Download as pptx, pdf, or txt
You might also like
- Radar Plotting SheetDocument1 pageRadar Plotting SheetCl dubeyNo ratings yet
- Anatomy, Lecture 12, Blood Supply of The Gastrointestinal Tract (Slides)Document27 pagesAnatomy, Lecture 12, Blood Supply of The Gastrointestinal Tract (Slides)Ali Al-Qudsi100% (1)
- Computer Project 1: Assignment 1.1Document10 pagesComputer Project 1: Assignment 1.1Nelu TurcanuNo ratings yet
- Anatomy of The AortaDocument19 pagesAnatomy of The AortaUma Sanggari ThirunavukarasuNo ratings yet
- Vascularization of AbdomenDocument25 pagesVascularization of AbdomenInka Fransiska MariaNo ratings yet
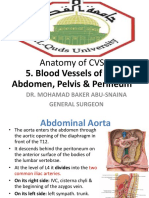
- Anatomy of CVS: 5. Blood Vessels of The Abdomen, Pelvis & PerineumDocument30 pagesAnatomy of CVS: 5. Blood Vessels of The Abdomen, Pelvis & Perineumsultan khabeebNo ratings yet
- Blood Vessels of Abdomen-PIMSR DR - Gosai 2022Document32 pagesBlood Vessels of Abdomen-PIMSR DR - Gosai 2022Dr.B.B.GosaiNo ratings yet
- Arterial SystemDocument49 pagesArterial SystemNaveelaNo ratings yet
- 13b.blood Vessels of AbdomenDocument71 pages13b.blood Vessels of AbdomenIshimwe TheotimeNo ratings yet
- Blood Supply To The AbdomenDocument29 pagesBlood Supply To The AbdomentawandarukwavamadisonNo ratings yet
- Blood Supply of The Gastrointestinal TractDocument2 pagesBlood Supply of The Gastrointestinal TractAli AkeelNo ratings yet
- Large Blood Vessels of The GutDocument61 pagesLarge Blood Vessels of The GutpoojaNo ratings yet
- 3 Major Arteries of GIDocument9 pages3 Major Arteries of GIbeia21No ratings yet
- Emrcs SurgeryDocument145 pagesEmrcs Surgerydanish balochNo ratings yet
- Coeliac Trunk Dr. A. S. D' SouzaDocument12 pagesCoeliac Trunk Dr. A. S. D' SouzaLisa DentonNo ratings yet
- Blood Circulation-DmDocument32 pagesBlood Circulation-DmMathews showsNo ratings yet
- AnatomyDocument8 pagesAnatomyOM BAWNENo ratings yet
- Blood Vessels and CirculationDocument45 pagesBlood Vessels and CirculationLloyd RebusiNo ratings yet
- Blood Supply To The GitDocument15 pagesBlood Supply To The GitEniola abdullahi AduagbaNo ratings yet
- Angiology Lecture 2Document5 pagesAngiology Lecture 2আহানাফ তাহমিদ শব্দNo ratings yet
- Pulmonary Trunk Ascending Aorta, Aortic Arch and Its BranchesDocument27 pagesPulmonary Trunk Ascending Aorta, Aortic Arch and Its Branches4dyhm4456qNo ratings yet
- Anatomy of Circulatory SystemDocument56 pagesAnatomy of Circulatory SystemLina Wijaya100% (2)
- Superior & Inferior Mesenteric Arteries Portal Vein & Its TributariesDocument19 pagesSuperior & Inferior Mesenteric Arteries Portal Vein & Its TributariesHevin GokulNo ratings yet
- The Cardiovascular System Blood VesselsDocument50 pagesThe Cardiovascular System Blood Vesselsyamlehtemagallanes888No ratings yet
- Anatomy of HeartDocument34 pagesAnatomy of HeartSamyog ChaliseNo ratings yet
- CardiovascularDocument92 pagesCardiovascularRolinette DaneNo ratings yet
- Cardiac Chambers Valves Cardiac SkeletonDocument30 pagesCardiac Chambers Valves Cardiac Skeleton4dyhm4456qNo ratings yet
- Anatomy 2nd-U-1 CVSDocument121 pagesAnatomy 2nd-U-1 CVSsinte beyuNo ratings yet
- STOMACHDocument18 pagesSTOMACHOlaifa victorNo ratings yet
- MS Wrep IIDocument51 pagesMS Wrep IIiana-almocera-6970No ratings yet
- Aorta AnatomyDocument41 pagesAorta AnatomySingey LhendupNo ratings yet
- Anatomy of Urinary SystemDocument42 pagesAnatomy of Urinary Systemdebdeepbhattacharya411No ratings yet
- Blood Supply of AbdomenDocument30 pagesBlood Supply of AbdomenShadowStormNo ratings yet
- Cardio NewDocument204 pagesCardio NewHaleema SaadiaNo ratings yet
- Osup TTDocument23 pagesOsup TTKIM EUNHANo ratings yet
- Cardiovascular and Circulatory FunctionDocument271 pagesCardiovascular and Circulatory FunctionARAGON GEMMA LYNNo ratings yet
- Cardiovascular System Part 2 PDFDocument46 pagesCardiovascular System Part 2 PDFVizhiNo ratings yet
- Small IntestineDocument16 pagesSmall IntestineShimmering MoonNo ratings yet
- Cardiovascular System Heart ModuleDocument19 pagesCardiovascular System Heart Modulebadodong700No ratings yet
- Cardiovascular System: HeartDocument44 pagesCardiovascular System: HeartMohammedJSkaikNo ratings yet
- Case 2: 1. What Is The Blood Supply of The Alimentary System? EsophagusDocument25 pagesCase 2: 1. What Is The Blood Supply of The Alimentary System? EsophagusMed LawNo ratings yet
- Cardiovascular SystemDocument18 pagesCardiovascular SystemDeep RoyNo ratings yet
- Null 1Document37 pagesNull 1Esdras DountioNo ratings yet
- Heart PDFDocument73 pagesHeart PDFzanelehgazuNo ratings yet
- BloodsupplyofgitDocument29 pagesBloodsupplyofgitAishaFarooqNo ratings yet
- Anatomy of CVS: 2. The HeartDocument68 pagesAnatomy of CVS: 2. The Heartsultan khabeebNo ratings yet
- The AortaDocument52 pagesThe Aortaviorel79No ratings yet
- The Aorta - Branches - Aortic Arch - TeachMeAnatomy PDFDocument5 pagesThe Aorta - Branches - Aortic Arch - TeachMeAnatomy PDFUsama KhawajaNo ratings yet
- Liver, PancreasDocument42 pagesLiver, Pancreasjosephsilva112No ratings yet
- The Portal Venous SystemDocument21 pagesThe Portal Venous SystemAhmed DsoukiNo ratings yet
- Liver and Biliary TractDocument27 pagesLiver and Biliary TractAbraham Oluwatimilehin IsaacNo ratings yet
- The Abdominal AortaDocument9 pagesThe Abdominal AortaJuan Jose LeonNo ratings yet
- Ana 202 Gross Anatomy of The Heart and Great VesselsDocument57 pagesAna 202 Gross Anatomy of The Heart and Great Vesselsayomideolaniran14No ratings yet
- Posterior Abdominal Wall 2Document34 pagesPosterior Abdominal Wall 2kastodaniel4971No ratings yet
- Heart - AnatomyDocument66 pagesHeart - AnatomySony ArthurNo ratings yet
- Samenvatting Anatomie HPDocument11 pagesSamenvatting Anatomie HPndoemdnsNo ratings yet
- Arteries On The Posterior Abdominal Wall.Document19 pagesArteries On The Posterior Abdominal Wall.Shimmering MoonNo ratings yet
- Cardiovascular System: Blood VesselsDocument12 pagesCardiovascular System: Blood VesselsSoniyaJI84100% (1)
- Cardio VasDocument99 pagesCardio VashellerkittyNo ratings yet
- Blood Vessels and CirculationDocument11 pagesBlood Vessels and CirculationMary Ann SacramentoNo ratings yet
- Human Body Book | Introduction to the Vascular System | Children's Anatomy & Physiology EditionFrom EverandHuman Body Book | Introduction to the Vascular System | Children's Anatomy & Physiology EditionNo ratings yet
- Product Requirements Specification Process in ProdDocument12 pagesProduct Requirements Specification Process in ProdemmyNo ratings yet
- Fourth Quarter Exam in TLE Grade SevenDocument5 pagesFourth Quarter Exam in TLE Grade SevenShabby Gay Trogani83% (12)
- Our Own English High School, Sharjah Look Who'S Answering Quiz Club Group I (Grade 1) Question Bank - MAY 2019Document3 pagesOur Own English High School, Sharjah Look Who'S Answering Quiz Club Group I (Grade 1) Question Bank - MAY 2019Abimanyu ShenilNo ratings yet
- Nclex Boot CampDocument24 pagesNclex Boot CampMariekris Sangalang100% (12)
- CPS - Data Intensive Distributed ComputingDocument11 pagesCPS - Data Intensive Distributed ComputingManoj KavediaNo ratings yet
- Aquion Battery Technology - 1216Document18 pagesAquion Battery Technology - 1216sinnlosNo ratings yet
- Travel Tourism in Bangladesh: A Study On Regent Tours & TravelDocument72 pagesTravel Tourism in Bangladesh: A Study On Regent Tours & TravelNahidNo ratings yet
- Ingersoll Rand Ingersoll Rand Compressor 39880984 Interstage Pressure SwitchDocument1 pageIngersoll Rand Ingersoll Rand Compressor 39880984 Interstage Pressure Switchbara putranta fahdliNo ratings yet
- P2 Chp2 Section 2.1ADocument3 pagesP2 Chp2 Section 2.1APaing Khant KyawNo ratings yet
- Environmental EthicsDocument6 pagesEnvironmental EthicsHELI SHAHNo ratings yet
- 2006 Philippines Road ClassificationDocument44 pages2006 Philippines Road ClassificationpetiepanNo ratings yet
- Urinary SystemDocument9 pagesUrinary SystemMary Joyce RamosNo ratings yet
- Valorisation of Spent Coffee Grounds Production of Biodiesel Via Enzimatic Catalisis With Ethanol and Co-SolventDocument14 pagesValorisation of Spent Coffee Grounds Production of Biodiesel Via Enzimatic Catalisis With Ethanol and Co-SolventAline GonçalvesNo ratings yet
- Metasploit FrameworkDocument1 pageMetasploit FrameworkPAUL VINCENT FAJARDONo ratings yet
- CoEpower SVG AHF Price ListDocument2 pagesCoEpower SVG AHF Price ListChristian Huanca OscoNo ratings yet
- Youjo Senki Side Story - A Borrowed Cat (v1.1)Document11 pagesYoujo Senki Side Story - A Borrowed Cat (v1.1)faiyaNo ratings yet
- Geography & Resources of The PhilippinesDocument12 pagesGeography & Resources of The PhilippinesPaulAliboghaNo ratings yet
- End-Of-Year Test: ListeningDocument3 pagesEnd-Of-Year Test: ListeningRox Purdea0% (1)
- Global Stability Analysis of Eccentric Taylor Couette FlowDocument28 pagesGlobal Stability Analysis of Eccentric Taylor Couette FlowSreekanth MenonNo ratings yet
- KKSB1273 Teknologi Binaan Dan Bahan 01 1112 - 09 Konkrit Sebagai Bahan BinaanDocument56 pagesKKSB1273 Teknologi Binaan Dan Bahan 01 1112 - 09 Konkrit Sebagai Bahan BinaanFarhana NorzelanNo ratings yet
- Especificaciones de Motor j15 de Datsun NissanDocument2 pagesEspecificaciones de Motor j15 de Datsun NissanPablo Andres60% (5)
- QnA Intro To Gas Regulation in Indonesia (Ilham Maulana)Document15 pagesQnA Intro To Gas Regulation in Indonesia (Ilham Maulana)Ilham Maulana Ash Shiddieq100% (1)
- Class 9 - ScienceDocument228 pagesClass 9 - ScienceYashwanth KasturiNo ratings yet
- Analisis Potensi Dan Tingkat Pemanfaatan Sumberdaya Ikan Di Perairan Kabupaten Bangka SelatanDocument12 pagesAnalisis Potensi Dan Tingkat Pemanfaatan Sumberdaya Ikan Di Perairan Kabupaten Bangka SelatanShope IkmaNo ratings yet
- Sonia Thakker 184 Jignesh Bhatt 105 Rekha Wachkawde 188 Shailendra Singh 178 Pravin Nayak 147 Jibu James 128Document44 pagesSonia Thakker 184 Jignesh Bhatt 105 Rekha Wachkawde 188 Shailendra Singh 178 Pravin Nayak 147 Jibu James 128treakoNo ratings yet
- Logicalreasoning MockDocument11 pagesLogicalreasoning MockTarun GaurNo ratings yet
- Fliqlo - Mobile AppDocument1 pageFliqlo - Mobile AppJon BaerNo ratings yet
- Raychem Molded PartsDocument28 pagesRaychem Molded PartsAMNo ratings yet