Download as pptx, pdf, or txt
You might also like
- Practical Medical Oncology Textbook (Antonio Russo, Marc Peeters, Lorena Incorvaia Etc.)Document1,104 pagesPractical Medical Oncology Textbook (Antonio Russo, Marc Peeters, Lorena Incorvaia Etc.)Paolo FassinaNo ratings yet
- SOGP AnaemiaDocument16 pagesSOGP AnaemiaMuhammad Farrukh ul IslamNo ratings yet
- Sat-600hp Service Manual1223Document50 pagesSat-600hp Service Manual1223FuadNo ratings yet
- Getinge Autoclave Service Manual Green FilmDocument5 pagesGetinge Autoclave Service Manual Green FilmFuadNo ratings yet
- MOSFET Cross-Reference Search - Equivalent TransistorsDocument1 pageMOSFET Cross-Reference Search - Equivalent TransistorsFuadNo ratings yet
- Dell Optiplex Computers Repair ManualDocument5 pagesDell Optiplex Computers Repair ManualFuad0% (1)
- Of Periodontal & Peri-Implant Diseases: ClassificationDocument24 pagesOf Periodontal & Peri-Implant Diseases: ClassificationruchaNo ratings yet
- Government College of Nursing: JodhpurDocument9 pagesGovernment College of Nursing: JodhpurpriyankaNo ratings yet
- Nutritional Anemia: Dr. Mardiana, M.Kes, SP - GK Department of Clinical Nutrition Hasanuddin University MakassarDocument77 pagesNutritional Anemia: Dr. Mardiana, M.Kes, SP - GK Department of Clinical Nutrition Hasanuddin University MakassarDianaNo ratings yet
- Clinical Update AnemiaDocument4 pagesClinical Update AnemiaAnisah TifaniNo ratings yet
- Nutritional AnemiaDocument78 pagesNutritional AnemiaJoUng DjelauNo ratings yet
- Anemia GiziDocument47 pagesAnemia Giziadink mochammadNo ratings yet
- Anemia in Pregnancy2024Document24 pagesAnemia in Pregnancy2024akankiza.lucky83No ratings yet
- Anemia During PregnancyDocument15 pagesAnemia During PregnancyKuleshwar SahuNo ratings yet
- RITADocument54 pagesRITAFobie Kate CarinoNo ratings yet
- Dr. Ramya Moderator: DR - PallaveeDocument71 pagesDr. Ramya Moderator: DR - PallaveeMonika shankarNo ratings yet
- Iron Deficiency Anemia: Iron Transport in The PlasmaDocument13 pagesIron Deficiency Anemia: Iron Transport in The PlasmaarbazNo ratings yet
- Anemia Gizi: Agussalim Bukhari Bagian Ilmu Gizi Fak - Kedokteran UnhasDocument47 pagesAnemia Gizi: Agussalim Bukhari Bagian Ilmu Gizi Fak - Kedokteran UnhasPratiwi Dwi LestariNo ratings yet
- Buy The Book PDA Download: Update MeDocument12 pagesBuy The Book PDA Download: Update MeyanajaeNo ratings yet
- Anaemia in Pregnancy: Definition and IncidenceDocument14 pagesAnaemia in Pregnancy: Definition and IncidencejNo ratings yet
- Anaemia in PregnancyDocument29 pagesAnaemia in PregnancyDavina DakapNo ratings yet
- O&G - Article - Anaemia in Pregnancy (GLOWM)Document6 pagesO&G - Article - Anaemia in Pregnancy (GLOWM)Leroy LoyNo ratings yet
- Anemia in PregnancyDocument20 pagesAnemia in PregnancyMargaretha UsbokoNo ratings yet
- Anemia in PregnancyDocument7 pagesAnemia in PregnancyLenrok AdrianNo ratings yet
- Anaemia in PregnancyDocument35 pagesAnaemia in PregnancyUmar Dhani89% (9)
- Diet Pada Anemia, Kva, GakiDocument39 pagesDiet Pada Anemia, Kva, GakiYanuarti PetrikaNo ratings yet
- HematinicsDocument27 pagesHematinicsDeepankar SutradharNo ratings yet
- Disampaikan Oleh: Dr. Ong Tjandra, MMPD., Spog (K)Document46 pagesDisampaikan Oleh: Dr. Ong Tjandra, MMPD., Spog (K)Asis muhammadNo ratings yet
- During PregnancyDocument31 pagesDuring PregnancyMotaz AliNo ratings yet
- Final AnemiaDocument23 pagesFinal Anemiaat0420529No ratings yet
- Obg 2Document150 pagesObg 2PrathibhaNo ratings yet
- AnemiaDocument57 pagesAnemiaSandhya BasnetNo ratings yet
- Anemia PregnancyمحاضرةDocument33 pagesAnemia PregnancyمحاضرةSamia Abu AishiaNo ratings yet
- Diet Pada Anemia, Kva, GakiDocument39 pagesDiet Pada Anemia, Kva, GakiYanuarti PetrikaNo ratings yet
- AnemiaDocument71 pagesAnemiaAnsu MaliyakalNo ratings yet
- Megaloblastic AnemiaDocument26 pagesMegaloblastic AnemiaAbdifatah Abdiwali mohamedNo ratings yet
- #3 - NCM 109 - TransesDocument8 pages#3 - NCM 109 - TransesJaimie BanaagNo ratings yet
- Medico Study Join Our Telegram Channel @medicostudyDocument5 pagesMedico Study Join Our Telegram Channel @medicostudyKirubel DeribNo ratings yet
- Dr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik UnjaDocument18 pagesDr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik Unjariska yulizaNo ratings yet
- Anemia PregnancyDocument44 pagesAnemia Pregnancykhadzx100% (3)
- AnemiaDocument11 pagesAnemiadewiq_wahyuNo ratings yet
- Anaemia in PregnancyDocument31 pagesAnaemia in PregnancyheatherNo ratings yet
- Anemia IN Pregnancy: Prepared By: Aashma Bidari M.Sc. Nursing 1 Year 4 Batch, KUSMSDocument53 pagesAnemia IN Pregnancy: Prepared By: Aashma Bidari M.Sc. Nursing 1 Year 4 Batch, KUSMSAasma Bidari100% (1)
- Anemia and Pregnancy: Sunil Kumar DahaDocument43 pagesAnemia and Pregnancy: Sunil Kumar DahaBhawna JoshiNo ratings yet
- Pregnancy With PallorDocument31 pagesPregnancy With PallorshoaibakhtardgkNo ratings yet
- Anemia in PregnancyDocument33 pagesAnemia in PregnancyKomal Dhulap100% (1)
- Iron Deficiency AnemiaDocument17 pagesIron Deficiency Anemiaمصطفى عبد الرزاق ورد حسينNo ratings yet
- Case 21Document14 pagesCase 21rawan.5alilNo ratings yet
- Government College of Nursing Jodhpur: Presentation On Anemia and Nutritional DeficiencyDocument7 pagesGovernment College of Nursing Jodhpur: Presentation On Anemia and Nutritional Deficiencypriyanka100% (2)
- Dr. Waled Abohatab Turkish Board MD Nasser Medical ComplexDocument19 pagesDr. Waled Abohatab Turkish Board MD Nasser Medical ComplexArwa QishtaNo ratings yet
- AnaemiaDocument66 pagesAnaemiaSusmita DasNo ratings yet
- MBBS-4 No014090Document43 pagesMBBS-4 No014090diphylleia90grayiNo ratings yet
- Anemia: Hussein Hallak, PH.DDocument19 pagesAnemia: Hussein Hallak, PH.DIbrahim BarhamNo ratings yet
- Anemia Defisiensi Pada KehamilanDocument23 pagesAnemia Defisiensi Pada KehamilanAmri AshshiddieqNo ratings yet
- Nutritional Therapy For Deficiency AnemiasDocument49 pagesNutritional Therapy For Deficiency AnemiasKartikaPANo ratings yet
- archivetempPharmEducate Blood and NutritionDocument29 pagesarchivetempPharmEducate Blood and NutritionAyeshaNo ratings yet
- Anaemia in Pregnancy-MaklapDocument34 pagesAnaemia in Pregnancy-MaklapBronson KaturkanaNo ratings yet
- Etiology: There Are 3 Main Causes: 1-Erythrocyte Production: (Hypo Proliferative Anemia)Document28 pagesEtiology: There Are 3 Main Causes: 1-Erythrocyte Production: (Hypo Proliferative Anemia)heatherNo ratings yet
- SIM - Anemias of PregnancyDocument17 pagesSIM - Anemias of PregnancyGabrielle EvangelistaNo ratings yet
- Nutritional AnemiaDocument90 pagesNutritional AnemiaIrham KhairiNo ratings yet
- انيماDocument59 pagesانيمااحمد احمدNo ratings yet
- Anaemia in PregnancyDocument36 pagesAnaemia in PregnancyParvathy R NairNo ratings yet
- Hypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- A Simple Guide to Vitamin B12 Anemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Vitamin B12 Anemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- A Simple Guide to Anemia, Treatment and Related DiseasesFrom EverandA Simple Guide to Anemia, Treatment and Related DiseasesRating: 4.5 out of 5 stars4.5/5 (2)
- Spare PartDocument3 pagesSpare PartFuadNo ratings yet
- Water Utility BillDocument1 pageWater Utility BillFuadNo ratings yet
- 1 Statistical Methods For Continuous Variables Corr and RegressionDocument75 pages1 Statistical Methods For Continuous Variables Corr and RegressionFuad100% (1)
- Zones of Protection and General Principles of ProtectionDocument5 pagesZones of Protection and General Principles of ProtectionFuadNo ratings yet
- ALX Application Founder Transcript.Document2 pagesALX Application Founder Transcript.FuadNo ratings yet
- Chapter 11: Reagent Manufacture: Guidelines For The Blood Transfusion ServicesDocument33 pagesChapter 11: Reagent Manufacture: Guidelines For The Blood Transfusion ServicesFuadNo ratings yet
- Certificate Course On Instruments Maintenance For TechniciansDocument3 pagesCertificate Course On Instruments Maintenance For TechniciansFuadNo ratings yet
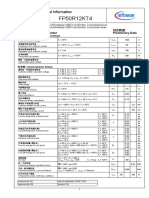
- Fp50R12Kt4: 技术信息/TechnicalinformationDocument11 pagesFp50R12Kt4: 技术信息/TechnicalinformationFuadNo ratings yet
- Online Course On Ophthalmic Instruments Maintenance - Part IDocument2 pagesOnline Course On Ophthalmic Instruments Maintenance - Part IFuadNo ratings yet
- Infineon-EconoPACK - EconoPIM - Series - ApplicationNotes-v01 - 00-ENDocument27 pagesInfineon-EconoPACK - EconoPIM - Series - ApplicationNotes-v01 - 00-ENFuadNo ratings yet
- Service Manual: H.C.P.T. APR'07Document11 pagesService Manual: H.C.P.T. APR'07FuadNo ratings yet
- Prepared By: Someone Like John CrixusDocument67 pagesPrepared By: Someone Like John CrixusFuadNo ratings yet
- Hand Wheel Vertical Autoclave Biobase BKQ-B75IIDocument3 pagesHand Wheel Vertical Autoclave Biobase BKQ-B75IIFuadNo ratings yet
- 45 - 70685 - EE412 - 2012 - 1 - 1 - 1 - Control System II-1Document24 pages45 - 70685 - EE412 - 2012 - 1 - 1 - 1 - Control System II-1FuadNo ratings yet
- 1SDC210107D0201 - Embedded ATSDocument4 pages1SDC210107D0201 - Embedded ATSFuadNo ratings yet
- Hitachi R-Z570ARU7 Service ManualDocument11 pagesHitachi R-Z570ARU7 Service ManualFuadNo ratings yet
- ABB ATS Brochure V 10-2 LRDocument12 pagesABB ATS Brochure V 10-2 LRFuadNo ratings yet
- Postcodes in Ethiopia: Listed in Postcode Order From 1000 To 7260Document5 pagesPostcodes in Ethiopia: Listed in Postcode Order From 1000 To 7260FuadNo ratings yet
- V23990-P849 - 4 - PM: Flow PIM 0 3Document24 pagesV23990-P849 - 4 - PM: Flow PIM 0 3FuadNo ratings yet
- Finecare BrochureDocument2 pagesFinecare BrochureFuadNo ratings yet
- GN Series: Product SelectionDocument182 pagesGN Series: Product SelectionFuadNo ratings yet
- Tn0200T/Ts N-Channel 20-V (D-S) Mosfets: Vishay SiliconixDocument5 pagesTn0200T/Ts N-Channel 20-V (D-S) Mosfets: Vishay SiliconixFuadNo ratings yet
- 1.pulse Oximeter: General Description: Non-Invasive Measurement of Oxygen Saturation and Pulse Rate WithDocument4 pages1.pulse Oximeter: General Description: Non-Invasive Measurement of Oxygen Saturation and Pulse Rate WithFuadNo ratings yet
- 5Q0765RTDocument10 pages5Q0765RTFuadNo ratings yet
- The Specifications of K15A60D: Details PDFDocument1 pageThe Specifications of K15A60D: Details PDFFuadNo ratings yet
- Silicon PNP Power Transistors: Product SpecificationDocument3 pagesSilicon PNP Power Transistors: Product SpecificationFuadNo ratings yet
- A Rarest Case of Post-Partum Uterine Prolapsed in Doe RabbitDocument2 pagesA Rarest Case of Post-Partum Uterine Prolapsed in Doe RabbitReissa YuniaNo ratings yet
- Ulcirex CapsuleDocument3 pagesUlcirex Capsulehk_scribdNo ratings yet
- 2.nutrition Guide For Physicians PDFDocument444 pages2.nutrition Guide For Physicians PDFMauro Lopez100% (2)
- Cholesteatoma and Ear SurgeryDocument508 pagesCholesteatoma and Ear SurgeryKarolina RamirezNo ratings yet
- OsteomyelitisDocument20 pagesOsteomyelitisYusri HarisNo ratings yet
- Pulse Rate LabDocument4 pagesPulse Rate LabTishana ThompsonNo ratings yet
- Medication Administration Sheet SampleDocument2 pagesMedication Administration Sheet SampleAmeliaM100% (2)
- Bacillus Amyloliquefaciens A ReviewDocument9 pagesBacillus Amyloliquefaciens A ReviewGaurav DhumalNo ratings yet
- A Manual On Clinical Surgery by Das S: 8.lee Mcgregor'S Synopsis of Surgical Anatomy 500Document1 pageA Manual On Clinical Surgery by Das S: 8.lee Mcgregor'S Synopsis of Surgical Anatomy 500prabhakarNo ratings yet
- Substance Related DisordersDocument29 pagesSubstance Related DisordersAnonymous nz9rhHNo ratings yet
- PSRC Medical and Consent Form 20230727Document3 pagesPSRC Medical and Consent Form 20230727bigdog99bcNo ratings yet
- Definition and Aim of EpidemiologyDocument25 pagesDefinition and Aim of EpidemiologyJeevan KumarNo ratings yet
- Effect of Honey Bee Venom Apis Mellifera On Hyperglycemia and Hyperlipidemia in Alloxan Induced Diabetic Rabbits 2155 6156.1000507Document4 pagesEffect of Honey Bee Venom Apis Mellifera On Hyperglycemia and Hyperlipidemia in Alloxan Induced Diabetic Rabbits 2155 6156.1000507Solongo GanboldNo ratings yet
- KoshtaDocument15 pagesKoshtaPanchakarma DepartmentNo ratings yet
- Pharmacology NotesDocument30 pagesPharmacology NotesJessica WalkerNo ratings yet
- Self Health Resource Center: Liver & Gallbladder Cleanse and FlushDocument6 pagesSelf Health Resource Center: Liver & Gallbladder Cleanse and FlushIulian CracanaNo ratings yet
- Trindade 2018Document10 pagesTrindade 2018Tales FernandoNo ratings yet
- OPHTHA Case Report Diabetic RetinopathyDocument51 pagesOPHTHA Case Report Diabetic RetinopathyJessa MeaNo ratings yet
- C 315Document54 pagesC 315Rumana AliNo ratings yet
- Chapter 1 Cardiology PDFDocument48 pagesChapter 1 Cardiology PDFkatNo ratings yet
- Management Flabby RidgeDocument4 pagesManagement Flabby RidgeNidya Patricia Sembiring100% (1)
- AllopurinolDocument7 pagesAllopurinolSahera Nurhidayah NasutionNo ratings yet
- BDS PDFDocument4 pagesBDS PDFMahendra KumarNo ratings yet
- Systemic VPT-Lecture NotesDocument34 pagesSystemic VPT-Lecture NotesshNo ratings yet
- Anesthetics: Local Topical: Name Indications Peak Effect (Min) Duration (Min) AmidesDocument3 pagesAnesthetics: Local Topical: Name Indications Peak Effect (Min) Duration (Min) Amidesammar amerNo ratings yet
- Health Facts 2021Document19 pagesHealth Facts 2021azhar samsung2No ratings yet
- The Risk of Childbearing Manila 05 PDFDocument14 pagesThe Risk of Childbearing Manila 05 PDFBrix ValdrizNo ratings yet
- TMJ AnkylosisDocument66 pagesTMJ Ankylosisumesh dombale100% (1)