Download as pptx, pdf, or txt
You might also like
- Sans 1200 HDocument3 pagesSans 1200 HfilipeNo ratings yet
- Pre-Hospital Trauma CareDocument8 pagesPre-Hospital Trauma Carecorsaru100% (1)
- Emergency NursingDocument10 pagesEmergency Nursingkellyhutch50% (2)
- Trauma NursingDocument35 pagesTrauma NursingGodwin Babista Gonzales100% (2)
- Comic Relief Core Strength Fund - AnalysisDocument25 pagesComic Relief Core Strength Fund - AnalysisNCVO100% (3)
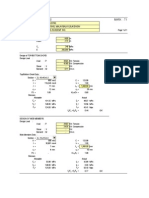
- Spirit Levels - Block LevelsDocument4 pagesSpirit Levels - Block LevelsGia Minh Tieu Tu100% (1)
- 4.surgical DiseaseDocument8 pages4.surgical Diseasekrq7d4yqf7No ratings yet
- TraumaDocument49 pagesTraumamahdi aljamalNo ratings yet
- 087 Pre Hospital Trauma CareDocument9 pages087 Pre Hospital Trauma CareabbuahmedibbuNo ratings yet
- Chapter 4 BleedingDocument21 pagesChapter 4 BleedingAnna MethyldaNo ratings yet
- Jason Wolfe's ATLS Trauma Moulage Page: (Thoughts On The Management of The Multiply Injured Patient)Document18 pagesJason Wolfe's ATLS Trauma Moulage Page: (Thoughts On The Management of The Multiply Injured Patient)gogopal100% (6)
- First Aid For Bleeding and Taking Care of - 124731Document21 pagesFirst Aid For Bleeding and Taking Care of - 124731Kim KaundaNo ratings yet
- Tactical Combat Casualty CareDocument114 pagesTactical Combat Casualty Caresrtmedic100% (5)
- Trauma: Dr. Hasanain Abdulammer JasimDocument41 pagesTrauma: Dr. Hasanain Abdulammer Jasimميمونه عبد الرحيم مصطفىNo ratings yet
- Patient Evaluation and Wound Assessment: Key Practice PointsDocument6 pagesPatient Evaluation and Wound Assessment: Key Practice PointsFofiuNo ratings yet
- Trauma Gunshot WoundsDocument11 pagesTrauma Gunshot Woundschrisr310No ratings yet
- Trauma Assessment Initial Trauma AssessmentDocument6 pagesTrauma Assessment Initial Trauma Assessmentrika100% (1)
- HEMA2 - Bleeding Time Written ReportDocument10 pagesHEMA2 - Bleeding Time Written ReportMarjorie GabalunosNo ratings yet
- C0274 Specialty Guide Orthopaedic Trauma v2 14 AprilDocument7 pagesC0274 Specialty Guide Orthopaedic Trauma v2 14 AprilRema AmerNo ratings yet
- Pre Analytical ConsiderationsDocument54 pagesPre Analytical ConsiderationsLycah Jyde PechuancoNo ratings yet
- Basic First Aid - FuturelearnDocument11 pagesBasic First Aid - FuturelearnSuhaib SghaireenNo ratings yet
- Disaster Triage CategoriesDocument63 pagesDisaster Triage CategoriesJanna Arianne Servan TomasNo ratings yet
- Amputation and Hemorrhage ControlDocument17 pagesAmputation and Hemorrhage ControlIlyes FerenczNo ratings yet
- IV Therapy SsDocument56 pagesIV Therapy Sssaeed_chohan100% (8)
- Nclex RN Actual ExamDocument32 pagesNclex RN Actual ExamIrfan AliNo ratings yet
- 3 Tactical Field CareDocument164 pages3 Tactical Field CareINSTRUCTOR INTERNACIONAL ANTONIO RAMIREZNo ratings yet
- Cardiac CardiacResynchronizationTherapyDefibrillator 0117 EngDocument3 pagesCardiac CardiacResynchronizationTherapyDefibrillator 0117 EngStella PraphulKumarNo ratings yet
- First AidDocument7 pagesFirst AidElla MarieNo ratings yet
- External Hemorrhage 1Document17 pagesExternal Hemorrhage 1Junalyn MartinezNo ratings yet
- ATLS 10th Edition ChangesDocument71 pagesATLS 10th Edition Changessharvindan subramaniam67% (3)
- NYSORA Hazdics RegionalDocument8 pagesNYSORA Hazdics RegionalAishu BNo ratings yet
- What Is First AidDocument6 pagesWhat Is First AidNaomi RamirezNo ratings yet
- Intravenous Therapy Notes OnlineDocument5 pagesIntravenous Therapy Notes OnlineDexie James Ventenilla DizonNo ratings yet
- First AidDocument54 pagesFirst AidMadhavi ModaNo ratings yet
- Laboratory #1 Bleeding Time Skills 4 Points ObjectivesDocument9 pagesLaboratory #1 Bleeding Time Skills 4 Points ObjectivesMaz AndikaNo ratings yet
- Post Operative Emergency Management in Periodontics PeioDocument40 pagesPost Operative Emergency Management in Periodontics PeioFourthMolar.comNo ratings yet
- Mass Casualty Incident (MCI) ResponseDocument25 pagesMass Casualty Incident (MCI) ResponseMary Joy GarciaNo ratings yet
- Nur 3552 Emergency CareDocument32 pagesNur 3552 Emergency CareKhadijah ShaariNo ratings yet
- Hemorrhoidectomy ManuscriptDocument5 pagesHemorrhoidectomy ManuscriptMa. Ydela MeradoresNo ratings yet
- 12 Commandments Wound CareDocument10 pages12 Commandments Wound CareBecky HowardNo ratings yet
- First Aid-Guide&treamentDocument30 pagesFirst Aid-Guide&treamentHoda ElebrashyNo ratings yet
- Triage Is The Process of Determining The Priority of Patients' Treatments Based On The Severity ofDocument7 pagesTriage Is The Process of Determining The Priority of Patients' Treatments Based On The Severity ofRalph PelegrinoNo ratings yet
- Atls Advanced Trauma Life Support: DR - Alex, MDDocument73 pagesAtls Advanced Trauma Life Support: DR - Alex, MDAlex beharuNo ratings yet
- Skills 118 Final LizaDocument66 pagesSkills 118 Final LizaojiNo ratings yet
- FUNDAMENTALS OF TACTICAL COMBAT CASUALTY CARE For PPSCDocument80 pagesFUNDAMENTALS OF TACTICAL COMBAT CASUALTY CARE For PPSColiver garcianoNo ratings yet
- 4 Emergency and Mass Casualty NursingDocument7 pages4 Emergency and Mass Casualty NursingPxPPxH ChanNo ratings yet
- Orthopedic EmergenciesDocument37 pagesOrthopedic EmergenciesRajiv NegandhiNo ratings yet
- Burn Emergency Management For The First Responder-Layout VDocument16 pagesBurn Emergency Management For The First Responder-Layout VnikitagustiNo ratings yet
- First Aid AND Life Saving Techniques: Pcinsp Reuben A Macario, RN, MPM, CeseDocument72 pagesFirst Aid AND Life Saving Techniques: Pcinsp Reuben A Macario, RN, MPM, CeseJd Jamolod PelovelloNo ratings yet
- Driving School First Aid ModuleDocument26 pagesDriving School First Aid ModuleScribdTranslationsNo ratings yet
- HEsi HintsDocument5 pagesHEsi HintsOMGStudy100% (3)
- Start TriageDocument7 pagesStart TriageIrene LopezNo ratings yet
- Consent, JournalDocument32 pagesConsent, JournalthinzarNo ratings yet
- CVC Catheter-Consent OnlyDocument4 pagesCVC Catheter-Consent OnlyRia Gita PratiwiNo ratings yet
- Bullets For Nursing Basic Concepts Part 15Document61 pagesBullets For Nursing Basic Concepts Part 15oh_chamieNo ratings yet
- HemorrhageDocument15 pagesHemorrhageMariegreat Piscos BisnarNo ratings yet
- Dzino's SurgeryDocument718 pagesDzino's SurgeryHuram SeremaniNo ratings yet
- Emergency and Disasater NursingDocument96 pagesEmergency and Disasater Nursingblacknurse100% (3)
- Textbook of Urgent Care Management: Chapter 39, Ensuring Patient SafetyFrom EverandTextbook of Urgent Care Management: Chapter 39, Ensuring Patient SafetyNo ratings yet
- Different in the therapy of pressure negtotheeva single-useFrom EverandDifferent in the therapy of pressure negtotheeva single-useNo ratings yet
- Challenging Arterial Reconstructions: 100 Clinical CasesFrom EverandChallenging Arterial Reconstructions: 100 Clinical CasesNo ratings yet
- Aire Premium Delta 8 Vape - 1000mg - Everything 420Document1 pageAire Premium Delta 8 Vape - 1000mg - Everything 4206hsphckmf8No ratings yet
- The Art Book Page One, Primary Hands - Portfolio Assessment and Art Lessons For Kids - KinderArtDocument9 pagesThe Art Book Page One, Primary Hands - Portfolio Assessment and Art Lessons For Kids - KinderArttote126No ratings yet
- Jurnal - Asmawati - E321192152 .Document11 pagesJurnal - Asmawati - E321192152 .Nurul fuadiNo ratings yet
- At The AirportDocument6 pagesAt The AirportAlen KuharićNo ratings yet
- List of Companies Having SAPDocument2 pagesList of Companies Having SAPKrushikeshNo ratings yet
- Graded Quesions Complete Book0Document344 pagesGraded Quesions Complete Book0Irimia Mihai Adrian100% (1)
- M Tech Dissertation Power SystemDocument7 pagesM Tech Dissertation Power SystemWriteMyStatisticsPaperAkron100% (1)
- POLGOVSEA - MOD 1 - IntroDocument30 pagesPOLGOVSEA - MOD 1 - IntroBryan MarasiganNo ratings yet
- COT-Router Configuration - Docx - Republic of The Philippines DEPARTMENT OF EDUCATION Division of Sultan Kudarat BAI SARIPINANG - College SidekickDocument10 pagesCOT-Router Configuration - Docx - Republic of The Philippines DEPARTMENT OF EDUCATION Division of Sultan Kudarat BAI SARIPINANG - College Sidekickmarivic itongNo ratings yet
- Linear Phase Finite Impulse ResponseDocument30 pagesLinear Phase Finite Impulse ResponseHafizuddin AliNo ratings yet
- Design Furnishings V Zen Path TRO ExtensionDocument11 pagesDesign Furnishings V Zen Path TRO ExtensionEric GoldmanNo ratings yet
- M As1 Formative Task: Review Questions: Star Alliance Sky Team OneworldDocument4 pagesM As1 Formative Task: Review Questions: Star Alliance Sky Team OneworldSharlyne PimentelNo ratings yet
- Biology, Ecology, and Management of The Pea Weevil, Bruchus Pisorum (Coleoptera: Chrysomelidae)Document12 pagesBiology, Ecology, and Management of The Pea Weevil, Bruchus Pisorum (Coleoptera: Chrysomelidae)Alexandra-Ana-Maria VulpeNo ratings yet
- Family Biz BibleDocument26 pagesFamily Biz BibleFrank ParrNo ratings yet
- Training Slides HSE-OH-ST10 Biological HazardsDocument18 pagesTraining Slides HSE-OH-ST10 Biological HazardsAbdul Malik AnsariNo ratings yet
- Software Defined Radio (SDR)Document11 pagesSoftware Defined Radio (SDR)Sanjay GiriNo ratings yet
- Gospel Steel TrussDocument18 pagesGospel Steel TrussJoseph Cloyd L. LamberteNo ratings yet
- Dhaka University Affiliated Colleges: Third Year Syllabus Department of MathematicsDocument8 pagesDhaka University Affiliated Colleges: Third Year Syllabus Department of MathematicsHasibul Hassan ShantoNo ratings yet
- PQR Amp WPQ Standard Testing Parameter WorksheetDocument4 pagesPQR Amp WPQ Standard Testing Parameter WorksheetvinodNo ratings yet
- Charusat 6th SemDocument1 pageCharusat 6th SemdhruvilNo ratings yet
- Wallenberg's BlizzBaller - Diablo 2 at Diablo2Document9 pagesWallenberg's BlizzBaller - Diablo 2 at Diablo2kuntokinteNo ratings yet
- S. Ivo Alla Sapienza and Borrominis Sym PDFDocument25 pagesS. Ivo Alla Sapienza and Borrominis Sym PDFClaudio CastellettiNo ratings yet
- Pakistan Exams BC Bank AccountsDocument4 pagesPakistan Exams BC Bank AccountskhulsanNo ratings yet
- Disk No. Label Comments BootDocument1 pageDisk No. Label Comments BootDavid HiddingsNo ratings yet
- SOP FOR STIFFNESS Tester (09.6.17)Document2 pagesSOP FOR STIFFNESS Tester (09.6.17)Q ANo ratings yet
- Bestiary of The Rosewood Highlands Draft 1-4-08!07!19Document82 pagesBestiary of The Rosewood Highlands Draft 1-4-08!07!19Stefano Chiaramonti100% (2)
- ALB067 Albeo ALV2 Series LED Low Bay Industrial Luminaire Spec SheetDocument4 pagesALB067 Albeo ALV2 Series LED Low Bay Industrial Luminaire Spec SheetsamuelNo ratings yet