (1)
- AbdomenDocument142 pagesAbdomenleul TizazuNo ratings yet
- Anatomi Gaster Dan DuodenumDocument179 pagesAnatomi Gaster Dan DuodenumHaraka NabdaNo ratings yet
- GasterDocument179 pagesGasterAraka Patriota100% (1)
- ANAT 221 - PeritoneumDocument22 pagesANAT 221 - PeritoneumWisdom IkechukwuNo ratings yet
- Gross Anatomy of The Small IntestineDocument27 pagesGross Anatomy of The Small IntestineEniola DaramolaNo ratings yet
- Clinical Embriology and Anatomy of Gi Tract Part1Document44 pagesClinical Embriology and Anatomy of Gi Tract Part1trianaamalia100% (1)
- Upper GITDocument33 pagesUpper GITWahida Amalin Ab RazakNo ratings yet
- Colon CancerDocument38 pagesColon CancerUsmle GuyNo ratings yet
- Ac 2Document104 pagesAc 2saide limNo ratings yet
- The Small Intestine-1Document38 pagesThe Small Intestine-1ChiderahNo ratings yet
- Surgical Anatomy of PeritoneumDocument63 pagesSurgical Anatomy of PeritoneumSuvarna RajNo ratings yet
- Anatomy StomachDocument43 pagesAnatomy StomachBijo K BennyNo ratings yet
- Structures of The ForegutDocument13 pagesStructures of The ForegutJatan KothariNo ratings yet
- PeritoneumDocument31 pagesPeritoneumbravadoNo ratings yet
- Colorectal MalignancyDocument108 pagesColorectal MalignancySatishht SatishNo ratings yet
- General Arrangement of The Abdominal VisceraDocument30 pagesGeneral Arrangement of The Abdominal Visceraapi-249972919100% (2)
- STOMACHDocument18 pagesSTOMACHOlaifa victorNo ratings yet
- PeritoneumDocument39 pagesPeritoneumtuhinsinghNo ratings yet
- Anatomy and Histology Gaster - DuodenumDocument149 pagesAnatomy and Histology Gaster - DuodenumRevila AuliaNo ratings yet
- Small IntestineDocument16 pagesSmall IntestineShimmering MoonNo ratings yet
- 4 The Stomach and The Abdominal EsophagusDocument43 pages4 The Stomach and The Abdominal EsophagusAbdullah HaroonNo ratings yet
- Clinical Embriology and Anatomy of Gi Tract Part1Document43 pagesClinical Embriology and Anatomy of Gi Tract Part1Luna LitamiNo ratings yet
- Digestive System (2015 - 06 - 09 20 - 43 - 48 Utc)Document90 pagesDigestive System (2015 - 06 - 09 20 - 43 - 48 Utc)DiazNo ratings yet
- Anat 221-Large IntestineDocument21 pagesAnat 221-Large IntestineWisdom IkechukwuNo ratings yet
- Anatomy of Small Intestine: Lecture-4Document23 pagesAnatomy of Small Intestine: Lecture-4Ahmed OudahNo ratings yet
- Anatomy of Digestive SystemDocument20 pagesAnatomy of Digestive Systemolive jollyNo ratings yet
- Anatomi Dan Histologi Saluran Cerna BawahDocument20 pagesAnatomi Dan Histologi Saluran Cerna BawahIlhamDevirxaNo ratings yet
- Blok GastrointestinalDocument103 pagesBlok GastrointestinalArLyne MakinNo ratings yet
- StomachDocument24 pagesStomachHarini KarthikeyanNo ratings yet
- GIS1 - K1,2 - Anatomi Dan EmbriologiDocument70 pagesGIS1 - K1,2 - Anatomi Dan EmbriologiNatasya Ryani PurbaNo ratings yet
- Digestive SystemDocument242 pagesDigestive SystemVansh SinghNo ratings yet
- Abdomen Kub Presentation (Autosaved)Document81 pagesAbdomen Kub Presentation (Autosaved)adhikariaashi2004No ratings yet
- Anatomy SpleenDocument32 pagesAnatomy SpleenBijo K BennyNo ratings yet
- Small Intestine 2017Document78 pagesSmall Intestine 2017yasrul izadNo ratings yet
- Rectum & Anal CanalDocument14 pagesRectum & Anal CanalLisa DentonNo ratings yet
- Anatomy of Jejunum, Ileum and Large Intestine: Dr. Mohammed Mahmoud MosaedDocument38 pagesAnatomy of Jejunum, Ileum and Large Intestine: Dr. Mohammed Mahmoud MosaedRakaNo ratings yet
- Intestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandIntestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Abdomen: DR Solomie Ayalew, M.D. Wolkite UniversityDocument177 pagesAbdomen: DR Solomie Ayalew, M.D. Wolkite UniversityDureti DuretiNo ratings yet
- Abdomen Wall-1Document86 pagesAbdomen Wall-1Dureti DuretiNo ratings yet
- Lec 6 Thorax - FinalDocument223 pagesLec 6 Thorax - FinalDureti DuretiNo ratings yet
- The Thorax-1 (Compatibility Mode)Document122 pagesThe Thorax-1 (Compatibility Mode)Dureti DuretiNo ratings yet
- Ocular Changes and Approaches of Ophthalmopathy in Basedow - Graves-Parry - Flajani DiseaseDocument7 pagesOcular Changes and Approaches of Ophthalmopathy in Basedow - Graves-Parry - Flajani Diseasesmartjohnsmith10No ratings yet
- 1st M&M 2013 Case Protocol - Shoulder Dystocia PDFDocument4 pages1st M&M 2013 Case Protocol - Shoulder Dystocia PDFAnonymous D7NzSe69kgNo ratings yet
- Female Reproductive OrgansDocument32 pagesFemale Reproductive Organsapi-19916399100% (1)
- Lisa Pang: Education TeachingDocument2 pagesLisa Pang: Education TeachingpangdaNo ratings yet
- Case Taking Form - Bashir Mahmud ElliasDocument5 pagesCase Taking Form - Bashir Mahmud ElliasBashir Mahmud ElliasNo ratings yet
- Vomiting in Children 2018 PDFDocument19 pagesVomiting in Children 2018 PDFSamuel DiazNo ratings yet
- AnatomyDocument4 pagesAnatomySureen PaduaNo ratings yet
- An Overview of Encapsulation Technologies For Food ApplicationsDocument11 pagesAn Overview of Encapsulation Technologies For Food ApplicationsannisyaNo ratings yet
- BioPsych NotesDocument18 pagesBioPsych NotesGUTIERREZ, CRISHA ANDREA M.No ratings yet
- Pathophysiology: Predisposing Factors Precipitating FactorsDocument1 pagePathophysiology: Predisposing Factors Precipitating Factorsrozj07No ratings yet
- 18 May tz2Document14 pages18 May tz2Eunice LeeNo ratings yet
- PELVIS, Student FileDocument52 pagesPELVIS, Student FileShawn Gaurav JhaNo ratings yet
- Cell Communication Ap Study GuideDocument5 pagesCell Communication Ap Study GuideJulia HartwegerNo ratings yet
- Respiratory System PhysiologyDocument35 pagesRespiratory System PhysiologySherwan R Shal100% (2)
- Biology Notes CHPTR 5Document4 pagesBiology Notes CHPTR 5Wan HasliraNo ratings yet
- Central Dogma of Molecular BiologyDocument54 pagesCentral Dogma of Molecular BiologyQuintero MerylNo ratings yet
- PathologyDocument184 pagesPathologymaximazarov100% (1)
- Geriatric Nursing Lecture 2020Document163 pagesGeriatric Nursing Lecture 2020Edgar RebuyasNo ratings yet
- Dr. Gyan P. SinghDocument4 pagesDr. Gyan P. SinghMohammed AL-TuhamiNo ratings yet
- 15-Sensory OrgansDocument23 pages15-Sensory OrgansMilad HabibiNo ratings yet
- PembahasanDocument32 pagesPembahasanwening gbNo ratings yet
- MindfulRunningReport FreeDocument35 pagesMindfulRunningReport Freedavid.paynter24No ratings yet
- BASIC FUNCTIONS of SYNAPSESDocument8 pagesBASIC FUNCTIONS of SYNAPSESJadys Merill DiezNo ratings yet
- Scoring Instructions For The Pittsburgh Sleep Quality IndexDocument1 pageScoring Instructions For The Pittsburgh Sleep Quality IndexMuhammad Afiif AzizNo ratings yet
- Book - Gruper of The WorldDocument11 pagesBook - Gruper of The WorldLidiya KirilovaNo ratings yet
- Practical HAP AttendanceDocument6 pagesPractical HAP AttendanceDAMBALENo ratings yet
- Ayurvedic Approach For Management of Liver Parenchymal Disease Acase Study 2161 069X 1000554Document3 pagesAyurvedic Approach For Management of Liver Parenchymal Disease Acase Study 2161 069X 1000554aman tiwariNo ratings yet
- Endo NclexDocument17 pagesEndo Nclexal-obinay shereenNo ratings yet



























































































Download as ppt, pdf, or txt
You might also like
- 4 Peritoneum PDFDocument64 pages4 Peritoneum PDFN ANo ratings yet
- Peritoneum and Peritoneal CavityDocument26 pagesPeritoneum and Peritoneal CavitytuhinsinghNo ratings yet
- Hyperthermia (Thurs)Document1 pageHyperthermia (Thurs)Christine Esguerra OrozcoNo ratings yet
- Pathophysiology of Intestinal ObstructionDocument3 pagesPathophysiology of Intestinal ObstructionJOvie Rectin100% (2)
- Small IntestineDocument34 pagesSmall IntestineIAMSANWAR019170100% (1)
- Anatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineDocument34 pagesAnatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineBilal YimamNo ratings yet
- Abdomen - Esophagus To ColonDocument42 pagesAbdomen - Esophagus To ColonBibek GajmerNo ratings yet
- Ana SGD 15Document67 pagesAna SGD 15Bea ManzanoNo ratings yet
- Abdominal AnatomyDocument39 pagesAbdominal AnatomyRahul MandhanNo ratings yet
- 1 Abdominal VisceraDocument45 pages1 Abdominal VisceraMero HamedNo ratings yet
- Abdominal CavityDocument78 pagesAbdominal Cavitytanishapatel1005No ratings yet
- Small Intestine MMCDocument65 pagesSmall Intestine MMCWorku KifleNo ratings yet
- Abdomen Part IDocument110 pagesAbdomen Part IAbel GirmaNo ratings yet
- Anatomy of StomachDocument58 pagesAnatomy of StomachSkinny tuberNo ratings yet
- Anatomy of PeritoneumDocument61 pagesAnatomy of PeritoneumFirdaus SeptiawanNo ratings yet
- Stomach: DR Kavitha M Kjiar (Savli)Document52 pagesStomach: DR Kavitha M Kjiar (Savli)Dhaval Chauhan0% (1)
- LO1 Anatomy and Histology of Lower Gi TractDocument180 pagesLO1 Anatomy and Histology of Lower Gi TractIcarus WingsNo ratings yet
- Peritoneum 2022Document86 pagesPeritoneum 2022Tayyib KhanNo ratings yet
- 3 Stomach & Small Intestine Oct 2017Document50 pages3 Stomach & Small Intestine Oct 2017mayankNo ratings yet
- Abdomen.: Moore, Keith. Clinically Oriented Anatomy. Seventh Edition. Lippincott Williams & Wilkins. Baltimore. 2014Document58 pagesAbdomen.: Moore, Keith. Clinically Oriented Anatomy. Seventh Edition. Lippincott Williams & Wilkins. Baltimore. 2014Paola Solarte ChicaizaNo ratings yet
- The StomachDocument3 pagesThe StomachSanjay KishoreNo ratings yet
- Peritoneum: General FeaturesDocument92 pagesPeritoneum: General FeaturestuhinsinghNo ratings yet
- Duodenum and PancreaslectureDocument35 pagesDuodenum and PancreaslectureChigozie GeraldNo ratings yet
- Large IntestineDocument29 pagesLarge IntestineOlaifa victorNo ratings yet
- StomachDocument29 pagesStomachSupriti Verma Bhatnagar100% (1)
- AbdomenDocument142 pagesAbdomenleul TizazuNo ratings yet
- Anatomi Gaster Dan DuodenumDocument179 pagesAnatomi Gaster Dan DuodenumHaraka NabdaNo ratings yet
- GasterDocument179 pagesGasterAraka Patriota100% (1)
- ANAT 221 - PeritoneumDocument22 pagesANAT 221 - PeritoneumWisdom IkechukwuNo ratings yet
- Gross Anatomy of The Small IntestineDocument27 pagesGross Anatomy of The Small IntestineEniola DaramolaNo ratings yet
- Clinical Embriology and Anatomy of Gi Tract Part1Document44 pagesClinical Embriology and Anatomy of Gi Tract Part1trianaamalia100% (1)
- Upper GITDocument33 pagesUpper GITWahida Amalin Ab RazakNo ratings yet
- Colon CancerDocument38 pagesColon CancerUsmle GuyNo ratings yet
- Ac 2Document104 pagesAc 2saide limNo ratings yet
- The Small Intestine-1Document38 pagesThe Small Intestine-1ChiderahNo ratings yet
- Surgical Anatomy of PeritoneumDocument63 pagesSurgical Anatomy of PeritoneumSuvarna RajNo ratings yet
- Anatomy StomachDocument43 pagesAnatomy StomachBijo K BennyNo ratings yet
- Structures of The ForegutDocument13 pagesStructures of The ForegutJatan KothariNo ratings yet
- PeritoneumDocument31 pagesPeritoneumbravadoNo ratings yet
- Colorectal MalignancyDocument108 pagesColorectal MalignancySatishht SatishNo ratings yet
- General Arrangement of The Abdominal VisceraDocument30 pagesGeneral Arrangement of The Abdominal Visceraapi-249972919100% (2)
- STOMACHDocument18 pagesSTOMACHOlaifa victorNo ratings yet
- PeritoneumDocument39 pagesPeritoneumtuhinsinghNo ratings yet
- Anatomy and Histology Gaster - DuodenumDocument149 pagesAnatomy and Histology Gaster - DuodenumRevila AuliaNo ratings yet
- Small IntestineDocument16 pagesSmall IntestineShimmering MoonNo ratings yet
- 4 The Stomach and The Abdominal EsophagusDocument43 pages4 The Stomach and The Abdominal EsophagusAbdullah HaroonNo ratings yet
- Clinical Embriology and Anatomy of Gi Tract Part1Document43 pagesClinical Embriology and Anatomy of Gi Tract Part1Luna LitamiNo ratings yet
- Digestive System (2015 - 06 - 09 20 - 43 - 48 Utc)Document90 pagesDigestive System (2015 - 06 - 09 20 - 43 - 48 Utc)DiazNo ratings yet
- Anat 221-Large IntestineDocument21 pagesAnat 221-Large IntestineWisdom IkechukwuNo ratings yet
- Anatomy of Small Intestine: Lecture-4Document23 pagesAnatomy of Small Intestine: Lecture-4Ahmed OudahNo ratings yet
- Anatomy of Digestive SystemDocument20 pagesAnatomy of Digestive Systemolive jollyNo ratings yet
- Anatomi Dan Histologi Saluran Cerna BawahDocument20 pagesAnatomi Dan Histologi Saluran Cerna BawahIlhamDevirxaNo ratings yet
- Blok GastrointestinalDocument103 pagesBlok GastrointestinalArLyne MakinNo ratings yet
- StomachDocument24 pagesStomachHarini KarthikeyanNo ratings yet
- GIS1 - K1,2 - Anatomi Dan EmbriologiDocument70 pagesGIS1 - K1,2 - Anatomi Dan EmbriologiNatasya Ryani PurbaNo ratings yet
- Digestive SystemDocument242 pagesDigestive SystemVansh SinghNo ratings yet
- Abdomen Kub Presentation (Autosaved)Document81 pagesAbdomen Kub Presentation (Autosaved)adhikariaashi2004No ratings yet
- Anatomy SpleenDocument32 pagesAnatomy SpleenBijo K BennyNo ratings yet
- Small Intestine 2017Document78 pagesSmall Intestine 2017yasrul izadNo ratings yet
- Rectum & Anal CanalDocument14 pagesRectum & Anal CanalLisa DentonNo ratings yet
- Anatomy of Jejunum, Ileum and Large Intestine: Dr. Mohammed Mahmoud MosaedDocument38 pagesAnatomy of Jejunum, Ileum and Large Intestine: Dr. Mohammed Mahmoud MosaedRakaNo ratings yet
- Intestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandIntestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Abdomen: DR Solomie Ayalew, M.D. Wolkite UniversityDocument177 pagesAbdomen: DR Solomie Ayalew, M.D. Wolkite UniversityDureti DuretiNo ratings yet
- Abdomen Wall-1Document86 pagesAbdomen Wall-1Dureti DuretiNo ratings yet
- Lec 6 Thorax - FinalDocument223 pagesLec 6 Thorax - FinalDureti DuretiNo ratings yet
- The Thorax-1 (Compatibility Mode)Document122 pagesThe Thorax-1 (Compatibility Mode)Dureti DuretiNo ratings yet
- Ocular Changes and Approaches of Ophthalmopathy in Basedow - Graves-Parry - Flajani DiseaseDocument7 pagesOcular Changes and Approaches of Ophthalmopathy in Basedow - Graves-Parry - Flajani Diseasesmartjohnsmith10No ratings yet
- 1st M&M 2013 Case Protocol - Shoulder Dystocia PDFDocument4 pages1st M&M 2013 Case Protocol - Shoulder Dystocia PDFAnonymous D7NzSe69kgNo ratings yet
- Female Reproductive OrgansDocument32 pagesFemale Reproductive Organsapi-19916399100% (1)
- Lisa Pang: Education TeachingDocument2 pagesLisa Pang: Education TeachingpangdaNo ratings yet
- Case Taking Form - Bashir Mahmud ElliasDocument5 pagesCase Taking Form - Bashir Mahmud ElliasBashir Mahmud ElliasNo ratings yet
- Vomiting in Children 2018 PDFDocument19 pagesVomiting in Children 2018 PDFSamuel DiazNo ratings yet
- AnatomyDocument4 pagesAnatomySureen PaduaNo ratings yet
- An Overview of Encapsulation Technologies For Food ApplicationsDocument11 pagesAn Overview of Encapsulation Technologies For Food ApplicationsannisyaNo ratings yet
- BioPsych NotesDocument18 pagesBioPsych NotesGUTIERREZ, CRISHA ANDREA M.No ratings yet
- Pathophysiology: Predisposing Factors Precipitating FactorsDocument1 pagePathophysiology: Predisposing Factors Precipitating Factorsrozj07No ratings yet
- 18 May tz2Document14 pages18 May tz2Eunice LeeNo ratings yet
- PELVIS, Student FileDocument52 pagesPELVIS, Student FileShawn Gaurav JhaNo ratings yet
- Cell Communication Ap Study GuideDocument5 pagesCell Communication Ap Study GuideJulia HartwegerNo ratings yet
- Respiratory System PhysiologyDocument35 pagesRespiratory System PhysiologySherwan R Shal100% (2)
- Biology Notes CHPTR 5Document4 pagesBiology Notes CHPTR 5Wan HasliraNo ratings yet
- Central Dogma of Molecular BiologyDocument54 pagesCentral Dogma of Molecular BiologyQuintero MerylNo ratings yet
- PathologyDocument184 pagesPathologymaximazarov100% (1)
- Geriatric Nursing Lecture 2020Document163 pagesGeriatric Nursing Lecture 2020Edgar RebuyasNo ratings yet
- Dr. Gyan P. SinghDocument4 pagesDr. Gyan P. SinghMohammed AL-TuhamiNo ratings yet
- 15-Sensory OrgansDocument23 pages15-Sensory OrgansMilad HabibiNo ratings yet
- PembahasanDocument32 pagesPembahasanwening gbNo ratings yet
- MindfulRunningReport FreeDocument35 pagesMindfulRunningReport Freedavid.paynter24No ratings yet
- BASIC FUNCTIONS of SYNAPSESDocument8 pagesBASIC FUNCTIONS of SYNAPSESJadys Merill DiezNo ratings yet
- Scoring Instructions For The Pittsburgh Sleep Quality IndexDocument1 pageScoring Instructions For The Pittsburgh Sleep Quality IndexMuhammad Afiif AzizNo ratings yet
- Book - Gruper of The WorldDocument11 pagesBook - Gruper of The WorldLidiya KirilovaNo ratings yet
- Practical HAP AttendanceDocument6 pagesPractical HAP AttendanceDAMBALENo ratings yet
- Ayurvedic Approach For Management of Liver Parenchymal Disease Acase Study 2161 069X 1000554Document3 pagesAyurvedic Approach For Management of Liver Parenchymal Disease Acase Study 2161 069X 1000554aman tiwariNo ratings yet
- Endo NclexDocument17 pagesEndo Nclexal-obinay shereenNo ratings yet