Download as ppt, pdf, or txt
You might also like
- Cleft Lip and Cleft PalateDocument6 pagesCleft Lip and Cleft PalatekrishnasreeNo ratings yet
- Design of Air Conditioning and Ventilation System For A Multi Storey Office BuildingDocument5 pagesDesign of Air Conditioning and Ventilation System For A Multi Storey Office BuildingIppiNo ratings yet
- Loreal IndiaDocument36 pagesLoreal IndiaDeepakNo ratings yet
- Nursing Care of The Child Born With PhysicalDocument55 pagesNursing Care of The Child Born With PhysicalJoy kimmNo ratings yet
- Maternal First Quiz ReviewerDocument15 pagesMaternal First Quiz ReviewerRay Ann BorresNo ratings yet
- Cleft Palate and Cleft Lip IntroductionDocument3 pagesCleft Palate and Cleft Lip IntroductionCLaui SagibalNo ratings yet
- Physical and Developmental Disorders of The Gastrointestinal SystemDocument10 pagesPhysical and Developmental Disorders of The Gastrointestinal SystemJo Marchianne PigarNo ratings yet
- Content Congenital DisorderDocument20 pagesContent Congenital DisorderKaka SalvatoreNo ratings yet
- Cleft Lip and Cleft PalateDocument4 pagesCleft Lip and Cleft PalateJulliza Joy PandiNo ratings yet
- Cleft Lip and PalateDocument20 pagesCleft Lip and Palatejapzee1988100% (1)
- Cleft Lip PalateDocument29 pagesCleft Lip PalatelisalovNo ratings yet
- PalatoschisisDocument4 pagesPalatoschisisInge Sandrie PhutriNo ratings yet
- Chrisanthopoulos Marika 300453 Cleft Lip and PalateDocument14 pagesChrisanthopoulos Marika 300453 Cleft Lip and PalateCharles IppolitoNo ratings yet
- The Child W/ Alterations in Nutrition/Metabolism: Report By: Anita P. Prieto & Sugar Lynn M. CafirmaDocument6 pagesThe Child W/ Alterations in Nutrition/Metabolism: Report By: Anita P. Prieto & Sugar Lynn M. CafirmaAnita PrietoNo ratings yet
- Cleft Palate and LipsDocument5 pagesCleft Palate and LipsAn NukmanNo ratings yet
- Cleft and Lip PalateDocument6 pagesCleft and Lip PalateShane PangilinanNo ratings yet
- Cleft Lip or Cleft PalateDocument2 pagesCleft Lip or Cleft PalateKueenmae Unza SolivenNo ratings yet
- Cleft Lip & PalateDocument9 pagesCleft Lip & PalateJahzel CallinoNo ratings yet
- Cleft Lip and Cleft PalateDocument8 pagesCleft Lip and Cleft PalateRAJU33% (3)
- Cleft Lip Pregnancy BabyDocument2 pagesCleft Lip Pregnancy BabySamrah ManibpelNo ratings yet
- 2 - Congenital Defects - AboDocument47 pages2 - Congenital Defects - Abomarymahmoud73737No ratings yet
- Types of Cleft Palate Surgeries and Side EffectsDocument91 pagesTypes of Cleft Palate Surgeries and Side Effectsahmad shaddadNo ratings yet
- Cleft Lip and Cleft PalateDocument16 pagesCleft Lip and Cleft PalateIsmail LubisNo ratings yet
- Cleft Lip and Cleft PalateDocument27 pagesCleft Lip and Cleft Palatenamah odatNo ratings yet
- About Oral Clefting: Birth DefectsDocument7 pagesAbout Oral Clefting: Birth DefectsWilly TenjayaNo ratings yet
- 6 Cleft Palate Cleft LipDocument2 pages6 Cleft Palate Cleft LipLidya DiandraNo ratings yet
- EJMCM - Volume 7 - Issue 10 - Pages 470-474Document5 pagesEJMCM - Volume 7 - Issue 10 - Pages 470-474Ayu Nur FadilahNo ratings yet
- Cleft LipDocument5 pagesCleft LipGrazieNo ratings yet
- Cleft Lip and PalateDocument19 pagesCleft Lip and PalateJuviely PremacioNo ratings yet
- Cleft Lip and Cleft Palate: College of Health Science Department of Midwifery Course Newborn Care For PostbasicDocument42 pagesCleft Lip and Cleft Palate: College of Health Science Department of Midwifery Course Newborn Care For PostbasicmichaelNo ratings yet
- Cleft Lip and Cleft PalateDocument22 pagesCleft Lip and Cleft PalateSelvester GeorgeNo ratings yet
- Cleft Lip BrochureDocument15 pagesCleft Lip BrochureValentina Cerón ZúñigaNo ratings yet
- Congenital Anomalies in Newborn (Critical)Document46 pagesCongenital Anomalies in Newborn (Critical)Shereen Mohamed Soliman HammoudaNo ratings yet
- Lesson 16Document20 pagesLesson 16Twinamasiko DanielNo ratings yet
- GASTROINTESTINAL DISORDERS Cleft Palate - Esophageal Atresia - Oral MoniliasisDocument7 pagesGASTROINTESTINAL DISORDERS Cleft Palate - Esophageal Atresia - Oral MoniliasisMikasa AckermanNo ratings yet
- About Cleft Lip and Palate: FeedingDocument3 pagesAbout Cleft Lip and Palate: FeedingnarutomovieNo ratings yet
- Cleft Lip and Cleft PalateDocument22 pagesCleft Lip and Cleft PalateOm VaishNav0% (1)
- Cleft Palate (DeGuzman)Document16 pagesCleft Palate (DeGuzman)JhayneNo ratings yet
- Cleft Lip Cleft Palate: Presented By: Ivan AvenadoDocument16 pagesCleft Lip Cleft Palate: Presented By: Ivan AvenadoIvan Liquiran AvenadoNo ratings yet
- Cleft Lip PalateDocument4 pagesCleft Lip PalateMaricel DefiestaNo ratings yet
- Cleft Palate Pregnancy Mouth: Slideshow: Migraine Dos and Don'tsDocument6 pagesCleft Palate Pregnancy Mouth: Slideshow: Migraine Dos and Don'tsBenedictus HanjayaNo ratings yet
- Baba Jaswant Singh Dental College and Research Institute, LudhianaDocument40 pagesBaba Jaswant Singh Dental College and Research Institute, LudhianaPalak VashistNo ratings yet
- Cleft Lip and PalateDocument25 pagesCleft Lip and PalateRahul Dhaker100% (1)
- Syndrome Cleft Lip and PalateDocument8 pagesSyndrome Cleft Lip and PalateValentina Lakhsmi PrabandariNo ratings yet
- Labioschizis Dan Palatoskisis Persentasi Kelompok 1Document17 pagesLabioschizis Dan Palatoskisis Persentasi Kelompok 1Hengky HanggaraNo ratings yet
- Cleft Lip and Cleft PalateDocument16 pagesCleft Lip and Cleft Palatemacuka08100% (3)
- NRS210 Stu01Document26 pagesNRS210 Stu01Rohit TheteNo ratings yet
- Mal RotationDocument13 pagesMal RotationkavyarkrnagarNo ratings yet
- Cleft Lip and PalateDocument4 pagesCleft Lip and PalateAyah HyasatNo ratings yet
- Cleft Lip and Cleft PalateDocument6 pagesCleft Lip and Cleft PalateRiza Angela BarazanNo ratings yet
- Cleft Lip & Cleft Palate: Presentor Ms. Jeewan JyotiDocument25 pagesCleft Lip & Cleft Palate: Presentor Ms. Jeewan JyotiHamss AhmedNo ratings yet
- Bad HabitsDocument7 pagesBad HabitsAnonymous itwv6oMNo ratings yet
- Cleft Lip and Palate NewDocument7 pagesCleft Lip and Palate NewUday Kumar0% (1)
- Cleft Lip and PalateDocument18 pagesCleft Lip and Palateicywitch100% (1)
- Health Brochure Comprehensive OverviewDocument12 pagesHealth Brochure Comprehensive Overviewعبدالرحمن سالم بن مخاشنNo ratings yet
- Child With Cleft To Lips and A Cleft PalateDocument9 pagesChild With Cleft To Lips and A Cleft PalateWeji ShNo ratings yet
- Chapter 13 Cleft Palate PDFDocument21 pagesChapter 13 Cleft Palate PDFmitasarisukadanaNo ratings yet
- Cleft Lip And Palate, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCleft Lip And Palate, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 4.5 out of 5 stars4.5/5 (3)
- Guidotti Timothy E1980Document164 pagesGuidotti Timothy E1980Samuel GarciaNo ratings yet
- The Incredible Analysis of W D GannDocument79 pagesThe Incredible Analysis of W D GannJohn Kent97% (31)
- APA PDS Supplement 1-90 Design and Fabrication of Plywood CurvedDocument24 pagesAPA PDS Supplement 1-90 Design and Fabrication of Plywood CurvedVinícius Da Cunha FerreiraNo ratings yet
- Group 3Document59 pagesGroup 3Grey Sinclair100% (1)
- Computer Vision Module 5Document22 pagesComputer Vision Module 5lukerichman29100% (1)
- SpeechDocument5 pagesSpeechNiza Pinky IchiyuNo ratings yet
- 04353957Document5 pages04353957Ramya RNo ratings yet
- Audio 4 - 1 Travelling 1Document15 pagesAudio 4 - 1 Travelling 1Farewell03311No ratings yet
- LevellingDocument11 pagesLevellingetikaf50% (2)
- Neverwhere by Neil Gaiman - Teacher Study GuideDocument3 pagesNeverwhere by Neil Gaiman - Teacher Study GuideHarperAcademic33% (3)
- TesisDocument78 pagesTesisWidya SariNo ratings yet
- PT English-6 Q2Document7 pagesPT English-6 Q2Elona Jane CapangpanganNo ratings yet
- Astro-Logics Pub PDFDocument7 pagesAstro-Logics Pub PDFlbedar100% (1)
- Thermotherapy PDFDocument51 pagesThermotherapy PDFRUdraNo ratings yet
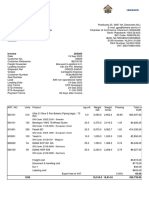
- Invoice 203265: GN Code: 3923.2100 - SwedenDocument2 pagesInvoice 203265: GN Code: 3923.2100 - SwedenArturo RiveroNo ratings yet
- Maya, Aztec, and Inca Civilizations PDFDocument116 pagesMaya, Aztec, and Inca Civilizations PDFGabriel Medina100% (2)
- Marketing Management Project: Submitted byDocument41 pagesMarketing Management Project: Submitted byrpotnisNo ratings yet
- 3storeyresidence Final ModelDocument1 page3storeyresidence Final ModelRheafel LimNo ratings yet
- Azolla: A Review of Its Biology and UtilizationDocument6 pagesAzolla: A Review of Its Biology and UtilizationAaron PabionaNo ratings yet
- Allison Taylor Dissertation Heinrich SchliemannDocument6 pagesAllison Taylor Dissertation Heinrich SchliemannPaperWritingServiceSuperiorpapersSpringfield100% (1)
- Transducers & Isolators: TR - IsoDocument1 pageTransducers & Isolators: TR - IsoManikandan B100% (1)
- FFS PINNSEF 30 November 2020Document1 pageFFS PINNSEF 30 November 2020teguhsunyotoNo ratings yet
- Organised By: Dr. Poonam S. TiwariDocument2 pagesOrganised By: Dr. Poonam S. Tiwarisayed kundumon100% (1)
- Allen StoneDocument4 pagesAllen StoneRubén FernándezNo ratings yet
- Boli Interne Vol I Partea 1Document454 pagesBoli Interne Vol I Partea 1Murariu Diana100% (2)
- Jouney To Becoming A Surface Pattern DesignerDocument16 pagesJouney To Becoming A Surface Pattern Designerwhere is my mindNo ratings yet
- Readme CCRDocument51 pagesReadme CCRSesha SuryaNo ratings yet
- Claims and Counter ClaimsDocument13 pagesClaims and Counter ClaimsRk VaitlaNo ratings yet