Download as pptx, pdf, or txt
You might also like
- Sports Medicine Exam2020 QQ - 1Document22 pagesSports Medicine Exam2020 QQ - 1Volc100% (2)
- Upper Limb OrthosisDocument53 pagesUpper Limb OrthosisifrahjavedNo ratings yet
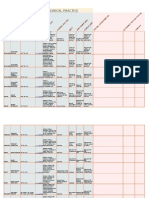
- Goniometry For Clinical PracticeDocument7 pagesGoniometry For Clinical Practicedramitsaini33% (3)
- Netter Atlas UL ChartsDocument4 pagesNetter Atlas UL ChartsJUSASB100% (1)
- Upper Extremity OrthoticsDocument19 pagesUpper Extremity OrthoticsCatalina CuleaNo ratings yet
- 07 Upper Limbs Orthosis Lecture 7Document11 pages07 Upper Limbs Orthosis Lecture 7Ijaz KhanNo ratings yet
- ORTHOSES FOR BURN MANAGMENT by DR Laiba HashmiDocument27 pagesORTHOSES FOR BURN MANAGMENT by DR Laiba Hashmihashmilaiba847No ratings yet
- Inroduction To AmputationDocument67 pagesInroduction To AmputationAlfred JacksonNo ratings yet
- DISCUSS THE USE OF SPLINTS AND TRACTION IN OrthopaedicDocument51 pagesDISCUSS THE USE OF SPLINTS AND TRACTION IN OrthopaedicEmmanuel DanielsNo ratings yet
- AmputationDocument52 pagesAmputationShobhit SharmaNo ratings yet
- Fracture ManagementDocument186 pagesFracture ManagementAyi SuwarayiNo ratings yet
- Splinting, Orthoses, and Casting For Occupational Therapy StudentsDocument43 pagesSplinting, Orthoses, and Casting For Occupational Therapy StudentsNatalia RamirezNo ratings yet
- Acquired Deformities1 PDFDocument33 pagesAcquired Deformities1 PDFRishabh VermaNo ratings yet
- Orthopaedics and Orthopaedic Nursing RNDocument70 pagesOrthopaedics and Orthopaedic Nursing RNFaith LwabilaNo ratings yet
- Splints+Tra: Guided By: Dr. PRAKASH D.RDocument111 pagesSplints+Tra: Guided By: Dr. PRAKASH D.Rlailatul husnaNo ratings yet
- Upper Limb OrthosesDocument29 pagesUpper Limb OrthosesMaryam KhalidNo ratings yet
- Amputation and ProsthesisDocument5 pagesAmputation and Prosthesisaishp2897No ratings yet
- 18 ProstheticsDocument54 pages18 ProstheticsMariya DantisNo ratings yet
- Rehabilitation of Adults With Upper-Limb AmputationsDocument59 pagesRehabilitation of Adults With Upper-Limb AmputationsSameeha AbbassNo ratings yet
- Orthopedic Injuries and Immobilization: Stanford University Division of Emergency MedicineDocument36 pagesOrthopedic Injuries and Immobilization: Stanford University Division of Emergency MedicineMohammad NorzaimNo ratings yet
- Orthosis and ProsthesisDocument25 pagesOrthosis and Prosthesissanika pradhanNo ratings yet
- Rigid Hinge: 1) Single-Axis Hinges.Document8 pagesRigid Hinge: 1) Single-Axis Hinges.Naziya KhanNo ratings yet
- 12.rehabilitation EngineeringDocument19 pages12.rehabilitation EngineeringMuhammad Moazzam100% (1)
- AmputationDocument16 pagesAmputationElmeldah TwaraNo ratings yet
- Splints and Tractions in OrthopaedicsDocument56 pagesSplints and Tractions in OrthopaedicsNinaNo ratings yet
- Orthosisofhandppt 181202162551Document65 pagesOrthosisofhandppt 181202162551Khageswar SamalNo ratings yet
- Appareillage de Traction Et de Contention Des Membres - Fr.enDocument61 pagesAppareillage de Traction Et de Contention Des Membres - Fr.enchaib boudabNo ratings yet
- Kinesio TapingDocument62 pagesKinesio TapingDiah Rahmat100% (1)
- Upper Limb OrthosisDocument83 pagesUpper Limb OrthosisAwaisNo ratings yet
- Prosthesis: Uganeswary VenugopalDocument14 pagesProsthesis: Uganeswary VenugopalUganeswary VenugopalNo ratings yet
- Taping and Wrapping: Sports MedicineDocument34 pagesTaping and Wrapping: Sports Medicinewong yoke hinNo ratings yet
- Immobilization ExtricationDocument75 pagesImmobilization ExtricationJohn Britto100% (3)
- Forearm SplintingDocument6 pagesForearm SplintingArabelle GONo ratings yet
- Functions of The Knee JointDocument40 pagesFunctions of The Knee JointAlfred JacksonNo ratings yet
- VRP STRDocument13 pagesVRP STRInna Ysabelle Hipolito CarpioNo ratings yet
- Splinting Techniques: by Madhumitha M, Aruna G, Abi P, Sakthivelayudham G, Sujidha R, Srivignesh MDocument99 pagesSplinting Techniques: by Madhumitha M, Aruna G, Abi P, Sakthivelayudham G, Sujidha R, Srivignesh MSakthivelayudhamganesanNo ratings yet
- Hemipelvectomy and Hip DisarticulationDocument40 pagesHemipelvectomy and Hip DisarticulationCarmelle Zia ReyesNo ratings yet
- Lower Limb Orthosis: DR - Ayesha Bhatti PP - DPT, BSPTDocument43 pagesLower Limb Orthosis: DR - Ayesha Bhatti PP - DPT, BSPTMajgsjqNo ratings yet
- Total Elbow Arthroplasty and RehabilitationDocument5 pagesTotal Elbow Arthroplasty and RehabilitationMarina ENo ratings yet
- Contentions Et Tractions TF - Fr.enDocument48 pagesContentions Et Tractions TF - Fr.enchaib boudabNo ratings yet
- Unit 4 ProsthesisDocument61 pagesUnit 4 ProsthesisMythily VedhagiriNo ratings yet
- (Trauma) 18 September Lower Extremity AmputationDocument37 pages(Trauma) 18 September Lower Extremity Amputationpublic newbieNo ratings yet
- SPLINTSDocument42 pagesSPLINTSRachit SekhrajkaNo ratings yet
- Modul PlusDocument64 pagesModul PlusMuhamad BenyaminNo ratings yet
- Definition & General Principle of ProsthesisDocument40 pagesDefinition & General Principle of ProsthesisAkbar AziziNo ratings yet
- Rotator Cuff Tear: Basic Understanding and Treatment OptionsDocument26 pagesRotator Cuff Tear: Basic Understanding and Treatment OptionsirsankurniawanNo ratings yet
- Cast/Splint Choice and Application: Worku K. (MD)Document15 pagesCast/Splint Choice and Application: Worku K. (MD)Worku KifleNo ratings yet
- A Double Reverse Kleinert Extension Splint For Extensor Tendon Repairs in Zones VI To VIIIDocument3 pagesA Double Reverse Kleinert Extension Splint For Extensor Tendon Repairs in Zones VI To VIIIElizabeth BrugesNo ratings yet
- Splint and CrutchesDocument37 pagesSplint and CrutchesNadhirah Mohamad NohNo ratings yet
- Orthopedic Devices DDocument31 pagesOrthopedic Devices Dmakenawairimu30No ratings yet
- Orthosis Dan ProsthesisDocument39 pagesOrthosis Dan ProsthesisdimasNo ratings yet
- ArthroplastyDocument64 pagesArthroplastyAmit Kochhar75% (4)
- Amputee RehabDocument153 pagesAmputee RehabNancy GuptaNo ratings yet
- DEFINATION: Amputation Is The Removal of ADocument22 pagesDEFINATION: Amputation Is The Removal of AsurchadNo ratings yet
- ProsthesisDocument14 pagesProsthesisUganeswary Venugopal100% (1)
- Facture/Dislocation: R I C EDocument23 pagesFacture/Dislocation: R I C EKrishnamurti KambleNo ratings yet
- RRASSINGMENTDocument12 pagesRRASSINGMENTAditi RajoraNo ratings yet
- Malleolar Fractures - Handout PDFDocument14 pagesMalleolar Fractures - Handout PDFAlin Bratu100% (2)
- Slide OrtopedieDocument134 pagesSlide OrtopedieIoana IsarieNo ratings yet
- Upper Extremity CastingDocument23 pagesUpper Extremity Castingamal.fathullahNo ratings yet
- Distal Humerus Fracture: Presentor:Dr Balaji Vinayaka Mission Kirubananda Variyar Medical College. SalemDocument48 pagesDistal Humerus Fracture: Presentor:Dr Balaji Vinayaka Mission Kirubananda Variyar Medical College. SalemNicholas DelaliNo ratings yet
- Reduction, Relocation and Splinting in Emergency Room (RASER)From EverandReduction, Relocation and Splinting in Emergency Room (RASER)No ratings yet
- Donatelli Chapter 2 Shoulder 2018Document16 pagesDonatelli Chapter 2 Shoulder 2018Julia SalvioNo ratings yet
- Anterior Compartment of Arm & Cubital FossaDocument24 pagesAnterior Compartment of Arm & Cubital FossaShahid MaqboolNo ratings yet
- Hand Flexor Tendon InjuryDocument13 pagesHand Flexor Tendon InjuryAsogaa MeteranNo ratings yet
- Brachialplexus Wustl Edu Glossary HTML 76Document7 pagesBrachialplexus Wustl Edu Glossary HTML 76Misa AjversonNo ratings yet
- Fracture Treatment - Quick Reference PosterDocument1 pageFracture Treatment - Quick Reference PosterTingting GeNo ratings yet
- Elbow Special TestDocument4 pagesElbow Special TestEllaiza Astacaan100% (1)
- The Spine and Shoulder Joints - Motion in The Golf SwingDocument14 pagesThe Spine and Shoulder Joints - Motion in The Golf SwingDFJohnsoNo ratings yet
- PDF Essentials of Musculoskeletal Care Fifth Edition American Academy of Orthopaedic Surgeons Ebook Full ChapterDocument53 pagesPDF Essentials of Musculoskeletal Care Fifth Edition American Academy of Orthopaedic Surgeons Ebook Full Chapterdaniel.keller545100% (3)
- Brachial Plexus MnemonicsDocument6 pagesBrachial Plexus MnemonicsTima Rawnap.No ratings yet
- 6 Eurofit Fitness BatteryDocument8 pages6 Eurofit Fitness BatteryRalucaAlupoaieNo ratings yet
- Pembekalan BPI Sem 5Document40 pagesPembekalan BPI Sem 5Mukhtar Ali MuktiNo ratings yet
- Anatomy Mnemonics UsmleDocument65 pagesAnatomy Mnemonics UsmleHoney HoneyNo ratings yet
- Bates' Guide To Physical Examination and History Taking, 12th EditionDocument41 pagesBates' Guide To Physical Examination and History Taking, 12th EditionTimothy GrecoNo ratings yet
- Ppt2 Pre Games TraditionalDocument46 pagesPpt2 Pre Games TraditionalAlyanna MagkalasNo ratings yet
- Shoulder and ArmDocument2 pagesShoulder and ArmMarina GincuNo ratings yet
- Dariel Fitzkee - Linking Ring Manipulation PDFDocument32 pagesDariel Fitzkee - Linking Ring Manipulation PDFLuigi-igiuL100% (4)
- Special Test For Shoulder:-For ImpingementDocument5 pagesSpecial Test For Shoulder:-For ImpingementYusrah SaniNo ratings yet
- Elbow Radiography: Projection Method Part Position Central Ray Structures Shown AP ProjectionDocument14 pagesElbow Radiography: Projection Method Part Position Central Ray Structures Shown AP ProjectionAndrei YabutNo ratings yet
- Worksheet - Movement AssignmentDocument9 pagesWorksheet - Movement Assignmentapi-240988800No ratings yet
- Body LinesDocument1 pageBody LinesAnonymous OAEuN9NE1sNo ratings yet
- 12 Steps For Proper Hand Washing PosterDocument1 page12 Steps For Proper Hand Washing PosterFizz FirdausNo ratings yet
- Activity Analysis Sample PedrettiDocument4 pagesActivity Analysis Sample PedrettiLenard Yel FernandezNo ratings yet
- Ace PDFDocument684 pagesAce PDFsami xNo ratings yet
- De Quervain's TendinosisDocument30 pagesDe Quervain's TendinosisSze Wing LeeNo ratings yet
- Fractures of The Shaft of The HumerusDocument6 pagesFractures of The Shaft of The HumerusTinkovan IonNo ratings yet
- Sistem Gerak Pada Regio Dan Vertebra WulanDocument16 pagesSistem Gerak Pada Regio Dan Vertebra WulanAlexander Xaverius LakiNo ratings yet
- Dr. Eman El Sawaf: Anatomy & Embryology DepartmentDocument56 pagesDr. Eman El Sawaf: Anatomy & Embryology DepartmentKareem DawoodNo ratings yet