Download as pptx, pdf, or txt
You might also like
- Copd 19Document31 pagesCopd 19ghgggtNo ratings yet
- Breathing Terhadap Penurunan Respiratory Rate: Diajukan Sebagai Salah Satu Syarat Memperoleh Gelar Ners KeperawatanDocument31 pagesBreathing Terhadap Penurunan Respiratory Rate: Diajukan Sebagai Salah Satu Syarat Memperoleh Gelar Ners KeperawatanSri Susanti AbdulwahabNo ratings yet
- Gas ExchangeDocument15 pagesGas ExchangeOsolemio Mer100% (1)
- Penyakit Paru Obstruktif Kronik (Ppok)Document32 pagesPenyakit Paru Obstruktif Kronik (Ppok)Rudy LusmiandaNo ratings yet
- Asthma Harrisons ClubDocument84 pagesAsthma Harrisons ClubLady AngodNo ratings yet
- COPDDocument59 pagesCOPDKarenmedicalNo ratings yet
- Obstructive Airway DiseasesDocument67 pagesObstructive Airway DiseasesImran Ali TunioNo ratings yet
- COPDDocument37 pagesCOPDNeelesh PatilNo ratings yet
- Lower Airway Disease: Copd Ashtma Tuberculosis Pneumonia Cyst FibrosisDocument39 pagesLower Airway Disease: Copd Ashtma Tuberculosis Pneumonia Cyst FibrosisWidi Marsha FadilaNo ratings yet
- Update in Airway Obstuction DiseaseDocument42 pagesUpdate in Airway Obstuction DiseaseTiyaTyraSidoraNo ratings yet
- Treatment of Bronchial AsthmaDocument50 pagesTreatment of Bronchial AsthmaJindal Chest ClinicNo ratings yet
- PPOK Dinkes Prov RevisiDocument54 pagesPPOK Dinkes Prov Revisidewi wahyuniNo ratings yet
- (Chronic Obstructive Pulmonary Disease) : Kelompok DDocument31 pages(Chronic Obstructive Pulmonary Disease) : Kelompok DErwin BawonoNo ratings yet
- Chronic Obstructive Pulmonary Diseases (COPD) Penyakit Paru Obstruktif Kronik (PPOK)Document55 pagesChronic Obstructive Pulmonary Diseases (COPD) Penyakit Paru Obstruktif Kronik (PPOK)Yolanda Octaviana TariganNo ratings yet
- IPD. 2. DR Theo - PPOKDocument96 pagesIPD. 2. DR Theo - PPOKTheopilus Obed LayNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument17 pagesChronic Obstructive Pulmonary DiseaseMark Adrian Jintalan ManzanoNo ratings yet
- Case Study On CopdDocument24 pagesCase Study On CopdPawan Batth67% (3)
- COPD - Update Diagnosis and Management of Stable COPDDocument29 pagesCOPD - Update Diagnosis and Management of Stable COPDIwanNo ratings yet
- Enfermedad Pulmonar Obstructiva CronicaDocument13 pagesEnfermedad Pulmonar Obstructiva CronicaCharlaNo ratings yet
- NCM 112 LEC Topic 11 AsthmaDocument2 pagesNCM 112 LEC Topic 11 AsthmaViviene Faye FombuenaNo ratings yet
- Ards EndDocument4 pagesArds Endmaherhamdy127No ratings yet
- Chronic Obstructive Pulmonary Disease: NCM 109 Gabriel PangadanDocument9 pagesChronic Obstructive Pulmonary Disease: NCM 109 Gabriel PangadanGabriel Benedict PangadanNo ratings yet
- Enfermedad Pulmonar Obstructiva CronicaDocument13 pagesEnfermedad Pulmonar Obstructiva CronicaCharlaNo ratings yet
- Acute Respiratory Distress Syndrome-Pathophysiology and ManagementDocument4 pagesAcute Respiratory Distress Syndrome-Pathophysiology and ManagementHalo HaloNo ratings yet
- COPDDocument73 pagesCOPDBroken Oreos100% (1)
- Common Respiratory Disease: BY: Niña Alessandra ValerianoDocument20 pagesCommon Respiratory Disease: BY: Niña Alessandra ValerianokarenbescaserNo ratings yet
- Rasionalitation in Anti-Asthma Drugs: Nurfatimah I.R. (030100088) Pipi Malindo H. (030100092) Deyvia Daulay (030100094)Document31 pagesRasionalitation in Anti-Asthma Drugs: Nurfatimah I.R. (030100088) Pipi Malindo H. (030100092) Deyvia Daulay (030100094)Vita DesriantiNo ratings yet
- Asthma COPD Overlap Syndrome - ACOSDocument59 pagesAsthma COPD Overlap Syndrome - ACOSdrmaqsoodaliNo ratings yet
- Optimizing Management of Asthma and COPDDocument58 pagesOptimizing Management of Asthma and COPDJindal Chest ClinicNo ratings yet
- Asthma & Copd Cme 2 FinalDocument51 pagesAsthma & Copd Cme 2 Finaldrewstark496No ratings yet
- COPD Lecture Slides For BlackBoardDocument52 pagesCOPD Lecture Slides For BlackBoardClayton JensenNo ratings yet
- Formoterol Gonzaga.Document2 pagesFormoterol Gonzaga.Sheryl Anne GonzagaNo ratings yet
- SL NO Content NODocument12 pagesSL NO Content NOPdianghunNo ratings yet
- Biologic Crisis: Prepared By: Ronnie M. Amazona, RN, ManDocument162 pagesBiologic Crisis: Prepared By: Ronnie M. Amazona, RN, ManLex CatNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document16 pagesChronic Obstructive Pulmonary Disease (COPD)Kimberly Abella CabreraNo ratings yet
- COPD Stepwise DigitalDocument1 pageCOPD Stepwise DigitalJeff CrocombeNo ratings yet
- Copd FK Unhas 2015Document28 pagesCopd FK Unhas 2015Muhammad Nur DelaphanEnamNo ratings yet
- Resource ViewDocument54 pagesResource ViewHamza AdeelNo ratings yet
- Childhood Asthma: DR - Rodman Tarigan, Spa.,MkesDocument35 pagesChildhood Asthma: DR - Rodman Tarigan, Spa.,MkesBambang IrwansyahNo ratings yet
- Covid 2021Document48 pagesCovid 2021Diego SarmientoNo ratings yet
- Chronic-Obstructive-Pulmonary-Disease 20240329 210008 0000Document4 pagesChronic-Obstructive-Pulmonary-Disease 20240329 210008 0000Mariel MuñezNo ratings yet
- PneumoniaSystem DisorderDocument1 pagePneumoniaSystem DisorderAA DDNo ratings yet
- 1 CopdDocument37 pages1 CopdnaturehalwestNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument24 pagesChronic Obstructive Pulmonary DiseasePratap JoshiNo ratings yet
- Case Study Opd UfcDocument13 pagesCase Study Opd UfcShan DyNo ratings yet
- Copd (Ppok) : Chronic Care ManagemantDocument33 pagesCopd (Ppok) : Chronic Care ManagemantTaufiq HidayatNo ratings yet
- Simposium 2.2 Dr. Luluk How Important Is ICSLABADocument27 pagesSimposium 2.2 Dr. Luluk How Important Is ICSLABAAndre AdhityoNo ratings yet
- 02 Bronchial AsthmaDocument6 pages02 Bronchial AsthmaahmedNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document21 pagesChronic Obstructive Pulmonary Disease (COPD)MudrekaNo ratings yet
- Athira UDocument22 pagesAthira UJuvana LachuNo ratings yet
- Chronic Bronchitis, Emphysema, Bronciectasis - PPT.Document51 pagesChronic Bronchitis, Emphysema, Bronciectasis - PPT.Jumar ValdezNo ratings yet
- Lower Respiratory (Autosaved)Document58 pagesLower Respiratory (Autosaved)VIVEK DHADYANNo ratings yet
- Case Discussion - CopdDocument63 pagesCase Discussion - CopdrajeshNo ratings yet
- COPDDocument70 pagesCOPDDr. Rizwana SamrinNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument23 pagesChronic Obstructive Pulmonary DiseaseLe RobertNo ratings yet
- Diseases of THE Respiratory System: Group 7Document57 pagesDiseases of THE Respiratory System: Group 7Fritz Darryl DavidNo ratings yet
- MOHFW Critical Care GuidelinesDocument123 pagesMOHFW Critical Care GuidelinesMOHAMMED IQBALNo ratings yet
- Copd Gold 2016Document5 pagesCopd Gold 2016adheNo ratings yet
- EDIT Respiratory Failure Assessment and Problem SolvingDocument66 pagesEDIT Respiratory Failure Assessment and Problem Solvingmursidstone.mursidNo ratings yet
- CopdDocument17 pagesCopdNAMREENNo ratings yet
- CopdDocument18 pagesCopdSalman KhanNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- How To Use A Metered Dose Inhaler 21 HL 8165Document2 pagesHow To Use A Metered Dose Inhaler 21 HL 8165nuhaNo ratings yet
- Original: DOI 10.1007/s00134-016-4617-8Document8 pagesOriginal: DOI 10.1007/s00134-016-4617-8qvc.regulatory 2No ratings yet
- Nursing Care Plan: Lorma Colleges Con Template Related Learning ExperienceDocument6 pagesNursing Care Plan: Lorma Colleges Con Template Related Learning ExperiencePauline GarciaNo ratings yet
- (Ped-W1) (Dr. Zuhair M. Al Musawi) Childhood AsthmaDocument71 pages(Ped-W1) (Dr. Zuhair M. Al Musawi) Childhood AsthmaHaider Nadhem AL-rubaiNo ratings yet
- Early View: A Randomised Trial of High-Flow Nasal Cannula in Infants With Moderate BronchiolitisDocument28 pagesEarly View: A Randomised Trial of High-Flow Nasal Cannula in Infants With Moderate BronchiolitisutamiprakosoNo ratings yet
- Gambaran Pendampingan Pengobatan ISPA (Infeksi Saluran Pernapasan Akut) Non Pneumonia Oleh Tenaga Kesehatan Di Puskesmas Cilacap Selatan IIDocument9 pagesGambaran Pendampingan Pengobatan ISPA (Infeksi Saluran Pernapasan Akut) Non Pneumonia Oleh Tenaga Kesehatan Di Puskesmas Cilacap Selatan IIRaihan Muhammad IsvandiarNo ratings yet
- 1.b. Bronchiolitis Clinical Presentation - History, Physical Examination, ComplicationsDocument3 pages1.b. Bronchiolitis Clinical Presentation - History, Physical Examination, ComplicationsDavid CraigNo ratings yet
- Content On Pediatric Asthma: Submitted To Mrs. Rupinder Kaur Lecturer Submitted by Anu George MSC Nsg. 1 YearDocument11 pagesContent On Pediatric Asthma: Submitted To Mrs. Rupinder Kaur Lecturer Submitted by Anu George MSC Nsg. 1 YeargopscharanNo ratings yet
- APRV VentilationDocument5 pagesAPRV VentilationIrina UngureanuNo ratings yet
- Asthma: Sure Name Saputra First Name RandaDocument3 pagesAsthma: Sure Name Saputra First Name Randalia bhaktiNo ratings yet
- Pulmonary Medicine 1Document28 pagesPulmonary Medicine 1Gloria JaisonNo ratings yet
- Machanical Ventilator Nursing Care PalnDocument13 pagesMachanical Ventilator Nursing Care PalnAnnie Priscilla100% (1)
- Respiratory EmergenciesDocument30 pagesRespiratory EmergenciesNovriefta NugrahaNo ratings yet
- Kaddam Multispeciality Hospital: (Mini Bypass, Bank Colony, Rohtak Road, Bhiwani, HR, 127021)Document6 pagesKaddam Multispeciality Hospital: (Mini Bypass, Bank Colony, Rohtak Road, Bhiwani, HR, 127021)sunitapuniaNo ratings yet
- Anatomia Patrones IntersticialesDocument16 pagesAnatomia Patrones IntersticialesIrai MartínezNo ratings yet
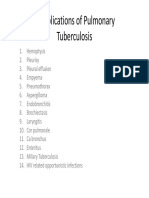
- Complication of TBDocument15 pagesComplication of TBTintin PoncianoNo ratings yet
- Student Nurses' Community: Nursing Care Plan PneumoniaDocument2 pagesStudent Nurses' Community: Nursing Care Plan PneumoniaNur SanaaniNo ratings yet
- VentilatorDocument17 pagesVentilatorDongxia WuNo ratings yet
- Volume Controlled VentilationDocument7 pagesVolume Controlled VentilationVijay GadagiNo ratings yet
- 02 2018 Biomedical Instrumentation - Measurement of RespirationDocument28 pages02 2018 Biomedical Instrumentation - Measurement of Respirationviki mikiNo ratings yet
- Quiz2 1 Issue2Document2 pagesQuiz2 1 Issue2Jazur AhamedNo ratings yet
- NebulizationDocument4 pagesNebulizationleoNo ratings yet
- Overview of Mechanical Ventilation - Critical Care Medicine - Merck Manuals Professional EditionDocument8 pagesOverview of Mechanical Ventilation - Critical Care Medicine - Merck Manuals Professional EditionParas KanwarNo ratings yet
- Chest PhysiotherapyDocument13 pagesChest PhysiotherapyAlma Susan100% (1)
- GE Healthcare: Premarket Notification 510 (K) Summary As Required by Section 807.92 Engstrom VentilatorDocument7 pagesGE Healthcare: Premarket Notification 510 (K) Summary As Required by Section 807.92 Engstrom VentilatorHAITHM MURSHEDNo ratings yet
- Тopic 4.2. Auscultation of the lungs. Additional sounds.Document7 pagesТopic 4.2. Auscultation of the lungs. Additional sounds.Donia HnainiaNo ratings yet
- Weaning Patients With Obesity From Ventilatory Support: ReviewDocument9 pagesWeaning Patients With Obesity From Ventilatory Support: ReviewGian CarloNo ratings yet
- Chest, Abdomen and RheumatologyDocument142 pagesChest, Abdomen and RheumatologyAhmed JaoadNo ratings yet