
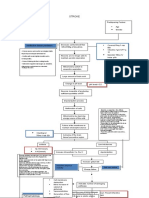
Existing Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical Form
Existing Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical Form
You might also like
- USUHS Anesthesia Pharmacology NotesetDocument247 pagesUSUHS Anesthesia Pharmacology NotesetSean Bancroft100% (3)
- Basic Principles of Obturator Design For Partially Edentulous Patients. Part I: ClassificationDocument69 pagesBasic Principles of Obturator Design For Partially Edentulous Patients. Part I: ClassificationDrFarha NazNo ratings yet
- Anti Diabetic DrugsDocument58 pagesAnti Diabetic DrugsDaniel Wang100% (1)
- Opioids Medicinal ChemistryDocument38 pagesOpioids Medicinal ChemistryDaniel WangNo ratings yet
- Concept Map CVADocument1 pageConcept Map CVASuzette Rae Tate100% (2)
- Pickard's Manual-Tooth Wear (Dragged)Document8 pagesPickard's Manual-Tooth Wear (Dragged)Adit MehtaNo ratings yet
- Flap Surgery 2Document38 pagesFlap Surgery 2Fah100% (1)
- Definition:: Types of Forceps Used For Tooth ExtractionDocument28 pagesDefinition:: Types of Forceps Used For Tooth Extractionayman moaed alyasen100% (1)
- Tarrson Family Endowed Chair in PeriodonticsDocument54 pagesTarrson Family Endowed Chair in PeriodonticsAchyutSinhaNo ratings yet
- New Microsoft Office Word DocumentDocument3 pagesNew Microsoft Office Word DocumentAtulsanapNo ratings yet
- Single Flap Approach With and Without Guided TissueDocument21 pagesSingle Flap Approach With and Without Guided TissuekarthikNo ratings yet
- Techniques On Vertical Ridge Augmentation: Indications and EffectivenessDocument30 pagesTechniques On Vertical Ridge Augmentation: Indications and Effectivenessrmartins76No ratings yet
- MLV136 REV C Locator PresentationDocument58 pagesMLV136 REV C Locator PresentationS. BenzaquenNo ratings yet
- Porcelain Fused To Metal (PFM) Crowns and Caries in Adjacent TeetDocument5 pagesPorcelain Fused To Metal (PFM) Crowns and Caries in Adjacent Teetbaiq rengganis dewiNo ratings yet
- Challenges in Dentin BondingDocument11 pagesChallenges in Dentin BondingDanish SattarNo ratings yet
- ACP Complete EdentulismDocument89 pagesACP Complete EdentulismAshwin PangiNo ratings yet
- Polyetheretherketone PEEK Dental Implants A Case FDocument8 pagesPolyetheretherketone PEEK Dental Implants A Case FPhoebe David100% (1)
- Bedrossian Treatment Planning The Maxilla PDFDocument11 pagesBedrossian Treatment Planning The Maxilla PDFSitiKhadijahNo ratings yet
- Surgical Extrusion: A Dental TechniqueDocument6 pagesSurgical Extrusion: A Dental TechniqueDragos CiongaruNo ratings yet
- Use of Implants in The Pterygoid Region For Prosthodontic TreatmentDocument4 pagesUse of Implants in The Pterygoid Region For Prosthodontic TreatmentSidhartha KumarNo ratings yet
- Preprosthetic and Reconstructive SurgeryDocument32 pagesPreprosthetic and Reconstructive Surgeryruoiconmapu100% (1)
- Short Implants or GraftsDocument31 pagesShort Implants or GraftsJess YuanNo ratings yet
- C24024 - Harmonize Shade Guide - EN UK PDFDocument7 pagesC24024 - Harmonize Shade Guide - EN UK PDFFabio RibeiroNo ratings yet
- The Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFDocument7 pagesThe Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFAhmed Mohammed Saaduddin Sapri100% (1)
- Badly Broken MarzoukDocument68 pagesBadly Broken MarzoukHend MohamedNo ratings yet
- Direct Cuspal CoverageDocument8 pagesDirect Cuspal CoverageLuLu NikhlaturNo ratings yet
- Pulp Therapy For Primary and Immature Permanent TeethDocument11 pagesPulp Therapy For Primary and Immature Permanent TeethPrabhjot KaurNo ratings yet
- What Is Suturing?: - The Primary Objective Is To Position andDocument16 pagesWhat Is Suturing?: - The Primary Objective Is To Position andmehak malhotraNo ratings yet
- Regressive Changes of TeethDocument45 pagesRegressive Changes of TeethNader AlaizariNo ratings yet
- Instrument Used in ExodontaDocument32 pagesInstrument Used in ExodontaNoor Abdullah AlNo ratings yet
- Wisdom Tooth WisdomDocument134 pagesWisdom Tooth WisdomPaulo Rabelo Jr.100% (1)
- Dentin Bonding Agents - An OverviewDocument4 pagesDentin Bonding Agents - An OverviewIOSRjournalNo ratings yet
- Surgical Vs Non-Surgical Approach in PeriodonticsDocument13 pagesSurgical Vs Non-Surgical Approach in PeriodonticsBea DominguezNo ratings yet
- Alloderm Surgical Technique Guide PDFDocument8 pagesAlloderm Surgical Technique Guide PDFamagueNo ratings yet
- Material Options For Class II Composite Restorations - Varied Clinical Parameters Require Different TechniquesDocument6 pagesMaterial Options For Class II Composite Restorations - Varied Clinical Parameters Require Different TechniquesMohammed NabeelNo ratings yet
- Anterior Cross-Bite Conference On 16092010Document42 pagesAnterior Cross-Bite Conference On 16092010Dent YomarajNo ratings yet
- Alveolar Ridge Preservation Utilizing The Socket-Plug TechniqueDocument7 pagesAlveolar Ridge Preservation Utilizing The Socket-Plug Techniquekeily rodriguez100% (1)
- Implants in Esthetic ZoneDocument10 pagesImplants in Esthetic ZoneInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- MANUAL FOR OPERATIVE DENTISTRY - Xa - Yimg.com (PDFDrive)Document169 pagesMANUAL FOR OPERATIVE DENTISTRY - Xa - Yimg.com (PDFDrive)cvpk prasannaNo ratings yet
- Oral Manifestations of Denture AbuseDocument53 pagesOral Manifestations of Denture AbuseBharanija100% (2)
- 3.factors and Techniques Influencing Peri-Implant Papillae - PDFDocument12 pages3.factors and Techniques Influencing Peri-Implant Papillae - PDFMargarita María Blanco LópezNo ratings yet
- Fundamentals of Cavity PreprationDocument70 pagesFundamentals of Cavity PreprationSATNAMNo ratings yet
- Iti Implant Course 2018 PDFDocument5 pagesIti Implant Course 2018 PDFShyam K MaharjanNo ratings yet
- Implant Surgical AnatomyDocument14 pagesImplant Surgical AnatomyKo YotoNo ratings yet
- Margin (Finish Line) PlacementDocument36 pagesMargin (Finish Line) PlacementIulia Florina Sima100% (1)
- Crown Lengthening A Comprehensive ReviewDocument11 pagesCrown Lengthening A Comprehensive ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Instrumen Endodontik PatahDocument8 pagesInstrumen Endodontik PatahKhamila TusyNo ratings yet
- Implant Thread Designs: An Overview: July 2017Document10 pagesImplant Thread Designs: An Overview: July 2017Seno FauziNo ratings yet
- Criteria For The Selection of Restoration Materials PDFDocument8 pagesCriteria For The Selection of Restoration Materials PDFSofia BoteroNo ratings yet
- Esthetic Considerations in Interdental Papilla PDFDocument11 pagesEsthetic Considerations in Interdental Papilla PDFXavier AltamiranoNo ratings yet
- Trauma From Occlusion (TFO) : DR Khurram Assist Prof Isra Dental CollegeDocument41 pagesTrauma From Occlusion (TFO) : DR Khurram Assist Prof Isra Dental CollegeShahid HameedNo ratings yet
- Optimizing Gingival EstheticsDocument8 pagesOptimizing Gingival EstheticsThe Bioclear Clinic100% (1)
- Difference Between Primary and Permanent TeethDocument17 pagesDifference Between Primary and Permanent TeethMohd Tauseef Khan100% (1)
- Articulating PapersDocument48 pagesArticulating PapersMayank MalraNo ratings yet
- Full Mouth Rehabilitation of The Patient With Severly Worn Out Dentition A Case Report.Document5 pagesFull Mouth Rehabilitation of The Patient With Severly Worn Out Dentition A Case Report.sivak_198100% (1)
- Cavity Classification and NomenclatureDocument23 pagesCavity Classification and Nomenclatureyahya100% (3)
- Rationale For Dental ImplantsDocument18 pagesRationale For Dental ImplantsSamir Nayyar100% (1)
- IRTDocument2 pagesIRTIgnacioNo ratings yet
- Gigi Tiruan GasketDocument5 pagesGigi Tiruan GasketGus BasyaNo ratings yet
- Cieszynski' Rule of IsometryDocument5 pagesCieszynski' Rule of Isometrynishant_tewari_1No ratings yet
- Microbrush Stamp Technique To Achieve Occlusal Topography For Composite Resin Restorations - A Technical ReportDocument7 pagesMicrobrush Stamp Technique To Achieve Occlusal Topography For Composite Resin Restorations - A Technical ReportabulzNo ratings yet
- Drug MetabolismDocument47 pagesDrug MetabolismDaniel WangNo ratings yet
- Chemical CarcinogenDocument54 pagesChemical CarcinogenDaniel WangNo ratings yet
- Metabolic Changes of DrugsDocument103 pagesMetabolic Changes of DrugsDaniel Wang100% (2)
- Drug Treatment of PsychosisDocument57 pagesDrug Treatment of PsychosisDaniel WangNo ratings yet
- Thermodynamic 1Document312 pagesThermodynamic 1Daniel Wang100% (5)
- Antidepressant DrugsDocument68 pagesAntidepressant DrugsMatthew PhillipsNo ratings yet
- Malnutrition & The Older PatientDocument66 pagesMalnutrition & The Older PatientDaniel WangNo ratings yet
- Antihistamines: Student Learning GoalsDocument45 pagesAntihistamines: Student Learning GoalsDaniel WangNo ratings yet
- OperIII 2-5-08Document18 pagesOperIII 2-5-08Daniel WangNo ratings yet
- Antiepileptics Medicinal ChemistryDocument30 pagesAntiepileptics Medicinal ChemistryDaniel WangNo ratings yet
- Class IV Composite Finish Past ResultsDocument34 pagesClass IV Composite Finish Past ResultsDaniel WangNo ratings yet
- Chemical CarcinogenDocument54 pagesChemical CarcinogenDaniel WangNo ratings yet
- Existing Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDocument44 pagesExisting Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDaniel WangNo ratings yet
- Class II Amalgam Preparation Past Results: - Outline Form - 1.85Document50 pagesClass II Amalgam Preparation Past Results: - Outline Form - 1.85Daniel WangNo ratings yet
- Existing Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDocument58 pagesExisting Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDaniel WangNo ratings yet
- Shade Matching: Division of Operative Dentistry Department of Restorative SciencesDocument34 pagesShade Matching: Division of Operative Dentistry Department of Restorative SciencesDaniel WangNo ratings yet
- Shade Matching: Division of Operative Dentistry Department of Restorative SciencesDocument34 pagesShade Matching: Division of Operative Dentistry Department of Restorative SciencesDaniel WangNo ratings yet
- Dental Caries: Diagnosis and Treatment OptionsDocument53 pagesDental Caries: Diagnosis and Treatment OptionsDaniel WangNo ratings yet
- Treatment Planning in Operative Dentistry: Dr. Ignatius LeeDocument42 pagesTreatment Planning in Operative Dentistry: Dr. Ignatius LeeDaniel Wang100% (1)
- Dent 5805 Operative Dentistry III: Course Director Dr. Ignatius Lee Office: 8-376b Moos EmailDocument19 pagesDent 5805 Operative Dentistry III: Course Director Dr. Ignatius Lee Office: 8-376b Moos EmailDaniel WangNo ratings yet
- 02 Class II Amalgams Examples)Document52 pages02 Class II Amalgams Examples)Daniel WangNo ratings yet
- Health Benefits of CoffeeDocument9 pagesHealth Benefits of CoffeeMaru PabloNo ratings yet
- CDF SPC All LOB Except HL LevelDocument2 pagesCDF SPC All LOB Except HL LevelSRIKANTA ROUTNo ratings yet
- Review of The NICE Guidelines For Multiple Myeloma: G. Pratt, T.C. MorrisDocument11 pagesReview of The NICE Guidelines For Multiple Myeloma: G. Pratt, T.C. MorrisHashim AhmadNo ratings yet
- The Aim of Medicine Is Not To Know The DiseaseDocument4 pagesThe Aim of Medicine Is Not To Know The DiseasekazchandranNo ratings yet
- Approach To Renal BiopsyDocument77 pagesApproach To Renal BiopsySandeep Kumar VushikamallaNo ratings yet
- BM482 Biomedical InstrumentationDocument2 pagesBM482 Biomedical InstrumentationmellumathewNo ratings yet
- Closed System: Eltek CpuntDocument2 pagesClosed System: Eltek CpuntLozorroNo ratings yet
- Konsep Dasar Epidemiologi Dan KependudukanDocument44 pagesKonsep Dasar Epidemiologi Dan Kependudukanandi pranataNo ratings yet
- Reflection On Bipolar DisorderDocument2 pagesReflection On Bipolar DisorderLaila GabrielNo ratings yet
- Final Quality Assurance ProgramDocument4 pagesFinal Quality Assurance ProgramGanie Mar BiasonNo ratings yet
- Ljl0wdga4zgftfjlachhji4oDocument3 pagesLjl0wdga4zgftfjlachhji4oAmitNo ratings yet
- Name Generic Class of Drug Patient'S Dose and Route Usual Dose Recommended Target Symptoms Drug Is Intended To Address Top 3-5 Nursing ImplicationsDocument3 pagesName Generic Class of Drug Patient'S Dose and Route Usual Dose Recommended Target Symptoms Drug Is Intended To Address Top 3-5 Nursing ImplicationsJay VillasotoNo ratings yet
- Perevod Behzod Nodira PDFDocument327 pagesPerevod Behzod Nodira PDFMayur WakchaureNo ratings yet
- Community Medicine: Guideline by Afaq Naeem (Aimc Batch 2k20)Document39 pagesCommunity Medicine: Guideline by Afaq Naeem (Aimc Batch 2k20)Saher ShahzadNo ratings yet
- London Cancer Lung Radiotherapy Guidelines 2013 v1 0Document24 pagesLondon Cancer Lung Radiotherapy Guidelines 2013 v1 0Cosmin SaftaNo ratings yet
- PREGABALINDocument5 pagesPREGABALINJojenelle R. TepaitNo ratings yet
- Introduction To The Astm E3219 Standard Guide For Derivation of Health Based Exposure Limits (Hbels)Document10 pagesIntroduction To The Astm E3219 Standard Guide For Derivation of Health Based Exposure Limits (Hbels)nsk79inNo ratings yet
- 3 Chronic MyringitisDocument19 pages3 Chronic MyringitissyahputriNo ratings yet
- Pembahasan UKDI CLINIC 3 Batch Mei 2016Document662 pagesPembahasan UKDI CLINIC 3 Batch Mei 2016widi kusumaNo ratings yet
- NCP Nursing Care Plans For Aplastic AnemiaDocument3 pagesNCP Nursing Care Plans For Aplastic AnemiaTahir Ali0% (1)
- Topical Immunomodulators in DermatologyDocument9 pagesTopical Immunomodulators in DermatologyRifky Budi TriyatnoNo ratings yet
- Literature Feeding and Eating Quick GuideDocument17 pagesLiterature Feeding and Eating Quick GuideHana alassafNo ratings yet
- BenzodiazepinesDocument7 pagesBenzodiazepinesRully B ChristinaNo ratings yet
- Journal CHFDocument9 pagesJournal CHFaniabNo ratings yet
- Benign and Malignant Tumors of Oral CavityDocument56 pagesBenign and Malignant Tumors of Oral CavityPawan Kumar83% (6)
- (Download PDF) Essentials of Radiology Common Indications and Interpretation 4Th Edition Mettler JR MD MPH Online Ebook All Chapter PDFDocument42 pages(Download PDF) Essentials of Radiology Common Indications and Interpretation 4Th Edition Mettler JR MD MPH Online Ebook All Chapter PDFtracy.freeman317100% (14)
- Mold ToxinsDocument7 pagesMold ToxinsMikiatlantul100% (1)
- Rekap BPJS Ri 2015 UpdateDocument373 pagesRekap BPJS Ri 2015 UpdateA- RONIENo ratings yet
- Oxfordshire ADULT Antimicrobial Prescribing Guidelines For Primary CareDocument21 pagesOxfordshire ADULT Antimicrobial Prescribing Guidelines For Primary CareDan IonescuNo ratings yet














































































































Download as ppt, pdf, or txt
You might also like
- USUHS Anesthesia Pharmacology NotesetDocument247 pagesUSUHS Anesthesia Pharmacology NotesetSean Bancroft100% (3)
- Basic Principles of Obturator Design For Partially Edentulous Patients. Part I: ClassificationDocument69 pagesBasic Principles of Obturator Design For Partially Edentulous Patients. Part I: ClassificationDrFarha NazNo ratings yet
- Anti Diabetic DrugsDocument58 pagesAnti Diabetic DrugsDaniel Wang100% (1)
- Opioids Medicinal ChemistryDocument38 pagesOpioids Medicinal ChemistryDaniel WangNo ratings yet
- Concept Map CVADocument1 pageConcept Map CVASuzette Rae Tate100% (2)
- Pickard's Manual-Tooth Wear (Dragged)Document8 pagesPickard's Manual-Tooth Wear (Dragged)Adit MehtaNo ratings yet
- Flap Surgery 2Document38 pagesFlap Surgery 2Fah100% (1)
- Definition:: Types of Forceps Used For Tooth ExtractionDocument28 pagesDefinition:: Types of Forceps Used For Tooth Extractionayman moaed alyasen100% (1)
- Tarrson Family Endowed Chair in PeriodonticsDocument54 pagesTarrson Family Endowed Chair in PeriodonticsAchyutSinhaNo ratings yet
- New Microsoft Office Word DocumentDocument3 pagesNew Microsoft Office Word DocumentAtulsanapNo ratings yet
- Single Flap Approach With and Without Guided TissueDocument21 pagesSingle Flap Approach With and Without Guided TissuekarthikNo ratings yet
- Techniques On Vertical Ridge Augmentation: Indications and EffectivenessDocument30 pagesTechniques On Vertical Ridge Augmentation: Indications and Effectivenessrmartins76No ratings yet
- MLV136 REV C Locator PresentationDocument58 pagesMLV136 REV C Locator PresentationS. BenzaquenNo ratings yet
- Porcelain Fused To Metal (PFM) Crowns and Caries in Adjacent TeetDocument5 pagesPorcelain Fused To Metal (PFM) Crowns and Caries in Adjacent Teetbaiq rengganis dewiNo ratings yet
- Challenges in Dentin BondingDocument11 pagesChallenges in Dentin BondingDanish SattarNo ratings yet
- ACP Complete EdentulismDocument89 pagesACP Complete EdentulismAshwin PangiNo ratings yet
- Polyetheretherketone PEEK Dental Implants A Case FDocument8 pagesPolyetheretherketone PEEK Dental Implants A Case FPhoebe David100% (1)
- Bedrossian Treatment Planning The Maxilla PDFDocument11 pagesBedrossian Treatment Planning The Maxilla PDFSitiKhadijahNo ratings yet
- Surgical Extrusion: A Dental TechniqueDocument6 pagesSurgical Extrusion: A Dental TechniqueDragos CiongaruNo ratings yet
- Use of Implants in The Pterygoid Region For Prosthodontic TreatmentDocument4 pagesUse of Implants in The Pterygoid Region For Prosthodontic TreatmentSidhartha KumarNo ratings yet
- Preprosthetic and Reconstructive SurgeryDocument32 pagesPreprosthetic and Reconstructive Surgeryruoiconmapu100% (1)
- Short Implants or GraftsDocument31 pagesShort Implants or GraftsJess YuanNo ratings yet
- C24024 - Harmonize Shade Guide - EN UK PDFDocument7 pagesC24024 - Harmonize Shade Guide - EN UK PDFFabio RibeiroNo ratings yet
- The Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFDocument7 pagesThe Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFAhmed Mohammed Saaduddin Sapri100% (1)
- Badly Broken MarzoukDocument68 pagesBadly Broken MarzoukHend MohamedNo ratings yet
- Direct Cuspal CoverageDocument8 pagesDirect Cuspal CoverageLuLu NikhlaturNo ratings yet
- Pulp Therapy For Primary and Immature Permanent TeethDocument11 pagesPulp Therapy For Primary and Immature Permanent TeethPrabhjot KaurNo ratings yet
- What Is Suturing?: - The Primary Objective Is To Position andDocument16 pagesWhat Is Suturing?: - The Primary Objective Is To Position andmehak malhotraNo ratings yet
- Regressive Changes of TeethDocument45 pagesRegressive Changes of TeethNader AlaizariNo ratings yet
- Instrument Used in ExodontaDocument32 pagesInstrument Used in ExodontaNoor Abdullah AlNo ratings yet
- Wisdom Tooth WisdomDocument134 pagesWisdom Tooth WisdomPaulo Rabelo Jr.100% (1)
- Dentin Bonding Agents - An OverviewDocument4 pagesDentin Bonding Agents - An OverviewIOSRjournalNo ratings yet
- Surgical Vs Non-Surgical Approach in PeriodonticsDocument13 pagesSurgical Vs Non-Surgical Approach in PeriodonticsBea DominguezNo ratings yet
- Alloderm Surgical Technique Guide PDFDocument8 pagesAlloderm Surgical Technique Guide PDFamagueNo ratings yet
- Material Options For Class II Composite Restorations - Varied Clinical Parameters Require Different TechniquesDocument6 pagesMaterial Options For Class II Composite Restorations - Varied Clinical Parameters Require Different TechniquesMohammed NabeelNo ratings yet
- Anterior Cross-Bite Conference On 16092010Document42 pagesAnterior Cross-Bite Conference On 16092010Dent YomarajNo ratings yet
- Alveolar Ridge Preservation Utilizing The Socket-Plug TechniqueDocument7 pagesAlveolar Ridge Preservation Utilizing The Socket-Plug Techniquekeily rodriguez100% (1)
- Implants in Esthetic ZoneDocument10 pagesImplants in Esthetic ZoneInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- MANUAL FOR OPERATIVE DENTISTRY - Xa - Yimg.com (PDFDrive)Document169 pagesMANUAL FOR OPERATIVE DENTISTRY - Xa - Yimg.com (PDFDrive)cvpk prasannaNo ratings yet
- Oral Manifestations of Denture AbuseDocument53 pagesOral Manifestations of Denture AbuseBharanija100% (2)
- 3.factors and Techniques Influencing Peri-Implant Papillae - PDFDocument12 pages3.factors and Techniques Influencing Peri-Implant Papillae - PDFMargarita María Blanco LópezNo ratings yet
- Fundamentals of Cavity PreprationDocument70 pagesFundamentals of Cavity PreprationSATNAMNo ratings yet
- Iti Implant Course 2018 PDFDocument5 pagesIti Implant Course 2018 PDFShyam K MaharjanNo ratings yet
- Implant Surgical AnatomyDocument14 pagesImplant Surgical AnatomyKo YotoNo ratings yet
- Margin (Finish Line) PlacementDocument36 pagesMargin (Finish Line) PlacementIulia Florina Sima100% (1)
- Crown Lengthening A Comprehensive ReviewDocument11 pagesCrown Lengthening A Comprehensive ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Instrumen Endodontik PatahDocument8 pagesInstrumen Endodontik PatahKhamila TusyNo ratings yet
- Implant Thread Designs: An Overview: July 2017Document10 pagesImplant Thread Designs: An Overview: July 2017Seno FauziNo ratings yet
- Criteria For The Selection of Restoration Materials PDFDocument8 pagesCriteria For The Selection of Restoration Materials PDFSofia BoteroNo ratings yet
- Esthetic Considerations in Interdental Papilla PDFDocument11 pagesEsthetic Considerations in Interdental Papilla PDFXavier AltamiranoNo ratings yet
- Trauma From Occlusion (TFO) : DR Khurram Assist Prof Isra Dental CollegeDocument41 pagesTrauma From Occlusion (TFO) : DR Khurram Assist Prof Isra Dental CollegeShahid HameedNo ratings yet
- Optimizing Gingival EstheticsDocument8 pagesOptimizing Gingival EstheticsThe Bioclear Clinic100% (1)
- Difference Between Primary and Permanent TeethDocument17 pagesDifference Between Primary and Permanent TeethMohd Tauseef Khan100% (1)
- Articulating PapersDocument48 pagesArticulating PapersMayank MalraNo ratings yet
- Full Mouth Rehabilitation of The Patient With Severly Worn Out Dentition A Case Report.Document5 pagesFull Mouth Rehabilitation of The Patient With Severly Worn Out Dentition A Case Report.sivak_198100% (1)
- Cavity Classification and NomenclatureDocument23 pagesCavity Classification and Nomenclatureyahya100% (3)
- Rationale For Dental ImplantsDocument18 pagesRationale For Dental ImplantsSamir Nayyar100% (1)
- IRTDocument2 pagesIRTIgnacioNo ratings yet
- Gigi Tiruan GasketDocument5 pagesGigi Tiruan GasketGus BasyaNo ratings yet
- Cieszynski' Rule of IsometryDocument5 pagesCieszynski' Rule of Isometrynishant_tewari_1No ratings yet
- Microbrush Stamp Technique To Achieve Occlusal Topography For Composite Resin Restorations - A Technical ReportDocument7 pagesMicrobrush Stamp Technique To Achieve Occlusal Topography For Composite Resin Restorations - A Technical ReportabulzNo ratings yet
- Drug MetabolismDocument47 pagesDrug MetabolismDaniel WangNo ratings yet
- Chemical CarcinogenDocument54 pagesChemical CarcinogenDaniel WangNo ratings yet
- Metabolic Changes of DrugsDocument103 pagesMetabolic Changes of DrugsDaniel Wang100% (2)
- Drug Treatment of PsychosisDocument57 pagesDrug Treatment of PsychosisDaniel WangNo ratings yet
- Thermodynamic 1Document312 pagesThermodynamic 1Daniel Wang100% (5)
- Antidepressant DrugsDocument68 pagesAntidepressant DrugsMatthew PhillipsNo ratings yet
- Malnutrition & The Older PatientDocument66 pagesMalnutrition & The Older PatientDaniel WangNo ratings yet
- Antihistamines: Student Learning GoalsDocument45 pagesAntihistamines: Student Learning GoalsDaniel WangNo ratings yet
- OperIII 2-5-08Document18 pagesOperIII 2-5-08Daniel WangNo ratings yet
- Antiepileptics Medicinal ChemistryDocument30 pagesAntiepileptics Medicinal ChemistryDaniel WangNo ratings yet
- Class IV Composite Finish Past ResultsDocument34 pagesClass IV Composite Finish Past ResultsDaniel WangNo ratings yet
- Chemical CarcinogenDocument54 pagesChemical CarcinogenDaniel WangNo ratings yet
- Existing Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDocument44 pagesExisting Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDaniel WangNo ratings yet
- Class II Amalgam Preparation Past Results: - Outline Form - 1.85Document50 pagesClass II Amalgam Preparation Past Results: - Outline Form - 1.85Daniel WangNo ratings yet
- Existing Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDocument58 pagesExisting Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDaniel WangNo ratings yet
- Shade Matching: Division of Operative Dentistry Department of Restorative SciencesDocument34 pagesShade Matching: Division of Operative Dentistry Department of Restorative SciencesDaniel WangNo ratings yet
- Shade Matching: Division of Operative Dentistry Department of Restorative SciencesDocument34 pagesShade Matching: Division of Operative Dentistry Department of Restorative SciencesDaniel WangNo ratings yet
- Dental Caries: Diagnosis and Treatment OptionsDocument53 pagesDental Caries: Diagnosis and Treatment OptionsDaniel WangNo ratings yet
- Treatment Planning in Operative Dentistry: Dr. Ignatius LeeDocument42 pagesTreatment Planning in Operative Dentistry: Dr. Ignatius LeeDaniel Wang100% (1)
- Dent 5805 Operative Dentistry III: Course Director Dr. Ignatius Lee Office: 8-376b Moos EmailDocument19 pagesDent 5805 Operative Dentistry III: Course Director Dr. Ignatius Lee Office: 8-376b Moos EmailDaniel WangNo ratings yet
- 02 Class II Amalgams Examples)Document52 pages02 Class II Amalgams Examples)Daniel WangNo ratings yet
- Health Benefits of CoffeeDocument9 pagesHealth Benefits of CoffeeMaru PabloNo ratings yet
- CDF SPC All LOB Except HL LevelDocument2 pagesCDF SPC All LOB Except HL LevelSRIKANTA ROUTNo ratings yet
- Review of The NICE Guidelines For Multiple Myeloma: G. Pratt, T.C. MorrisDocument11 pagesReview of The NICE Guidelines For Multiple Myeloma: G. Pratt, T.C. MorrisHashim AhmadNo ratings yet
- The Aim of Medicine Is Not To Know The DiseaseDocument4 pagesThe Aim of Medicine Is Not To Know The DiseasekazchandranNo ratings yet
- Approach To Renal BiopsyDocument77 pagesApproach To Renal BiopsySandeep Kumar VushikamallaNo ratings yet
- BM482 Biomedical InstrumentationDocument2 pagesBM482 Biomedical InstrumentationmellumathewNo ratings yet
- Closed System: Eltek CpuntDocument2 pagesClosed System: Eltek CpuntLozorroNo ratings yet
- Konsep Dasar Epidemiologi Dan KependudukanDocument44 pagesKonsep Dasar Epidemiologi Dan Kependudukanandi pranataNo ratings yet
- Reflection On Bipolar DisorderDocument2 pagesReflection On Bipolar DisorderLaila GabrielNo ratings yet
- Final Quality Assurance ProgramDocument4 pagesFinal Quality Assurance ProgramGanie Mar BiasonNo ratings yet
- Ljl0wdga4zgftfjlachhji4oDocument3 pagesLjl0wdga4zgftfjlachhji4oAmitNo ratings yet
- Name Generic Class of Drug Patient'S Dose and Route Usual Dose Recommended Target Symptoms Drug Is Intended To Address Top 3-5 Nursing ImplicationsDocument3 pagesName Generic Class of Drug Patient'S Dose and Route Usual Dose Recommended Target Symptoms Drug Is Intended To Address Top 3-5 Nursing ImplicationsJay VillasotoNo ratings yet
- Perevod Behzod Nodira PDFDocument327 pagesPerevod Behzod Nodira PDFMayur WakchaureNo ratings yet
- Community Medicine: Guideline by Afaq Naeem (Aimc Batch 2k20)Document39 pagesCommunity Medicine: Guideline by Afaq Naeem (Aimc Batch 2k20)Saher ShahzadNo ratings yet
- London Cancer Lung Radiotherapy Guidelines 2013 v1 0Document24 pagesLondon Cancer Lung Radiotherapy Guidelines 2013 v1 0Cosmin SaftaNo ratings yet
- PREGABALINDocument5 pagesPREGABALINJojenelle R. TepaitNo ratings yet
- Introduction To The Astm E3219 Standard Guide For Derivation of Health Based Exposure Limits (Hbels)Document10 pagesIntroduction To The Astm E3219 Standard Guide For Derivation of Health Based Exposure Limits (Hbels)nsk79inNo ratings yet
- 3 Chronic MyringitisDocument19 pages3 Chronic MyringitissyahputriNo ratings yet
- Pembahasan UKDI CLINIC 3 Batch Mei 2016Document662 pagesPembahasan UKDI CLINIC 3 Batch Mei 2016widi kusumaNo ratings yet
- NCP Nursing Care Plans For Aplastic AnemiaDocument3 pagesNCP Nursing Care Plans For Aplastic AnemiaTahir Ali0% (1)
- Topical Immunomodulators in DermatologyDocument9 pagesTopical Immunomodulators in DermatologyRifky Budi TriyatnoNo ratings yet
- Literature Feeding and Eating Quick GuideDocument17 pagesLiterature Feeding and Eating Quick GuideHana alassafNo ratings yet
- BenzodiazepinesDocument7 pagesBenzodiazepinesRully B ChristinaNo ratings yet
- Journal CHFDocument9 pagesJournal CHFaniabNo ratings yet
- Benign and Malignant Tumors of Oral CavityDocument56 pagesBenign and Malignant Tumors of Oral CavityPawan Kumar83% (6)
- (Download PDF) Essentials of Radiology Common Indications and Interpretation 4Th Edition Mettler JR MD MPH Online Ebook All Chapter PDFDocument42 pages(Download PDF) Essentials of Radiology Common Indications and Interpretation 4Th Edition Mettler JR MD MPH Online Ebook All Chapter PDFtracy.freeman317100% (14)
- Mold ToxinsDocument7 pagesMold ToxinsMikiatlantul100% (1)
- Rekap BPJS Ri 2015 UpdateDocument373 pagesRekap BPJS Ri 2015 UpdateA- RONIENo ratings yet
- Oxfordshire ADULT Antimicrobial Prescribing Guidelines For Primary CareDocument21 pagesOxfordshire ADULT Antimicrobial Prescribing Guidelines For Primary CareDan IonescuNo ratings yet