Download as pptx, pdf, or txt
You might also like
- CNusat Riko The AdventurerDocument38 pagesCNusat Riko The AdventurerMuhammad Farhan Saiful AzmanNo ratings yet
- Powerpoint: Colorectal Polyps and Colorectal CarcinomaDocument68 pagesPowerpoint: Colorectal Polyps and Colorectal Carcinomaj.doe.hex_87100% (5)
- Project Proposal DraftDocument14 pagesProject Proposal DraftAdasa EdwardsNo ratings yet
- Oncology 11Document24 pagesOncology 11anbumanijayakumarrewNo ratings yet
- Urinary Tract CancerDocument53 pagesUrinary Tract CancerandikaisnaeniNo ratings yet
- Colon: Malueth AbrahamDocument39 pagesColon: Malueth AbrahamMalueth AnguiNo ratings yet
- Appendiceal Cancer: - 1% of Appendectomies Contain CancerDocument28 pagesAppendiceal Cancer: - 1% of Appendectomies Contain CancerRajendra SoniNo ratings yet
- Colon and Rectal CancerDocument62 pagesColon and Rectal CancerSK TalkNo ratings yet
- Urology Final Exam SummaryDocument6 pagesUrology Final Exam SummaryPanda PandaNo ratings yet
- ONCOLOGICAL GYNECOLOGY-Malignant Diseases of The Vulva and Modalities of Treatment by Prof - Dr.Vesna AntovskaDocument22 pagesONCOLOGICAL GYNECOLOGY-Malignant Diseases of The Vulva and Modalities of Treatment by Prof - Dr.Vesna AntovskaVesna AntovskaNo ratings yet
- Kidneys, UB, Prostate, TesticlesDocument37 pagesKidneys, UB, Prostate, TesticlesAkash KumarNo ratings yet
- Appendiceal Ca mgt-1Document17 pagesAppendiceal Ca mgt-1Worku KifleNo ratings yet
- Gastric CancerDocument126 pagesGastric Cancermwani775100% (1)
- Urinary Bladder PathologyDocument16 pagesUrinary Bladder Pathologyv@r0_5No ratings yet
- Bladder CancerDocument43 pagesBladder CancerIsaac MwangiNo ratings yet
- CA OesophagusDocument47 pagesCA OesophagusAnsif KNo ratings yet
- Wilms TumorDocument11 pagesWilms TumorChichi Basar67% (3)
- Bladder TumorsDocument13 pagesBladder TumorsAngela RosaNo ratings yet
- Colorectal Ca (CRC) .: Malueth Abraham, MBCHB ViDocument36 pagesColorectal Ca (CRC) .: Malueth Abraham, MBCHB ViMalueth AnguiNo ratings yet
- Carcinoma Oesophagus: Dr. S. Ranita DeviDocument46 pagesCarcinoma Oesophagus: Dr. S. Ranita DeviVivek AhanthemNo ratings yet
- Renal Parenchymal TumorsDocument45 pagesRenal Parenchymal TumorsDaniel100% (1)
- Billet 12Document3 pagesBillet 12Tarun GargNo ratings yet
- 19 UrothelialDocument16 pages19 Urothelialenglish-exactlyNo ratings yet
- Rectum: Malueth AbrahamDocument19 pagesRectum: Malueth AbrahamMalueth AnguiNo ratings yet
- ONCOLOGICAL GYNECOLOGY - Malignant Tumors of The Vagina and Modalities of TreatmentDocument9 pagesONCOLOGICAL GYNECOLOGY - Malignant Tumors of The Vagina and Modalities of TreatmentVesna AntovskaNo ratings yet
- Bladder Cancer 1Document31 pagesBladder Cancer 1Anas HamadNo ratings yet
- (Riola) Intestinal Neoplasm, Obesity and OverweightDocument38 pages(Riola) Intestinal Neoplasm, Obesity and Overweightlovely roan riolaNo ratings yet
- Carcinoma Gall BladderDocument25 pagesCarcinoma Gall Bladderrajan kumarNo ratings yet
- Upper Git TumorsDocument51 pagesUpper Git TumorsIsaac MwangiNo ratings yet
- Esophageal CADocument56 pagesEsophageal CAEdwin OkonNo ratings yet
- Cholangiocarcinoma: R.KarthikeyanDocument49 pagesCholangiocarcinoma: R.KarthikeyanKarthikeyan R100% (2)
- Cervical CancerDocument36 pagesCervical CancerPro fatherNo ratings yet
- GIT, CorrectedDocument105 pagesGIT, Correctedali attiaNo ratings yet
- Rectal Ca:: Malueth Abraham, MBCHB ViDocument32 pagesRectal Ca:: Malueth Abraham, MBCHB ViMalueth AnguiNo ratings yet
- Carcinoma Penis: Pravin NarkhedeDocument36 pagesCarcinoma Penis: Pravin Narkhedepravin narkhede100% (1)
- Diseases of The Peritoneal CavityDocument19 pagesDiseases of The Peritoneal CavityJoanna BisNo ratings yet
- Colonic and Small Intestine Disorders-1Document28 pagesColonic and Small Intestine Disorders-1YIKI ISAACNo ratings yet
- Clinical Presentation, Diagnosis, and Staging of Bladder Cancer - UpToDateDocument29 pagesClinical Presentation, Diagnosis, and Staging of Bladder Cancer - UpToDateMario Lopez CastellanosNo ratings yet
- Karsinoma Buli-BuliDocument10 pagesKarsinoma Buli-BuliHumaira AgustinaNo ratings yet
- Karsinoma Buli-BuliDocument10 pagesKarsinoma Buli-BuliHumaira AgustinaNo ratings yet
- Small IntestineDocument4 pagesSmall IntestineSiruNo ratings yet
- Periampullary Cancer1Document18 pagesPeriampullary Cancer1Muhammad UsamaNo ratings yet
- ONCO - Shweta NaikDocument16 pagesONCO - Shweta NaikShweta NaikNo ratings yet
- Peritoneal Carcinomatosis Recent Advances in Surgery - 16 Edition Roshanlal GuptaDocument48 pagesPeritoneal Carcinomatosis Recent Advances in Surgery - 16 Edition Roshanlal GuptaPraveen CpNo ratings yet
- Retroperitoneal MassesDocument34 pagesRetroperitoneal MassesBanaz SadiqNo ratings yet
- Carcinoma of OesophagusDocument18 pagesCarcinoma of Oesophaguszxcvbzaki123No ratings yet
- Diseases of Rectum and Anal CanalDocument68 pagesDiseases of Rectum and Anal CanalKoridor Falua Sakti Halawa 21000063No ratings yet
- Colorectal Cancer : Presented By: Anas Jolani - Amiral Aiman - Ahmed FathiDocument55 pagesColorectal Cancer : Presented By: Anas Jolani - Amiral Aiman - Ahmed FathiRashed ShatnawiNo ratings yet
- Carcinoma Rectum - Janak - NEWDocument74 pagesCarcinoma Rectum - Janak - NEWTowhidulIslamNo ratings yet
- DR 180114164748Document43 pagesDR 180114164748Hasnain ToheedNo ratings yet
- Colon CancerDocument5 pagesColon CancerPan Dong100% (1)
- Neoplasmsofoesophagus 230619112311 Dfc34b23Document59 pagesNeoplasmsofoesophagus 230619112311 Dfc34b23Dharmdev YadavNo ratings yet
- Colon CancerDocument45 pagesColon CancerbukankhadamNo ratings yet
- Small - Intestinal Neoplasms and Carcinoid TumorsDocument51 pagesSmall - Intestinal Neoplasms and Carcinoid TumorsOlga GoryachevaNo ratings yet
- CT Peritoneal Carcinomat and Mimics 2014Document12 pagesCT Peritoneal Carcinomat and Mimics 2014gatoflacoNo ratings yet
- Dr. E. J. Arteen F.R.C.S General & Colorectal Consultant SurgeonDocument65 pagesDr. E. J. Arteen F.R.C.S General & Colorectal Consultant SurgeonEslam R. Almassri100% (1)
- Carcinoma of ColonDocument39 pagesCarcinoma of ColonMuhammad DaniyalNo ratings yet
- Cancer of The BladderDocument22 pagesCancer of The BladderKarl Kiw-isNo ratings yet
- Vaginal CancerDocument12 pagesVaginal CancerJohn Christopher LucesNo ratings yet
- Pathology Lab.: Gastrointestinal Tract MD IvDocument27 pagesPathology Lab.: Gastrointestinal Tract MD IvPablo SisirucaNo ratings yet
- Retroperitoneal Tumors: Clinical ManagementFrom EverandRetroperitoneal Tumors: Clinical ManagementCheng-Hua LuoNo ratings yet
- Endoscopic Ultrasound Management of Pancreatic Lesions: From Diagnosis to TherapyFrom EverandEndoscopic Ultrasound Management of Pancreatic Lesions: From Diagnosis to TherapyAntonio FacciorussoNo ratings yet
- GODIVA PRÉsentationDocument34 pagesGODIVA PRÉsentationJulie JulietteNo ratings yet
- 60. Đề Thi Thử TN THPT 2021 - Môn Tiếng Anh - Sở GD & ĐT Hưng Yên - File Word Có Lời GiảiDocument6 pages60. Đề Thi Thử TN THPT 2021 - Môn Tiếng Anh - Sở GD & ĐT Hưng Yên - File Word Có Lời GiảiMinh DươngNo ratings yet
- Ynatrwl Nonannexure2022augm25 5532078444 8661400943Document4 pagesYnatrwl Nonannexure2022augm25 5532078444 8661400943INSIGNIA LABS - DATANo ratings yet
- United States Court of Appeals, Eleventh CircuitDocument52 pagesUnited States Court of Appeals, Eleventh CircuitScribd Government DocsNo ratings yet
- Messianic Theology and Christian Faith - G. A. RigganDocument206 pagesMessianic Theology and Christian Faith - G. A. RigganLucianaNo ratings yet
- Lean Management Tools in Aviation Industry - New Wine Into Old Wineskins (#1037251) - 2134747Document7 pagesLean Management Tools in Aviation Industry - New Wine Into Old Wineskins (#1037251) - 2134747Mohammed Yassin ChampionNo ratings yet
- Formal Letters - 2020 Class X - Letter To The Editor, Complaint LetterDocument7 pagesFormal Letters - 2020 Class X - Letter To The Editor, Complaint LetterVandana RawatNo ratings yet
- Vedanta Solution To Our Fundamental ProblemDocument356 pagesVedanta Solution To Our Fundamental Problemspikeman42100% (1)
- Personal Lifelong Learning PlanDocument7 pagesPersonal Lifelong Learning PlanRamilAdubal100% (2)
- The Residences at Greenbelt Manila Tower 1-Bedroom For Sale 24DDocument2 pagesThe Residences at Greenbelt Manila Tower 1-Bedroom For Sale 24DJP ReyesNo ratings yet
- AMS4029MDocument5 pagesAMS4029M黄当甲No ratings yet
- Eslprintables 2009810153647888645279Document1 pageEslprintables 2009810153647888645279Mathéo DE OLIVEIRANo ratings yet
- Comtemporary ResearchDocument11 pagesComtemporary ResearchKlthryn Dairo CabilesNo ratings yet
- Your World 3 Grammar Presentation 1 2Document7 pagesYour World 3 Grammar Presentation 1 2epalmerNo ratings yet
- Las Castellana BananaDocument28 pagesLas Castellana BananajerichomuhiNo ratings yet
- M-Sand in Tamil NaduDocument9 pagesM-Sand in Tamil Nadurameshkanu1No ratings yet
- En 288 377Document90 pagesEn 288 377Vitaliy KlimenkoNo ratings yet
- Soy Un Discipulo de JesucristoDocument27 pagesSoy Un Discipulo de JesucristoMaggySUDNo ratings yet
- Basic Cell Culture TechniquesDocument22 pagesBasic Cell Culture TechniquestapanagnihotriNo ratings yet
- NCERT Book For Class 9 English Poem A Legend of The NorthlandDocument3 pagesNCERT Book For Class 9 English Poem A Legend of The NorthlandSD PNo ratings yet
- Blood Donation Management SystemDocument55 pagesBlood Donation Management SystemMounika50% (18)
- 1359 - 1368. TingkahanDocument5 pages1359 - 1368. TingkahanRizal Daujr Tingkahan IIINo ratings yet
- Dracula and TBC CheatsheetDocument2 pagesDracula and TBC CheatsheetalicejessicapreesNo ratings yet
- (PHYS1112) (2017) (F) Final R8udkjdt 62165Document18 pages(PHYS1112) (2017) (F) Final R8udkjdt 62165black.widow.010300No ratings yet
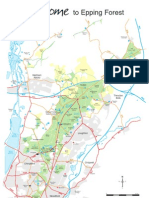
- Epping Forest MapDocument1 pageEpping Forest MapViktor CasualNo ratings yet
- NCBTSDocument44 pagesNCBTSGlenn GomezNo ratings yet
- 2014 SIM Annual Report Print FriendlyDocument73 pages2014 SIM Annual Report Print Friendlyzaid chaudry1No ratings yet
- Services To GASCO On Unified Drawing Format & Drawing AutomationDocument14 pagesServices To GASCO On Unified Drawing Format & Drawing Automationmadhu_karekar100% (1)