Download as pptx, pdf, or txt
You might also like
- Bisb - Bank StatementDocument23 pagesBisb - Bank Statementazstartup.bhNo ratings yet
- SM CH PDFDocument18 pagesSM CH PDFHector NaranjoNo ratings yet
- Chemical Hardness Ralph G. PearsonDocument208 pagesChemical Hardness Ralph G. PearsonVasu NagpalNo ratings yet
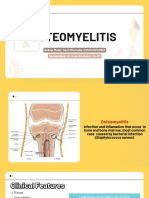
- 6 OsteomyelitisDocument29 pages6 OsteomyelitisMohammed AshrefNo ratings yet
- Disorders of Bone II-2Document59 pagesDisorders of Bone II-2Guhan DergNo ratings yet
- Osteomyelitisofjaw 131117034448 Phpapp02Document35 pagesOsteomyelitisofjaw 131117034448 Phpapp02D YasIr MussaNo ratings yet
- 5 Inflammation of Bone NewDocument15 pages5 Inflammation of Bone Newnightfury200313No ratings yet
- OsteomyelitisofjawDocument35 pagesOsteomyelitisofjawOded KantzukerNo ratings yet
- 7 OsteomyelitisDocument3 pages7 Osteomyelitisameeraligadhban03No ratings yet
- Inflammatory Lesions of The JAW: Bhavika Pol Vhatkar 1 Yr PGDocument132 pagesInflammatory Lesions of The JAW: Bhavika Pol Vhatkar 1 Yr PGArpita SankhwarNo ratings yet
- Inflammatory Diseases of BoneDocument20 pagesInflammatory Diseases of BonesiaNo ratings yet
- Pathology of Bone and Soft Tissue-LectureDocument52 pagesPathology of Bone and Soft Tissue-Lecturejohnwickshopping79No ratings yet
- Inflammatory Disorder of BoneDocument13 pagesInflammatory Disorder of Bonedentist07801644159No ratings yet
- Xray of Bones in OsteomyelitisDocument35 pagesXray of Bones in OsteomyelitisBukola AjokeNo ratings yet
- OsteomylitisDocument48 pagesOsteomylitissamar yousif mohamed100% (1)
- OSTEOMYELITISDocument5 pagesOSTEOMYELITISArafat Masud Niloy100% (1)
- Inflammatory Disease of BonesDocument93 pagesInflammatory Disease of BonesNelson LagatNo ratings yet
- Osteomyelitis: Oral Pathology 4 Stage DR - Hemn M.Sharif (B.D.S, MSC, O.Medicine) 2-4-2020Document18 pagesOsteomyelitis: Oral Pathology 4 Stage DR - Hemn M.Sharif (B.D.S, MSC, O.Medicine) 2-4-2020محمد عبدالهادي إسماعيلNo ratings yet
- Remota 170426124830Document34 pagesRemota 170426124830Lolo TotoNo ratings yet
- Osteomyelitis of The JawsDocument73 pagesOsteomyelitis of The JawsArshu Shaik812No ratings yet
- Bone Infections For PMDocument31 pagesBone Infections For PM202201666No ratings yet
- Bone InfectionsDocument22 pagesBone InfectionsOmar MustafaNo ratings yet
- Osteomyelitis "Is Often More Than Simply The Presence of Organisms in The Skeleton and Often Less Than Pain, Swelling, and Drainage.'Document75 pagesOsteomyelitis "Is Often More Than Simply The Presence of Organisms in The Skeleton and Often Less Than Pain, Swelling, and Drainage.'JayeshNo ratings yet
- Osteomyelitis: ClassificationDocument5 pagesOsteomyelitis: Classificationthanuja mathewNo ratings yet
- OsteomyelitisDocument147 pagesOsteomyelitisAnkit Agur100% (1)
- OsteomyelitisDocument17 pagesOsteomyelitisBindu BinduNo ratings yet
- Pulp and Periapical TissuesDocument2 pagesPulp and Periapical TissuesBhaveshNo ratings yet
- OsteomyelitisDocument10 pagesOsteomyelitismustafaNo ratings yet
- 34 W11 OsteomylitisDocument32 pages34 W11 OsteomylitisAbdulelah MurshidNo ratings yet
- Plain X Rays of BonesDocument17 pagesPlain X Rays of BonesEmmanuella NoelNo ratings yet
- Specific Infections 7.1. OsteomyelitisDocument2 pagesSpecific Infections 7.1. OsteomyelitisTitis Mustika HandayaniNo ratings yet
- Osteomyelitis 130708212636 Phpapp01Document107 pagesOsteomyelitis 130708212636 Phpapp01merikasorNo ratings yet
- 2 5420394524511833795 PDFDocument232 pages2 5420394524511833795 PDFعبدالرحمن عبدالسلام ذنون المصريNo ratings yet
- Osteomyelitis of The JawsDocument70 pagesOsteomyelitis of The JawsMONIKANo ratings yet
- OsteomyelitisDocument41 pagesOsteomyelitisArumpaavai PugazhiniNo ratings yet
- OsteomyelitisDocument15 pagesOsteomyelitis2018B-04Desti RhomaliaNo ratings yet
- Oral Surgery4 Lec.16 OsteomyelitisDocument23 pagesOral Surgery4 Lec.16 OsteomyelitisSRO oONo ratings yet
- Chronic OsteomylitisqDocument5 pagesChronic Osteomylitisqdrahmed1028No ratings yet
- Infection of The JawDocument51 pagesInfection of The JawMutia Safitri0% (1)
- Curs 9 Imagistica MSKDocument62 pagesCurs 9 Imagistica MSKn bNo ratings yet
- OsteomyelitisDocument32 pagesOsteomyelitisyogeshNo ratings yet
- Osteomyelitis PathoDocument1 pageOsteomyelitis PathoSheng Tingson PacitNo ratings yet
- Presentation 1Document120 pagesPresentation 1Khurram ChauhanNo ratings yet
- Osteomyelitis of Jaws: Presented By: Anuradha B.D.S Final YearDocument11 pagesOsteomyelitis of Jaws: Presented By: Anuradha B.D.S Final YearGujjar VishalNo ratings yet
- Due To The Sharp Bending of The Vessels in The Metaphysic and Also by The Hematoma Formed After InjuryDocument6 pagesDue To The Sharp Bending of The Vessels in The Metaphysic and Also by The Hematoma Formed After InjuryBashar EbrahimNo ratings yet
- OsteomyelitisDocument35 pagesOsteomyelitischinnnababu100% (1)
- Askep OsteomielitisDocument13 pagesAskep Osteomielitisuciha_herhyNo ratings yet
- OSTEOMYELITISDocument4 pagesOSTEOMYELITISGanah PeterNo ratings yet
- Special Lecture 5Document10 pagesSpecial Lecture 5HussainNo ratings yet
- Chronic Osteomyelitis: Dr. F. Abdul Khader Professor & HOD Department of Orthopaedics SSSMC & RiDocument31 pagesChronic Osteomyelitis: Dr. F. Abdul Khader Professor & HOD Department of Orthopaedics SSSMC & RiDr. F. Abdul KhaderNo ratings yet
- Patho (Osteomyelitis)Document2 pagesPatho (Osteomyelitis)sidaveNo ratings yet
- Osteomyelitis: Dr. Dewi Klarita Furtuna, M.Ked - Klin., SP - MKDocument49 pagesOsteomyelitis: Dr. Dewi Klarita Furtuna, M.Ked - Klin., SP - MKStefNo ratings yet
- Musculoskeletal Infection: Nor Aida, Jessica, Nivasini, Sarah, SyarifahDocument87 pagesMusculoskeletal Infection: Nor Aida, Jessica, Nivasini, Sarah, SyarifahShalltear BloodfallenNo ratings yet
- Definition of OsteomyelitisDocument3 pagesDefinition of OsteomyelitisRey Gabriel Advincula GranadaNo ratings yet
- Wa0006.Document14 pagesWa0006.mldmddhNo ratings yet
- Osteomyelitis: Deo Jake Lacpacan Jhunevyl MallorcaDocument36 pagesOsteomyelitis: Deo Jake Lacpacan Jhunevyl MallorcaDeo Jake Lacpacan100% (1)
- Differential Diagnosis of Chronic OsteomyelitisDocument55 pagesDifferential Diagnosis of Chronic OsteomyelitisahmedNo ratings yet
- Asuhan Keperawatan Pada Klien Dengan Osteomyelitis: Oleh Ira Suarilah Dept - Kep.Medikal-Bedah Psik-Fk UnairDocument13 pagesAsuhan Keperawatan Pada Klien Dengan Osteomyelitis: Oleh Ira Suarilah Dept - Kep.Medikal-Bedah Psik-Fk UnairNikmaNo ratings yet
- OsteomyelitisDocument8 pagesOsteomyelitisyogeshNo ratings yet
- Sheet 4 (Bone Pathology)Document206 pagesSheet 4 (Bone Pathology)ardesh abdille0% (1)
- Compare Pyogenic and Tuberculous OsteomyelitisDocument3 pagesCompare Pyogenic and Tuberculous OsteomyelitisMOHAMED AMINNo ratings yet
- Bone Infection, (Osteomyelitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandBone Infection, (Osteomyelitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Analysis and Classification of Milk Qualityusingelectronicsensoryorgans-Mba-2017Document91 pagesAnalysis and Classification of Milk Qualityusingelectronicsensoryorgans-Mba-2017ziza20 ZizaNo ratings yet
- 580M Series 2 Hydraulics 4 PDFDocument3 pages580M Series 2 Hydraulics 4 PDFJESUSNo ratings yet
- MLAJ185-01 Advanced Java Programming Learning Manual - V1.0 April 2018 PDFDocument317 pagesMLAJ185-01 Advanced Java Programming Learning Manual - V1.0 April 2018 PDFmichaelNo ratings yet
- Tilt TableDocument2 pagesTilt TablenikhilNo ratings yet
- Research Process - StepsDocument31 pagesResearch Process - StepsPulkit SharmaNo ratings yet
- Islamic Architecture PDFDocument32 pagesIslamic Architecture PDFCamille CiokonNo ratings yet
- Essential Orthopaedics 2Nd Edition Mark D Miller Full ChapterDocument67 pagesEssential Orthopaedics 2Nd Edition Mark D Miller Full Chaptermargaret.jones429100% (8)
- Module in STSDocument5 pagesModule in STSAbriann Vince ImpenioNo ratings yet
- Abortion - A Philosophical Perspective: OpsommingDocument7 pagesAbortion - A Philosophical Perspective: OpsommingGeorge RaresNo ratings yet
- 85.deep Seabed Mining (12-2013)Document4 pages85.deep Seabed Mining (12-2013)RSTNo ratings yet
- PHD Syllabus AMUDocument2 pagesPHD Syllabus AMUMohd ShahidNo ratings yet
- 1LOC005 - How Do I Allocate Legs To A Drivers Run SheetDocument2 pages1LOC005 - How Do I Allocate Legs To A Drivers Run Sheetguolidong2017No ratings yet
- CDC Birth Control ChartDocument2 pagesCDC Birth Control ChartCaitlin StrohlNo ratings yet
- Microprocessor - 8086 Addressing ModesDocument3 pagesMicroprocessor - 8086 Addressing ModesGaganBhayanaNo ratings yet
- Error-Free - An Analysis of Art For Heart's Sake by Rube GoldbergDocument3 pagesError-Free - An Analysis of Art For Heart's Sake by Rube Goldbergwad elshaikhNo ratings yet
- Jurassic Production Facility (JPF) at Sabriya: Supplier Document Cover SheetDocument2 pagesJurassic Production Facility (JPF) at Sabriya: Supplier Document Cover SheetBiswasNo ratings yet
- Apply For Car Loan in Canada From Canadian Auto CenterDocument1 pageApply For Car Loan in Canada From Canadian Auto CenterCanadian Auto CenterNo ratings yet
- Crash Course: QM MathDocument6 pagesCrash Course: QM MathJosé Luis Salazar EspitiaNo ratings yet
- Proposed Syllabus: University of North BengalDocument53 pagesProposed Syllabus: University of North BengalDebolina BhattacharyaNo ratings yet
- JTG D20-2006 EngDocument113 pagesJTG D20-2006 EngchikwawaNo ratings yet
- Solution Manual For Operations and Supply Chain Management For The 21st Century 1st Edition by BoyerDocument7 pagesSolution Manual For Operations and Supply Chain Management For The 21st Century 1st Edition by Boyergowdie.mornward.b50a100% (55)
- Warhammer 40k Epic Scenarios MoonlightDocument28 pagesWarhammer 40k Epic Scenarios Moonlightdallin AndersonNo ratings yet
- FM-HS-240-01.7 Full Mob For Use Rev4Document5 pagesFM-HS-240-01.7 Full Mob For Use Rev4VZNo ratings yet
- 3-MIDA Investment Opportunities in GT IndustryDocument40 pages3-MIDA Investment Opportunities in GT IndustryWong Yong Sheng WongNo ratings yet
- TCCC Handbook Fall 2013Document192 pagesTCCC Handbook Fall 2013AMG_IA100% (4)
- Chapter 4-The Life of Jose RizalDocument3 pagesChapter 4-The Life of Jose RizalArmilah Sultan Masaranga100% (1)
- Science Internet ResourcesDocument4 pagesScience Internet ResourcesGabriela D CostescuNo ratings yet