Download as pptx, pdf, or txt
You might also like
- D300 Wild Magic Table PDFDocument10 pagesD300 Wild Magic Table PDFGala Alonso Puente67% (3)
- Nursing Care Plans Pelvic Inflammatory DiseaseDocument2 pagesNursing Care Plans Pelvic Inflammatory DiseaseJasmin Jacob74% (35)
- EASY Care StandardDocument16 pagesEASY Care StandardTPSaraHNo ratings yet
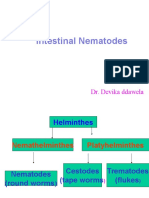
- 6 Intestinal NematodesDocument13 pages6 Intestinal Nematodesبلسم محمود شاكرNo ratings yet
- Revision: Types of Life Cycle in Trematoda and CestodaDocument71 pagesRevision: Types of Life Cycle in Trematoda and CestodaMicroscopeGeekNo ratings yet
- Granulosus and E. Multilocularis (Hydatid) .: Tenia Solium or T. Saginata (Teniasis)Document7 pagesGranulosus and E. Multilocularis (Hydatid) .: Tenia Solium or T. Saginata (Teniasis)moosNo ratings yet
- Parasite Project BIOLOGY EditedDocument21 pagesParasite Project BIOLOGY EditedPadma CharanNo ratings yet
- TrichurisDocument34 pagesTrichurisayaamrsharfNo ratings yet
- Medical Biology 6Document58 pagesMedical Biology 6Yusuf Yağız TimurNo ratings yet
- Kuliah 17 - Nematoda Dan ProtozoaDocument72 pagesKuliah 17 - Nematoda Dan ProtozoaivaNo ratings yet
- Pin WormDocument6 pagesPin WormAbang SupriantoNo ratings yet
- AscariasisDocument44 pagesAscariasisMuhammad AuliaNo ratings yet
- Enterobius VermicularisDocument3 pagesEnterobius Vermicularisshahidkhan 654321654321100% (1)
- Tissue and Blood NematodesDocument53 pagesTissue and Blood NematodesVincent ManganaanNo ratings yet
- Parasitology PresentationDocument28 pagesParasitology PresentationSamuel WilliamsNo ratings yet
- 12 - NematodaDocument44 pages12 - NematodaAnnisya MaharaniNo ratings yet
- NematodesDocument9 pagesNematodesMomo ShinNo ratings yet
- Nematodes Infections of The IntestineDocument17 pagesNematodes Infections of The Intestineabcde990075No ratings yet
- AscarisDocument42 pagesAscarisمصطفي خندقاوي100% (1)
- Hymenolepis Nana Group 5 Write UpDocument7 pagesHymenolepis Nana Group 5 Write UpSusan GachukiaNo ratings yet
- 28 Sept 16 Kuliah HelminthiasisDocument63 pages28 Sept 16 Kuliah HelminthiasisRafif AmirNo ratings yet
- Enterobius Vermicularis) : Hawri H. Mohammed H.D., M.Sc. ParasitologyDocument9 pagesEnterobius Vermicularis) : Hawri H. Mohammed H.D., M.Sc. ParasitologyHawre Najmaddin100% (1)
- Selma CestodesDocument23 pagesSelma CestodesAhmed EisaNo ratings yet
- Project IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Document38 pagesProject IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Catherine MetraNo ratings yet
- المحاضرة 7 مادة الطفيلياتDocument5 pagesالمحاضرة 7 مادة الطفيلياتdyabw6430No ratings yet
- Project IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Document36 pagesProject IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Catherine MetraNo ratings yet
- N M To Es: Dr. Wafaa Ezz ElarabDocument31 pagesN M To Es: Dr. Wafaa Ezz Elarabshoroq zaki100% (1)
- Anclynostoma Duodenale Ancylostoma Duodenale Ancylostoma Ancylostoma Duodenale Necator Americanus Ancylostoma DuodenaleDocument3 pagesAnclynostoma Duodenale Ancylostoma Duodenale Ancylostoma Ancylostoma Duodenale Necator Americanus Ancylostoma DuodenaleMarwin OditaNo ratings yet
- The Flight of The Lonely WandererDocument30 pagesThe Flight of The Lonely Wandererapi-3743483No ratings yet
- INTESTINAL NEMATODES Hand Out 10 - 11Document6 pagesINTESTINAL NEMATODES Hand Out 10 - 11microperadeniyaNo ratings yet
- Other AphasmidsDocument4 pagesOther AphasmidsJayricDepalobosNo ratings yet
- Lecture 6 2023Document16 pagesLecture 6 2023ayaessam392002No ratings yet
- Parasitic Infection in GI TractDocument123 pagesParasitic Infection in GI TractUtami HandayaniNo ratings yet
- Case Study: MicrobiologyDocument13 pagesCase Study: MicrobiologywellYONGNo ratings yet
- Hymenolepis NanaDocument15 pagesHymenolepis NanaDorothyNo ratings yet
- Intestinal NematodesDocument88 pagesIntestinal NematodesVincent Manganaan100% (1)
- Lec 9 NematodesDocument11 pagesLec 9 NematodesMurtdha ArifNo ratings yet
- NematodaDocument96 pagesNematodaPurplesmilezNo ratings yet
- Phylum NematodaDocument24 pagesPhylum NematodaKaten KyoukotsuNo ratings yet
- Platyhelminthes: Hazel Anne L. Tabo Olgga A. HaraDocument79 pagesPlatyhelminthes: Hazel Anne L. Tabo Olgga A. HaraHara OgheeNo ratings yet
- 01 - Parasitic Infections 2020Document85 pages01 - Parasitic Infections 2020gilbert agudoNo ratings yet
- Echinococcosis: Echinococcus GranulosusDocument3 pagesEchinococcosis: Echinococcus GranulosusJohanna FreddaNo ratings yet
- Taenia SoliumDocument7 pagesTaenia Soliumn41995639No ratings yet
- Ancy Lost OmaDocument41 pagesAncy Lost OmaMuhmmad TahaNo ratings yet
- EnterobiusDocument11 pagesEnterobiusMayuri VohraNo ratings yet
- Spirometra, Hymenolepis NanaDocument5 pagesSpirometra, Hymenolepis NanaJayricDepalobosNo ratings yet
- Aljas&Bama (Microbm9evaluate)Document8 pagesAljas&Bama (Microbm9evaluate)Mary Clare Fuentes BamaNo ratings yet
- Canfamphys00240 0140Document4 pagesCanfamphys00240 0140Abbas KhanNo ratings yet
- Exercise 5 ParasitologyDocument3 pagesExercise 5 ParasitologyIvanNo ratings yet
- The Intestinal NematodesDocument107 pagesThe Intestinal Nematodesblue_blooded23100% (1)
- Nematodes: Prepared By: Charriz A. AmoyanDocument81 pagesNematodes: Prepared By: Charriz A. AmoyanAudrie Allyson GabalesNo ratings yet
- Kuliah Cacing WestyDocument63 pagesKuliah Cacing WestyIndra ToshiwayNo ratings yet
- Ovariancystsintheguineapig (Caviaporcellus) : Andrew D. BeanDocument20 pagesOvariancystsintheguineapig (Caviaporcellus) : Andrew D. BeanALEX MOREANO ACOSTUPANo ratings yet
- Fascioliasis, TrematodesDocument31 pagesFascioliasis, Trematodesحسین جاسم ستارNo ratings yet
- Nematode Infections 2019 Student PDFDocument272 pagesNematode Infections 2019 Student PDFCharlene SuliganNo ratings yet
- Intestinal Nematodes: Dr. Devika DdawelaDocument127 pagesIntestinal Nematodes: Dr. Devika DdawelaPraveenKumarNo ratings yet
- CestodesDocument39 pagesCestodesNachiket Vijay PotdarNo ratings yet
- Cyclophyllidean CestodesDocument92 pagesCyclophyllidean CestodesPauline AñesNo ratings yet
- Economic Importance of CoralsDocument3 pagesEconomic Importance of CoralsjaleelkabdulNo ratings yet
- The NemathelminthesDocument16 pagesThe NemathelminthesBudi AfriyansyahNo ratings yet
- Helminths: NematodesDocument17 pagesHelminths: NematodesNicolle PanchoNo ratings yet
- 07-Vaccination Traveller RSUI 2020Document35 pages07-Vaccination Traveller RSUI 2020Eirna Syam Fitri IINo ratings yet
- The Child & Adolescent Learning Quiz 1 AM3Document4 pagesThe Child & Adolescent Learning Quiz 1 AM3Eugen TerseNo ratings yet
- Test Bank For Egans Fundamentals of Respiratory Care 10th Edition KacmarekDocument36 pagesTest Bank For Egans Fundamentals of Respiratory Care 10th Edition Kacmareknuggetessayistypcu100% (50)
- Crocq, Marc-Antoine (2013) - Milestones in The History of Personality Disorders. Dialogues in Clinical Neuroscience, 15 (2), 147-153Document7 pagesCrocq, Marc-Antoine (2013) - Milestones in The History of Personality Disorders. Dialogues in Clinical Neuroscience, 15 (2), 147-153AcatalepsoNo ratings yet
- Colorectal Carcinoma SurgeryDocument19 pagesColorectal Carcinoma SurgeryDaanishNo ratings yet
- Research Article: Detecting Abnormal Brain Regions in Schizophrenia Using Structural MRI Via Machine LearningDocument13 pagesResearch Article: Detecting Abnormal Brain Regions in Schizophrenia Using Structural MRI Via Machine LearningHago GoraNo ratings yet
- Infants of Women With Diabetes - UpToDateDocument16 pagesInfants of Women With Diabetes - UpToDatethelesphol pascalNo ratings yet
- A.G Carsico Et Al 2019Document7 pagesA.G Carsico Et Al 2019reclinpharmaNo ratings yet
- Midterm-Understanding The SelfDocument2 pagesMidterm-Understanding The SelfJuliet Cajes LicongNo ratings yet
- Prioritization LectureDocument6 pagesPrioritization LecturesamNo ratings yet
- Youth Leadership Participation and Accountability - The Recommendations 1Document28 pagesYouth Leadership Participation and Accountability - The Recommendations 1Aldren HilaNo ratings yet
- Jurnal Ilmiah Biologi UMA (JIBIOMA) : Penentuan Kadar Glukosa Urine Di Laboratorium Rumah Sakit Sari Mutiara MedanDocument5 pagesJurnal Ilmiah Biologi UMA (JIBIOMA) : Penentuan Kadar Glukosa Urine Di Laboratorium Rumah Sakit Sari Mutiara MedanIndraNo ratings yet
- Estethic DentistreDocument639 pagesEstethic DentistreAdrian Venegas Melo100% (1)
- NCP Risk For Bleeding 3Document2 pagesNCP Risk For Bleeding 3Jayson Olile100% (2)
- N-Methyl Aniline MSDS 99Document5 pagesN-Methyl Aniline MSDS 99Labeed ShamilNo ratings yet
- LIST OF DOCUMENTS To Be Submitted To The Notified Body (NB) PCBC For Conformity Assessment of The Medical DeviceDocument5 pagesLIST OF DOCUMENTS To Be Submitted To The Notified Body (NB) PCBC For Conformity Assessment of The Medical DevicegobeliyNo ratings yet
- Hallucinations in The General Population PDFDocument11 pagesHallucinations in The General Population PDFsasaNo ratings yet
- Sugar BluesDocument16 pagesSugar Bluesrobert desai100% (3)
- Medicinal Uses of TecomaDocument18 pagesMedicinal Uses of TecomaSimratNo ratings yet
- Bwahkinang InaDocument2 pagesBwahkinang InaChristine TamayoNo ratings yet
- Introduction To The Endocrine System: Human PhysiologyDocument27 pagesIntroduction To The Endocrine System: Human PhysiologySamNo ratings yet
- BronchosDocument5 pagesBronchosNeicoNo ratings yet
- Parasitology Review Notes For Medical Technologists: Leishmania SPP)Document39 pagesParasitology Review Notes For Medical Technologists: Leishmania SPP)Kat Jornadal100% (2)
- Reproductive HealthDocument93 pagesReproductive HealthDr shwetha hitnalNo ratings yet
- Icsst Nfpa-1001 Ff.i Reviewer - MarkedDocument40 pagesIcsst Nfpa-1001 Ff.i Reviewer - MarkedTinashe chikwanhaNo ratings yet
- Awareness SurveyDocument6 pagesAwareness Surveyveerasankar123No ratings yet
- Reproductive Health Class 12 Biology Mcqs PDF: Object 1Document41 pagesReproductive Health Class 12 Biology Mcqs PDF: Object 1rigNo ratings yet