
Jurnal Reading CABG MVR
Jurnal Reading CABG MVR
You might also like
- Gardner Timothy-Operative Cardiac Surgery Fifth Edition-CRC Press 2004Document937 pagesGardner Timothy-Operative Cardiac Surgery Fifth Edition-CRC Press 2004Elias Talani100% (3)
- A Review On Coronary Artery Disease, Its Risk Factors, and TherapeuticsDocument12 pagesA Review On Coronary Artery Disease, Its Risk Factors, and TherapeuticsshishichanNo ratings yet
- Cardiovascular Examination - OSCE Guide - Geeky MedicsDocument6 pagesCardiovascular Examination - OSCE Guide - Geeky MedicsJahangir AlamNo ratings yet
- Cardiogenic Shock: Updated Approach To ManagementDocument49 pagesCardiogenic Shock: Updated Approach To ManagementelsarahmiNo ratings yet
- Offpump Versus Onpump Cabg A Systematic Review and Analysis of 2018Document45 pagesOffpump Versus Onpump Cabg A Systematic Review and Analysis of 2018Anna Sofía ParedesNo ratings yet
- Chambers Et Al. 2019 - OA Vs RA in BifurcationDocument4 pagesChambers Et Al. 2019 - OA Vs RA in BifurcationPraveenVeeraNo ratings yet
- CABG - On Pump Vs Off Pump - AHA 2005Document7 pagesCABG - On Pump Vs Off Pump - AHA 2005odiseu81No ratings yet
- Mitral Durability After Robotic Mitral Valve Repair: Analysis of 200 Consecutive Mitral Regurgitation RepairsDocument7 pagesMitral Durability After Robotic Mitral Valve Repair: Analysis of 200 Consecutive Mitral Regurgitation RepairsEnrico SquiccimarroNo ratings yet
- RRT in Aki: Moderator: Dr. Manoj C PRESENTER: Dr. Prasad SMDocument64 pagesRRT in Aki: Moderator: Dr. Manoj C PRESENTER: Dr. Prasad SMSrinivas Mahesh PrasadNo ratings yet
- Cabg ConduitDocument23 pagesCabg ConduitVijay AnandNo ratings yet
- Research Cardiac SurgeryDocument7 pagesResearch Cardiac SurgeryImran KalyarNo ratings yet
- Adequate Lymph Node Assessment For Extrahepatic Bile Duct AdenocarcinomaDocument17 pagesAdequate Lymph Node Assessment For Extrahepatic Bile Duct Adenocarcinoma140111No ratings yet
- Jurnal 2_Coronary artery bypass surgery for ACSDocument10 pagesJurnal 2_Coronary artery bypass surgery for ACSjerrylmn999No ratings yet
- Critical Appraisal of The International Subarachnoid Aneurysm Trial (ISAT)Document7 pagesCritical Appraisal of The International Subarachnoid Aneurysm Trial (ISAT)Setiawan Arif WibowoNo ratings yet
- Renu VHDDocument91 pagesRenu VHDRenu KhedekarNo ratings yet
- ESC-2023 Day 3 UpdatesDocument41 pagesESC-2023 Day 3 UpdatesIvan TeongNo ratings yet
- Department of Pharmacy Practice Sultan Ul Uloom College of Pharmacy (Approved by AICTE & PCI, A Liated To JNTUH) Mount Pleasant, Road No.3, Banjara Hills, Hyderabad 500 034Document14 pagesDepartment of Pharmacy Practice Sultan Ul Uloom College of Pharmacy (Approved by AICTE & PCI, A Liated To JNTUH) Mount Pleasant, Road No.3, Banjara Hills, Hyderabad 500 034sufiya fatimaNo ratings yet
- En V27n4a04Document4 pagesEn V27n4a04Rodrigo AbreuNo ratings yet
- Trials-and-Guidelines 2 SpoonerDocument72 pagesTrials-and-Guidelines 2 SpoonerVimal NishadNo ratings yet
- The Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsDocument5 pagesThe Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsM Ali AdrianNo ratings yet
- PBM (Autosaved)Document36 pagesPBM (Autosaved)dr AmitNo ratings yet
- 5 Year Results of The COAPT Trial What Did We LeaDocument2 pages5 Year Results of The COAPT Trial What Did We LeaSamuel DNo ratings yet
- 102-Article Text-462-3-2-20200510Document10 pages102-Article Text-462-3-2-20200510Andre Boca Ribas FreitasNo ratings yet
- Nihms 644313Document18 pagesNihms 644313Toli kkakrNo ratings yet
- Dr. M Sahal - MitralDocument35 pagesDr. M Sahal - MitralHari Mas KuncoroNo ratings yet
- An International Consensus Statement On The Management of Postoperative Anaemia After Major Surgical ProceduresDocument14 pagesAn International Consensus Statement On The Management of Postoperative Anaemia After Major Surgical ProceduresEdwin PradanaNo ratings yet
- Wjem 23 358Document10 pagesWjem 23 358drsubramanianNo ratings yet
- Clinical Oncology AssignmentDocument8 pagesClinical Oncology Assignmentapi-598481829No ratings yet
- Overview of Treatment Approaches For Hepatocellular Carcinoma - UpToDateDocument66 pagesOverview of Treatment Approaches For Hepatocellular Carcinoma - UpToDateJoyce SumagaysayNo ratings yet
- Assessment of Left Ventricular Function by EchocardiographyDocument15 pagesAssessment of Left Ventricular Function by EchocardiographyramangNo ratings yet
- The Barrow Ruptured Aneurysm Trial - 6-Year ResultsDocument9 pagesThe Barrow Ruptured Aneurysm Trial - 6-Year ResultsJulieta PereyraNo ratings yet
- Fana Alemseged Endovascular Thrombectomy For Basil - 231118 - 114208Document8 pagesFana Alemseged Endovascular Thrombectomy For Basil - 231118 - 114208Luis Guilherme ScalianteNo ratings yet
- Infrainguinal Disease - Endovascular TherapyDocument24 pagesInfrainguinal Disease - Endovascular TherapyvsurgeonkamranNo ratings yet
- Discussion On The PapDiscussion On The Paper: Cost-Effectiveness of Implantable Cardioverter-DefibrillatorserDocument5 pagesDiscussion On The PapDiscussion On The Paper: Cost-Effectiveness of Implantable Cardioverter-Defibrillatorsersin001No ratings yet
- Percutaneous Mitral Valve Intervention TerreDocument37 pagesPercutaneous Mitral Valve Intervention Terrejezreel terreNo ratings yet
- Carotid Endarterectomy FinalDocument48 pagesCarotid Endarterectomy Finalimad mokalledNo ratings yet
- Presentation 1Document21 pagesPresentation 1abdulrafaykamalNo ratings yet
- Cabg Vs OpcabDocument17 pagesCabg Vs OpcabVijay AnandNo ratings yet
- National Incidence and Impact of Non-Infectious Urethral Catheter Related Complications On The Surgical Care Improvement ProjectDocument20 pagesNational Incidence and Impact of Non-Infectious Urethral Catheter Related Complications On The Surgical Care Improvement ProjectIsabella RoselliniNo ratings yet
- Adherence To Practice Guidelines: The Role of Specialty Society GuidelinesDocument12 pagesAdherence To Practice Guidelines: The Role of Specialty Society GuidelinesMariangelRodriguez55No ratings yet
- Echocardiography in Hemodynamic MonitoringDocument5 pagesEchocardiography in Hemodynamic MonitoringDr.Biswajit jenaNo ratings yet
- Management of Non Responders To CRT - A Practical Guide: DR G.Raghu KishoreDocument102 pagesManagement of Non Responders To CRT - A Practical Guide: DR G.Raghu KishoreMonica MonikaNo ratings yet
- Lower Extremity AmputationDocument41 pagesLower Extremity AmputationvsurgeonkamranNo ratings yet
- Stenting Versus Endarterectomy For Treatment of Carotid-Artery Stenosis (CREST Trial)Document11 pagesStenting Versus Endarterectomy For Treatment of Carotid-Artery Stenosis (CREST Trial)sirrfsNo ratings yet
- An Overview of Therapeutic Plasma ExchangeDocument65 pagesAn Overview of Therapeutic Plasma ExchangesayednourNo ratings yet
- 247 FullDocument8 pages247 FullRifqi AnraNo ratings yet
- Journal Critique Technical MethodsDocument4 pagesJournal Critique Technical MethodsJam SalazarNo ratings yet
- Laparoscopic Cholecystectomy Conversion Rates Two Decades LaterDocument8 pagesLaparoscopic Cholecystectomy Conversion Rates Two Decades LaterLuis Carlos Moncada TorresNo ratings yet
- The PCQP Score For Volume Status of Acutely Ill Patients - Integrating Vascular Pedicle Width, Caval Index, Respiratory Variability of The QRS Complex and R Wave AmplitudeDocument8 pagesThe PCQP Score For Volume Status of Acutely Ill Patients - Integrating Vascular Pedicle Width, Caval Index, Respiratory Variability of The QRS Complex and R Wave AmplitudeSoftwarebolivia EnriqueNo ratings yet
- What's New in The SICU: Douglas JE Schuerer, MD FACS Director of TraumaDocument54 pagesWhat's New in The SICU: Douglas JE Schuerer, MD FACS Director of Traumacrt0518No ratings yet
- AKI and CRRT RelationDocument10 pagesAKI and CRRT RelationZainab MotiwalaNo ratings yet
- Principles and Pitfalls in Coronary Vasomotor Function TestingDocument26 pagesPrinciples and Pitfalls in Coronary Vasomotor Function TestingRamón López PalopNo ratings yet
- Graft Patency After Off-Pump Versus On-Pump Coronary Artery Surgery in High-Risk PatientsDocument8 pagesGraft Patency After Off-Pump Versus On-Pump Coronary Artery Surgery in High-Risk PatientsZul FikarNo ratings yet
- Onwudike 2020Document10 pagesOnwudike 2020Han's OfficialNo ratings yet
- Journal of Cardiothoracic SurgeryDocument9 pagesJournal of Cardiothoracic SurgeryThanh BinhNo ratings yet
- Colloids Vs CrytaloidsDocument12 pagesColloids Vs CrytaloidsalimustagialgiNo ratings yet
- What Is OpcabDocument17 pagesWhat Is OpcabGrace Marie Sanchez-AguilarNo ratings yet
- Ivs 459Document3 pagesIvs 459melon segerNo ratings yet
- Evaluation of Factors Affecting Liver Function Test in Patients Underwent Coronary Artery Bypass Graft SurgeryDocument7 pagesEvaluation of Factors Affecting Liver Function Test in Patients Underwent Coronary Artery Bypass Graft SurgeryajmrdNo ratings yet
- Lesion Manguio Rotador en AmDocument5 pagesLesion Manguio Rotador en AmRelviGuzmanApazaNo ratings yet
- Goyal Et Al-2015-Annals of NeurologyDocument7 pagesGoyal Et Al-2015-Annals of NeurologyWinda Wahyu IkaputriNo ratings yet
- Intravascular ShuntDocument33 pagesIntravascular ShuntNatalindah Jokiem Woecandra T. D.No ratings yet
- Sherif Mokhtar, MD: Professor of Cardiology, Professor of Critical Care Medicine Cairo UniversityDocument85 pagesSherif Mokhtar, MD: Professor of Cardiology, Professor of Critical Care Medicine Cairo UniversityShimmering MoonNo ratings yet
- ECG NotesDocument7 pagesECG NotesShams NabeelNo ratings yet
- 3 - Deteksi Dini CHF - 22.3.23Document53 pages3 - Deteksi Dini CHF - 22.3.23tioNo ratings yet
- Cor Radiology (Kuliah Cardiovascular) 2011Document51 pagesCor Radiology (Kuliah Cardiovascular) 2011athayafebNo ratings yet
- Mcqs Pediatric Cardiology EmergencyDocument29 pagesMcqs Pediatric Cardiology EmergencyOmed M. AhmedNo ratings yet
- SVT CaseDocument11 pagesSVT CaseZakiy AzzuhdiNo ratings yet
- Vereckei TVDocument12 pagesVereckei TVVallejo Romo Alberto CristianNo ratings yet
- ACLS Algorithms SlideDocument26 pagesACLS Algorithms SlidehrsoNo ratings yet
- Atrial FibrilationDocument27 pagesAtrial FibrilationemialevelaNo ratings yet
- OSCEs SyllabusDocument133 pagesOSCEs SyllabusAnusha VergheseNo ratings yet
- 1500 Ebook Clinical Medicine Up PDFDocument215 pages1500 Ebook Clinical Medicine Up PDFAhmad Arif100% (1)
- What Is ArrhythmiaDocument14 pagesWhat Is ArrhythmiaSharan MurugaboopathyNo ratings yet
- 2022.02.10 MCCQE Study Plan Canada 2Document52 pages2022.02.10 MCCQE Study Plan Canada 2joann15marrieNo ratings yet
- European Examination in General Cardiology (EEGC) : Jim Hall Celine CarreraDocument37 pagesEuropean Examination in General Cardiology (EEGC) : Jim Hall Celine CarreraTasya MDNo ratings yet
- Nadolol (RX) : Category: Beta-BlockersDocument6 pagesNadolol (RX) : Category: Beta-BlockersSerious BlackNo ratings yet
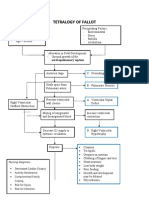
- Concept Map Tetralogy of FallotDocument2 pagesConcept Map Tetralogy of FallotKarl KiwisNo ratings yet
- Congenital Heart DefectsDocument13 pagesCongenital Heart DefectsGheluzee Herrera100% (2)
- Daftar Pustaka: Universitas Sumatera UtaraDocument2 pagesDaftar Pustaka: Universitas Sumatera UtaraNavisa HaifaNo ratings yet
- Syllab BSC RTDocument24 pagesSyllab BSC RTKiruba HaranNo ratings yet
- Rilantono, Lily L. 5 Rahasia Penyakit Kardiovaskular (PKV) - Jakarta: Badan Penerbit Fakultas Kedokteran Universitas Indonesia 2012. p.279-287Document1 pageRilantono, Lily L. 5 Rahasia Penyakit Kardiovaskular (PKV) - Jakarta: Badan Penerbit Fakultas Kedokteran Universitas Indonesia 2012. p.279-287Tegar DharmaNo ratings yet
- VT Origin PDFDocument60 pagesVT Origin PDFNikita PratamaNo ratings yet
- Azure™ XT DR MRI SureScan™ W2DR01Document44 pagesAzure™ XT DR MRI SureScan™ W2DR01mytake100No ratings yet
- Pharmacology Review Questions For QuizDocument14 pagesPharmacology Review Questions For QuizusedforfunplocNo ratings yet
- Cir 0000000000001054Document16 pagesCir 0000000000001054Code ValmirNo ratings yet
- Cath Lab ReportDocument13 pagesCath Lab ReportNasim AhmadNo ratings yet
- Nej M Abbotts TentDocument11 pagesNej M Abbotts TentWKYC.comNo ratings yet
- Cardiovascular ExaminationDocument4 pagesCardiovascular ExaminationarchanaNo ratings yet























































































Download as pptx, pdf, or txt
You might also like
- Gardner Timothy-Operative Cardiac Surgery Fifth Edition-CRC Press 2004Document937 pagesGardner Timothy-Operative Cardiac Surgery Fifth Edition-CRC Press 2004Elias Talani100% (3)
- A Review On Coronary Artery Disease, Its Risk Factors, and TherapeuticsDocument12 pagesA Review On Coronary Artery Disease, Its Risk Factors, and TherapeuticsshishichanNo ratings yet
- Cardiovascular Examination - OSCE Guide - Geeky MedicsDocument6 pagesCardiovascular Examination - OSCE Guide - Geeky MedicsJahangir AlamNo ratings yet
- Cardiogenic Shock: Updated Approach To ManagementDocument49 pagesCardiogenic Shock: Updated Approach To ManagementelsarahmiNo ratings yet
- Offpump Versus Onpump Cabg A Systematic Review and Analysis of 2018Document45 pagesOffpump Versus Onpump Cabg A Systematic Review and Analysis of 2018Anna Sofía ParedesNo ratings yet
- Chambers Et Al. 2019 - OA Vs RA in BifurcationDocument4 pagesChambers Et Al. 2019 - OA Vs RA in BifurcationPraveenVeeraNo ratings yet
- CABG - On Pump Vs Off Pump - AHA 2005Document7 pagesCABG - On Pump Vs Off Pump - AHA 2005odiseu81No ratings yet
- Mitral Durability After Robotic Mitral Valve Repair: Analysis of 200 Consecutive Mitral Regurgitation RepairsDocument7 pagesMitral Durability After Robotic Mitral Valve Repair: Analysis of 200 Consecutive Mitral Regurgitation RepairsEnrico SquiccimarroNo ratings yet
- RRT in Aki: Moderator: Dr. Manoj C PRESENTER: Dr. Prasad SMDocument64 pagesRRT in Aki: Moderator: Dr. Manoj C PRESENTER: Dr. Prasad SMSrinivas Mahesh PrasadNo ratings yet
- Cabg ConduitDocument23 pagesCabg ConduitVijay AnandNo ratings yet
- Research Cardiac SurgeryDocument7 pagesResearch Cardiac SurgeryImran KalyarNo ratings yet
- Adequate Lymph Node Assessment For Extrahepatic Bile Duct AdenocarcinomaDocument17 pagesAdequate Lymph Node Assessment For Extrahepatic Bile Duct Adenocarcinoma140111No ratings yet
- Jurnal 2_Coronary artery bypass surgery for ACSDocument10 pagesJurnal 2_Coronary artery bypass surgery for ACSjerrylmn999No ratings yet
- Critical Appraisal of The International Subarachnoid Aneurysm Trial (ISAT)Document7 pagesCritical Appraisal of The International Subarachnoid Aneurysm Trial (ISAT)Setiawan Arif WibowoNo ratings yet
- Renu VHDDocument91 pagesRenu VHDRenu KhedekarNo ratings yet
- ESC-2023 Day 3 UpdatesDocument41 pagesESC-2023 Day 3 UpdatesIvan TeongNo ratings yet
- Department of Pharmacy Practice Sultan Ul Uloom College of Pharmacy (Approved by AICTE & PCI, A Liated To JNTUH) Mount Pleasant, Road No.3, Banjara Hills, Hyderabad 500 034Document14 pagesDepartment of Pharmacy Practice Sultan Ul Uloom College of Pharmacy (Approved by AICTE & PCI, A Liated To JNTUH) Mount Pleasant, Road No.3, Banjara Hills, Hyderabad 500 034sufiya fatimaNo ratings yet
- En V27n4a04Document4 pagesEn V27n4a04Rodrigo AbreuNo ratings yet
- Trials-and-Guidelines 2 SpoonerDocument72 pagesTrials-and-Guidelines 2 SpoonerVimal NishadNo ratings yet
- The Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsDocument5 pagesThe Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsM Ali AdrianNo ratings yet
- PBM (Autosaved)Document36 pagesPBM (Autosaved)dr AmitNo ratings yet
- 5 Year Results of The COAPT Trial What Did We LeaDocument2 pages5 Year Results of The COAPT Trial What Did We LeaSamuel DNo ratings yet
- 102-Article Text-462-3-2-20200510Document10 pages102-Article Text-462-3-2-20200510Andre Boca Ribas FreitasNo ratings yet
- Nihms 644313Document18 pagesNihms 644313Toli kkakrNo ratings yet
- Dr. M Sahal - MitralDocument35 pagesDr. M Sahal - MitralHari Mas KuncoroNo ratings yet
- An International Consensus Statement On The Management of Postoperative Anaemia After Major Surgical ProceduresDocument14 pagesAn International Consensus Statement On The Management of Postoperative Anaemia After Major Surgical ProceduresEdwin PradanaNo ratings yet
- Wjem 23 358Document10 pagesWjem 23 358drsubramanianNo ratings yet
- Clinical Oncology AssignmentDocument8 pagesClinical Oncology Assignmentapi-598481829No ratings yet
- Overview of Treatment Approaches For Hepatocellular Carcinoma - UpToDateDocument66 pagesOverview of Treatment Approaches For Hepatocellular Carcinoma - UpToDateJoyce SumagaysayNo ratings yet
- Assessment of Left Ventricular Function by EchocardiographyDocument15 pagesAssessment of Left Ventricular Function by EchocardiographyramangNo ratings yet
- The Barrow Ruptured Aneurysm Trial - 6-Year ResultsDocument9 pagesThe Barrow Ruptured Aneurysm Trial - 6-Year ResultsJulieta PereyraNo ratings yet
- Fana Alemseged Endovascular Thrombectomy For Basil - 231118 - 114208Document8 pagesFana Alemseged Endovascular Thrombectomy For Basil - 231118 - 114208Luis Guilherme ScalianteNo ratings yet
- Infrainguinal Disease - Endovascular TherapyDocument24 pagesInfrainguinal Disease - Endovascular TherapyvsurgeonkamranNo ratings yet
- Discussion On The PapDiscussion On The Paper: Cost-Effectiveness of Implantable Cardioverter-DefibrillatorserDocument5 pagesDiscussion On The PapDiscussion On The Paper: Cost-Effectiveness of Implantable Cardioverter-Defibrillatorsersin001No ratings yet
- Percutaneous Mitral Valve Intervention TerreDocument37 pagesPercutaneous Mitral Valve Intervention Terrejezreel terreNo ratings yet
- Carotid Endarterectomy FinalDocument48 pagesCarotid Endarterectomy Finalimad mokalledNo ratings yet
- Presentation 1Document21 pagesPresentation 1abdulrafaykamalNo ratings yet
- Cabg Vs OpcabDocument17 pagesCabg Vs OpcabVijay AnandNo ratings yet
- National Incidence and Impact of Non-Infectious Urethral Catheter Related Complications On The Surgical Care Improvement ProjectDocument20 pagesNational Incidence and Impact of Non-Infectious Urethral Catheter Related Complications On The Surgical Care Improvement ProjectIsabella RoselliniNo ratings yet
- Adherence To Practice Guidelines: The Role of Specialty Society GuidelinesDocument12 pagesAdherence To Practice Guidelines: The Role of Specialty Society GuidelinesMariangelRodriguez55No ratings yet
- Echocardiography in Hemodynamic MonitoringDocument5 pagesEchocardiography in Hemodynamic MonitoringDr.Biswajit jenaNo ratings yet
- Management of Non Responders To CRT - A Practical Guide: DR G.Raghu KishoreDocument102 pagesManagement of Non Responders To CRT - A Practical Guide: DR G.Raghu KishoreMonica MonikaNo ratings yet
- Lower Extremity AmputationDocument41 pagesLower Extremity AmputationvsurgeonkamranNo ratings yet
- Stenting Versus Endarterectomy For Treatment of Carotid-Artery Stenosis (CREST Trial)Document11 pagesStenting Versus Endarterectomy For Treatment of Carotid-Artery Stenosis (CREST Trial)sirrfsNo ratings yet
- An Overview of Therapeutic Plasma ExchangeDocument65 pagesAn Overview of Therapeutic Plasma ExchangesayednourNo ratings yet
- 247 FullDocument8 pages247 FullRifqi AnraNo ratings yet
- Journal Critique Technical MethodsDocument4 pagesJournal Critique Technical MethodsJam SalazarNo ratings yet
- Laparoscopic Cholecystectomy Conversion Rates Two Decades LaterDocument8 pagesLaparoscopic Cholecystectomy Conversion Rates Two Decades LaterLuis Carlos Moncada TorresNo ratings yet
- The PCQP Score For Volume Status of Acutely Ill Patients - Integrating Vascular Pedicle Width, Caval Index, Respiratory Variability of The QRS Complex and R Wave AmplitudeDocument8 pagesThe PCQP Score For Volume Status of Acutely Ill Patients - Integrating Vascular Pedicle Width, Caval Index, Respiratory Variability of The QRS Complex and R Wave AmplitudeSoftwarebolivia EnriqueNo ratings yet
- What's New in The SICU: Douglas JE Schuerer, MD FACS Director of TraumaDocument54 pagesWhat's New in The SICU: Douglas JE Schuerer, MD FACS Director of Traumacrt0518No ratings yet
- AKI and CRRT RelationDocument10 pagesAKI and CRRT RelationZainab MotiwalaNo ratings yet
- Principles and Pitfalls in Coronary Vasomotor Function TestingDocument26 pagesPrinciples and Pitfalls in Coronary Vasomotor Function TestingRamón López PalopNo ratings yet
- Graft Patency After Off-Pump Versus On-Pump Coronary Artery Surgery in High-Risk PatientsDocument8 pagesGraft Patency After Off-Pump Versus On-Pump Coronary Artery Surgery in High-Risk PatientsZul FikarNo ratings yet
- Onwudike 2020Document10 pagesOnwudike 2020Han's OfficialNo ratings yet
- Journal of Cardiothoracic SurgeryDocument9 pagesJournal of Cardiothoracic SurgeryThanh BinhNo ratings yet
- Colloids Vs CrytaloidsDocument12 pagesColloids Vs CrytaloidsalimustagialgiNo ratings yet
- What Is OpcabDocument17 pagesWhat Is OpcabGrace Marie Sanchez-AguilarNo ratings yet
- Ivs 459Document3 pagesIvs 459melon segerNo ratings yet
- Evaluation of Factors Affecting Liver Function Test in Patients Underwent Coronary Artery Bypass Graft SurgeryDocument7 pagesEvaluation of Factors Affecting Liver Function Test in Patients Underwent Coronary Artery Bypass Graft SurgeryajmrdNo ratings yet
- Lesion Manguio Rotador en AmDocument5 pagesLesion Manguio Rotador en AmRelviGuzmanApazaNo ratings yet
- Goyal Et Al-2015-Annals of NeurologyDocument7 pagesGoyal Et Al-2015-Annals of NeurologyWinda Wahyu IkaputriNo ratings yet
- Intravascular ShuntDocument33 pagesIntravascular ShuntNatalindah Jokiem Woecandra T. D.No ratings yet
- Sherif Mokhtar, MD: Professor of Cardiology, Professor of Critical Care Medicine Cairo UniversityDocument85 pagesSherif Mokhtar, MD: Professor of Cardiology, Professor of Critical Care Medicine Cairo UniversityShimmering MoonNo ratings yet
- ECG NotesDocument7 pagesECG NotesShams NabeelNo ratings yet
- 3 - Deteksi Dini CHF - 22.3.23Document53 pages3 - Deteksi Dini CHF - 22.3.23tioNo ratings yet
- Cor Radiology (Kuliah Cardiovascular) 2011Document51 pagesCor Radiology (Kuliah Cardiovascular) 2011athayafebNo ratings yet
- Mcqs Pediatric Cardiology EmergencyDocument29 pagesMcqs Pediatric Cardiology EmergencyOmed M. AhmedNo ratings yet
- SVT CaseDocument11 pagesSVT CaseZakiy AzzuhdiNo ratings yet
- Vereckei TVDocument12 pagesVereckei TVVallejo Romo Alberto CristianNo ratings yet
- ACLS Algorithms SlideDocument26 pagesACLS Algorithms SlidehrsoNo ratings yet
- Atrial FibrilationDocument27 pagesAtrial FibrilationemialevelaNo ratings yet
- OSCEs SyllabusDocument133 pagesOSCEs SyllabusAnusha VergheseNo ratings yet
- 1500 Ebook Clinical Medicine Up PDFDocument215 pages1500 Ebook Clinical Medicine Up PDFAhmad Arif100% (1)
- What Is ArrhythmiaDocument14 pagesWhat Is ArrhythmiaSharan MurugaboopathyNo ratings yet
- 2022.02.10 MCCQE Study Plan Canada 2Document52 pages2022.02.10 MCCQE Study Plan Canada 2joann15marrieNo ratings yet
- European Examination in General Cardiology (EEGC) : Jim Hall Celine CarreraDocument37 pagesEuropean Examination in General Cardiology (EEGC) : Jim Hall Celine CarreraTasya MDNo ratings yet
- Nadolol (RX) : Category: Beta-BlockersDocument6 pagesNadolol (RX) : Category: Beta-BlockersSerious BlackNo ratings yet
- Concept Map Tetralogy of FallotDocument2 pagesConcept Map Tetralogy of FallotKarl KiwisNo ratings yet
- Congenital Heart DefectsDocument13 pagesCongenital Heart DefectsGheluzee Herrera100% (2)
- Daftar Pustaka: Universitas Sumatera UtaraDocument2 pagesDaftar Pustaka: Universitas Sumatera UtaraNavisa HaifaNo ratings yet
- Syllab BSC RTDocument24 pagesSyllab BSC RTKiruba HaranNo ratings yet
- Rilantono, Lily L. 5 Rahasia Penyakit Kardiovaskular (PKV) - Jakarta: Badan Penerbit Fakultas Kedokteran Universitas Indonesia 2012. p.279-287Document1 pageRilantono, Lily L. 5 Rahasia Penyakit Kardiovaskular (PKV) - Jakarta: Badan Penerbit Fakultas Kedokteran Universitas Indonesia 2012. p.279-287Tegar DharmaNo ratings yet
- VT Origin PDFDocument60 pagesVT Origin PDFNikita PratamaNo ratings yet
- Azure™ XT DR MRI SureScan™ W2DR01Document44 pagesAzure™ XT DR MRI SureScan™ W2DR01mytake100No ratings yet
- Pharmacology Review Questions For QuizDocument14 pagesPharmacology Review Questions For QuizusedforfunplocNo ratings yet
- Cir 0000000000001054Document16 pagesCir 0000000000001054Code ValmirNo ratings yet
- Cath Lab ReportDocument13 pagesCath Lab ReportNasim AhmadNo ratings yet
- Nej M Abbotts TentDocument11 pagesNej M Abbotts TentWKYC.comNo ratings yet
- Cardiovascular ExaminationDocument4 pagesCardiovascular ExaminationarchanaNo ratings yet