
Lai Neurourology & Urodynamics Review
Lai Neurourology & Urodynamics Review
You might also like
- Lisa Blackman-Immaterial Bodies - Affect, Embodiment, Mediation (2012) PDFDocument241 pagesLisa Blackman-Immaterial Bodies - Affect, Embodiment, Mediation (2012) PDFCristina PeñamarínNo ratings yet
- ECG Interpretations DR RPDocument109 pagesECG Interpretations DR RPArnis Putri RosyaniNo ratings yet
- Neurology I - Nervous System: CNS - Brain CNS - Spinal Cord Peripheral Nervous SystemDocument29 pagesNeurology I - Nervous System: CNS - Brain CNS - Spinal Cord Peripheral Nervous SystemDarla Mitu100% (2)
- Thierry Bardini. Junkware. The Essential Junkiness of Our Culture and BiologyDocument298 pagesThierry Bardini. Junkware. The Essential Junkiness of Our Culture and BiologyJulieta Yelin100% (1)
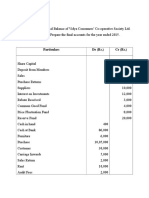
- Final AccountDocument7 pagesFinal Accountswati100% (3)
- Basic Ecg InterpretationDocument88 pagesBasic Ecg Interpretationtristan keeNo ratings yet
- Spinal Cord Gross Anatomy 2Document40 pagesSpinal Cord Gross Anatomy 2Mohamad NasrullohNo ratings yet
- Radicular Syndrome: Darwin Amir BGN Ilmu Penyakit Saraf Fakultas Kedokteran Universitas AndalasDocument32 pagesRadicular Syndrome: Darwin Amir BGN Ilmu Penyakit Saraf Fakultas Kedokteran Universitas Andalasdhilla_18No ratings yet
- Lec33 TbiDocument4 pagesLec33 TbiSatria Faye RespicioNo ratings yet
- Back and Spinal Cord Study Guide: 2.1 Topographic Anatomy Study AimsDocument1 pageBack and Spinal Cord Study Guide: 2.1 Topographic Anatomy Study AimsMihaelaNo ratings yet
- Presentase Paper Ashry SEDocument24 pagesPresentase Paper Ashry SEMahrushLuthfiNo ratings yet
- Practical Neurology: Neurologic ExamDocument114 pagesPractical Neurology: Neurologic ExamDannyNo ratings yet
- EAU Pocket On Neuro Urology 2022Document13 pagesEAU Pocket On Neuro Urology 2022Dane QhNo ratings yet
- Dasar-Dasar Membaca Elektroensefalografi - Gea Pandhita SDocument84 pagesDasar-Dasar Membaca Elektroensefalografi - Gea Pandhita Sgea pandhita sNo ratings yet
- Mri Spine by DR ShamolDocument309 pagesMri Spine by DR Shamolالقارئ محمد سيد عباس mohamed sayed abassNo ratings yet
- Bedside TeachingDocument14 pagesBedside TeachingArum Citra MelatiNo ratings yet
- ECG Module 4aDocument22 pagesECG Module 4aDexter GabrielNo ratings yet
- IVA. Heart ArrhythmiasDocument21 pagesIVA. Heart ArrhythmiasJohn Christopher P. TiamzonNo ratings yet
- ECG Rhythm Interpretation: Module IV ADocument21 pagesECG Rhythm Interpretation: Module IV AImim NozNo ratings yet
- Module 4a.heart ArryhtmiasDocument22 pagesModule 4a.heart ArryhtmiasFerry SofyanriNo ratings yet
- Autonomic Nervous System-1Document46 pagesAutonomic Nervous System-1a-tldNo ratings yet
- Pembekalan Auskultasi Jantung Jimmy AsafDocument45 pagesPembekalan Auskultasi Jantung Jimmy AsafFikriYTNo ratings yet
- ECG Presentation 2020Document131 pagesECG Presentation 2020Kiskeya KafeNo ratings yet
- Sci and Other Disease of The Spinal Cord: Slide 1Document9 pagesSci and Other Disease of The Spinal Cord: Slide 1Dyoan UhhmiitNo ratings yet
- ECG BookDocument232 pagesECG BooklaureeateNo ratings yet
- ECG Rhythm InterpretationDocument208 pagesECG Rhythm InterpretationMariah WaelNo ratings yet
- 8.bladder DysfunctionDocument26 pages8.bladder DysfunctionBhakti WashilkarNo ratings yet
- Table of Contents: Cclusion Omplete Entures Emovable Artial Entures Ixed RosthodonticsDocument88 pagesTable of Contents: Cclusion Omplete Entures Emovable Artial Entures Ixed RosthodonticsghanimNo ratings yet
- Autonomic Nervous SystemDocument28 pagesAutonomic Nervous SystemArt BuenaventuraNo ratings yet
- ECG InterpretationDocument3 pagesECG InterpretationBIANCA ROMELLE STEPHANIE PAYOTNo ratings yet
- Sinus Rhythm and Sinus and Atrial DysrhythmiasDocument41 pagesSinus Rhythm and Sinus and Atrial Dysrhythmiasclaudia brongNo ratings yet
- Case Based Discussion: Ghulam Gilmani 012085663Document36 pagesCase Based Discussion: Ghulam Gilmani 012085663Ghulam GilmaniNo ratings yet
- (Non Trauma) 11 Des Tn. IDocument11 pages(Non Trauma) 11 Des Tn. InadiasalmaNo ratings yet
- ECG Interpretations GoodDocument104 pagesECG Interpretations GoodaymenNo ratings yet
- Case Base Discussion: Advisor: Dr. Nur Anna C Sa'dyah, Sp. PD, K-EMD, FINASIMDocument106 pagesCase Base Discussion: Advisor: Dr. Nur Anna C Sa'dyah, Sp. PD, K-EMD, FINASIMRiza Fadhila MuhammadNo ratings yet
- Case Based Disscusion: Rifqi Ali Zaki (01.208.5765) Advisor Dr. Erwin Budi Cahyono, Sp. PDDocument17 pagesCase Based Disscusion: Rifqi Ali Zaki (01.208.5765) Advisor Dr. Erwin Budi Cahyono, Sp. PDana0% (1)
- ECGDocument154 pagesECGSandeep BansalNo ratings yet
- Primary SurveyDocument30 pagesPrimary SurveyLeo SihombingNo ratings yet
- 2020 10th Week Repetition of Cardiovascular SystemDocument26 pages2020 10th Week Repetition of Cardiovascular SystemBibo BobiNo ratings yet
- ECG InterpretationDocument108 pagesECG InterpretationMohammad SalehNo ratings yet
- 6 - CardiovascularDocument22 pages6 - Cardiovasculardona donneNo ratings yet
- 1.2 Intro To Oxy Diagnostic Procedures For Problems in OxygentionDocument3 pages1.2 Intro To Oxy Diagnostic Procedures For Problems in OxygentionCamille Joy BaliliNo ratings yet
- Module 4aDocument24 pagesModule 4aMaseaNo ratings yet
- CNS (Sensory System) CompiledDocument111 pagesCNS (Sensory System) CompiledChaudhry F MasoodNo ratings yet
- Self-Study - 18 - NeuropsychiatricDocument137 pagesSelf-Study - 18 - NeuropsychiatricAdeyemi OlusolaNo ratings yet
- CBD - Alifa Puspita P - 30101507367Document103 pagesCBD - Alifa Puspita P - 30101507367Jihan NabilaNo ratings yet
- Path Movement-Disorders Tuite SlidesDocument38 pagesPath Movement-Disorders Tuite Slidesberna chuaNo ratings yet
- 07.01 - 12 Lead ECG Interpretation 2019Document141 pages07.01 - 12 Lead ECG Interpretation 2019Lana LocoNo ratings yet
- Paralysis in Dogs and CatsDocument56 pagesParalysis in Dogs and Catscat clinic pdhbNo ratings yet
- ECG Rhythm InterpretationDocument200 pagesECG Rhythm InterpretationabramNo ratings yet
- BALI Respiratory Emergencies BEATTYDocument58 pagesBALI Respiratory Emergencies BEATTYdendikomalaNo ratings yet
- (NS) Arrhythmia Tutorial QuestionsDocument11 pages(NS) Arrhythmia Tutorial QuestionsJoei “Jojo” GohNo ratings yet
- Module 4aDocument22 pagesModule 4aSamer ThaherNo ratings yet
- Nclex RN Review Notes 2018 Triple eDocument30 pagesNclex RN Review Notes 2018 Triple eEndla SriniNo ratings yet
- K5 - Disorders of Autonomic Nervous SystemDocument47 pagesK5 - Disorders of Autonomic Nervous Systemengkiii100% (1)
- For More Free Medical Powerpoint Presentations Visit WebsiteDocument24 pagesFor More Free Medical Powerpoint Presentations Visit Websitevanstar7No ratings yet
- Presentasi Ws Ekg SakinahDocument40 pagesPresentasi Ws Ekg SakinahsiskaNo ratings yet
- Sinus Brad, Tach, PAC, PVCDocument17 pagesSinus Brad, Tach, PAC, PVCEdRobertArnadNo ratings yet
- Upload 9.06 Nerve Impulse Notes To EbackpackDocument24 pagesUpload 9.06 Nerve Impulse Notes To EbackpackPAMELA CASTILLONo ratings yet
- Cellular Components 2Document37 pagesCellular Components 2farzadcop1No ratings yet
- Tutorial Dr. SaugiDocument33 pagesTutorial Dr. SaugifemmytaniaNo ratings yet
- Lesson 18 - Orgasmic Disorder in The MaleDocument9 pagesLesson 18 - Orgasmic Disorder in The MaleJay JiangNo ratings yet
- 20230413083839Document2 pages20230413083839Jay JiangNo ratings yet
- ENT Competitveness - Concerns For Future 2015 - Kaplan PDFDocument3 pagesENT Competitveness - Concerns For Future 2015 - Kaplan PDFJay JiangNo ratings yet
- Author's Accepted Manuscript: 10.1016/j.urpr.2017.04.005Document23 pagesAuthor's Accepted Manuscript: 10.1016/j.urpr.2017.04.005Jay JiangNo ratings yet
- AUA Guideline On RUTI 10-12-22 FinalDocument44 pagesAUA Guideline On RUTI 10-12-22 FinalJay JiangNo ratings yet
- National Trends and Characteristics of Success in The Urology Match ProcessDocument6 pagesNational Trends and Characteristics of Success in The Urology Match ProcessJay JiangNo ratings yet
- EKGDocument31 pagesEKGJay JiangNo ratings yet
- Campbell Biology 12th Edition SummaryDocument6 pagesCampbell Biology 12th Edition Summaryprincesje05No ratings yet
- Notes Ankita KashyapDocument49 pagesNotes Ankita Kashyapkharsatikevin92No ratings yet
- Tort of NegligenceDocument10 pagesTort of NegligenceHETRAM SIYAGNo ratings yet
- TOAD Getting Started GuideDocument50 pagesTOAD Getting Started Guidesmruti_2012No ratings yet
- Joseph Kyle Neibert v. Computer Sciences Corporation, 11th Cir. (2015)Document20 pagesJoseph Kyle Neibert v. Computer Sciences Corporation, 11th Cir. (2015)Scribd Government DocsNo ratings yet
- Puri Brothers: Tax Type: ExemptedDocument66 pagesPuri Brothers: Tax Type: Exemptedmukesh puriNo ratings yet
- Snapshots of A Daughter in LawDocument2 pagesSnapshots of A Daughter in LawReshal AroraNo ratings yet
- Activity STSDocument1 pageActivity STSRalph ZeusNo ratings yet
- Chavara Brochure Edited CompressedDocument13 pagesChavara Brochure Edited CompressedShameer ShajiNo ratings yet
- METHODS OF TEACHING Lesson 1Document19 pagesMETHODS OF TEACHING Lesson 1Joey Bojo Tromes BolinasNo ratings yet
- Grumpy Bear: Some Questions ..Document2 pagesGrumpy Bear: Some Questions ..Mike BNo ratings yet
- Factors Responsible For Burnout Among College StudentsDocument7 pagesFactors Responsible For Burnout Among College StudentsRaj naveenNo ratings yet
- Billy Elliot EssayDocument2 pagesBilly Elliot Essayafabkgddu100% (1)
- Lifestyle Upper Intermediate CB 2012 177p PDFDocument177 pagesLifestyle Upper Intermediate CB 2012 177p PDFԿորյուն ՕհանյանNo ratings yet
- Storification - The Next Big Content Marketing Trend and 3 Benefits Marketers Shouldn't Miss Out OnDocument3 pagesStorification - The Next Big Content Marketing Trend and 3 Benefits Marketers Shouldn't Miss Out OnKetan JhaNo ratings yet
- Applied Economics Syllabus DeclassifiedDocument4 pagesApplied Economics Syllabus DeclassifiedAl Jay MejosNo ratings yet
- Ca. Bhagchand Chechani (Maheshwari)Document8 pagesCa. Bhagchand Chechani (Maheshwari)chechaniNo ratings yet
- Task 2Document4 pagesTask 2Gerardo LanzaNo ratings yet
- Glossary of Terms Relating To Signs and Symptoms: DictionaryDocument9 pagesGlossary of Terms Relating To Signs and Symptoms: DictionaryMishael Octaviany JirehNo ratings yet
- 08 Investmentquestfinal PDFDocument13 pages08 Investmentquestfinal PDFralphalonzo0% (1)
- Young - Coco Chanel Enseñanzas ModaDocument151 pagesYoung - Coco Chanel Enseñanzas ModaLuis Ángel Bejarano MaluquishNo ratings yet
- Aeco136 - Final Term Report (Manatal Multipurpose Cooperatives)Document20 pagesAeco136 - Final Term Report (Manatal Multipurpose Cooperatives)JoyDianneGumatayNo ratings yet
- 【拉图尔】临界区域:关键区域Critical ZonesDocument472 pages【拉图尔】临界区域:关键区域Critical Zoneszhang yanNo ratings yet
- Laguna Tayabas Bus Co V The Public Service CommissionDocument1 pageLaguna Tayabas Bus Co V The Public Service CommissionAnonymous byhgZINo ratings yet
- HR ManualDocument130 pagesHR Manualshikha khanejaNo ratings yet
- Research Design MBA MK02 UNIT IIDocument15 pagesResearch Design MBA MK02 UNIT IIAmit Kumar100% (3)






















































































Download as ppt, pdf, or txt
You might also like
- Lisa Blackman-Immaterial Bodies - Affect, Embodiment, Mediation (2012) PDFDocument241 pagesLisa Blackman-Immaterial Bodies - Affect, Embodiment, Mediation (2012) PDFCristina PeñamarínNo ratings yet
- ECG Interpretations DR RPDocument109 pagesECG Interpretations DR RPArnis Putri RosyaniNo ratings yet
- Neurology I - Nervous System: CNS - Brain CNS - Spinal Cord Peripheral Nervous SystemDocument29 pagesNeurology I - Nervous System: CNS - Brain CNS - Spinal Cord Peripheral Nervous SystemDarla Mitu100% (2)
- Thierry Bardini. Junkware. The Essential Junkiness of Our Culture and BiologyDocument298 pagesThierry Bardini. Junkware. The Essential Junkiness of Our Culture and BiologyJulieta Yelin100% (1)
- Final AccountDocument7 pagesFinal Accountswati100% (3)
- Basic Ecg InterpretationDocument88 pagesBasic Ecg Interpretationtristan keeNo ratings yet
- Spinal Cord Gross Anatomy 2Document40 pagesSpinal Cord Gross Anatomy 2Mohamad NasrullohNo ratings yet
- Radicular Syndrome: Darwin Amir BGN Ilmu Penyakit Saraf Fakultas Kedokteran Universitas AndalasDocument32 pagesRadicular Syndrome: Darwin Amir BGN Ilmu Penyakit Saraf Fakultas Kedokteran Universitas Andalasdhilla_18No ratings yet
- Lec33 TbiDocument4 pagesLec33 TbiSatria Faye RespicioNo ratings yet
- Back and Spinal Cord Study Guide: 2.1 Topographic Anatomy Study AimsDocument1 pageBack and Spinal Cord Study Guide: 2.1 Topographic Anatomy Study AimsMihaelaNo ratings yet
- Presentase Paper Ashry SEDocument24 pagesPresentase Paper Ashry SEMahrushLuthfiNo ratings yet
- Practical Neurology: Neurologic ExamDocument114 pagesPractical Neurology: Neurologic ExamDannyNo ratings yet
- EAU Pocket On Neuro Urology 2022Document13 pagesEAU Pocket On Neuro Urology 2022Dane QhNo ratings yet
- Dasar-Dasar Membaca Elektroensefalografi - Gea Pandhita SDocument84 pagesDasar-Dasar Membaca Elektroensefalografi - Gea Pandhita Sgea pandhita sNo ratings yet
- Mri Spine by DR ShamolDocument309 pagesMri Spine by DR Shamolالقارئ محمد سيد عباس mohamed sayed abassNo ratings yet
- Bedside TeachingDocument14 pagesBedside TeachingArum Citra MelatiNo ratings yet
- ECG Module 4aDocument22 pagesECG Module 4aDexter GabrielNo ratings yet
- IVA. Heart ArrhythmiasDocument21 pagesIVA. Heart ArrhythmiasJohn Christopher P. TiamzonNo ratings yet
- ECG Rhythm Interpretation: Module IV ADocument21 pagesECG Rhythm Interpretation: Module IV AImim NozNo ratings yet
- Module 4a.heart ArryhtmiasDocument22 pagesModule 4a.heart ArryhtmiasFerry SofyanriNo ratings yet
- Autonomic Nervous System-1Document46 pagesAutonomic Nervous System-1a-tldNo ratings yet
- Pembekalan Auskultasi Jantung Jimmy AsafDocument45 pagesPembekalan Auskultasi Jantung Jimmy AsafFikriYTNo ratings yet
- ECG Presentation 2020Document131 pagesECG Presentation 2020Kiskeya KafeNo ratings yet
- Sci and Other Disease of The Spinal Cord: Slide 1Document9 pagesSci and Other Disease of The Spinal Cord: Slide 1Dyoan UhhmiitNo ratings yet
- ECG BookDocument232 pagesECG BooklaureeateNo ratings yet
- ECG Rhythm InterpretationDocument208 pagesECG Rhythm InterpretationMariah WaelNo ratings yet
- 8.bladder DysfunctionDocument26 pages8.bladder DysfunctionBhakti WashilkarNo ratings yet
- Table of Contents: Cclusion Omplete Entures Emovable Artial Entures Ixed RosthodonticsDocument88 pagesTable of Contents: Cclusion Omplete Entures Emovable Artial Entures Ixed RosthodonticsghanimNo ratings yet
- Autonomic Nervous SystemDocument28 pagesAutonomic Nervous SystemArt BuenaventuraNo ratings yet
- ECG InterpretationDocument3 pagesECG InterpretationBIANCA ROMELLE STEPHANIE PAYOTNo ratings yet
- Sinus Rhythm and Sinus and Atrial DysrhythmiasDocument41 pagesSinus Rhythm and Sinus and Atrial Dysrhythmiasclaudia brongNo ratings yet
- Case Based Discussion: Ghulam Gilmani 012085663Document36 pagesCase Based Discussion: Ghulam Gilmani 012085663Ghulam GilmaniNo ratings yet
- (Non Trauma) 11 Des Tn. IDocument11 pages(Non Trauma) 11 Des Tn. InadiasalmaNo ratings yet
- ECG Interpretations GoodDocument104 pagesECG Interpretations GoodaymenNo ratings yet
- Case Base Discussion: Advisor: Dr. Nur Anna C Sa'dyah, Sp. PD, K-EMD, FINASIMDocument106 pagesCase Base Discussion: Advisor: Dr. Nur Anna C Sa'dyah, Sp. PD, K-EMD, FINASIMRiza Fadhila MuhammadNo ratings yet
- Case Based Disscusion: Rifqi Ali Zaki (01.208.5765) Advisor Dr. Erwin Budi Cahyono, Sp. PDDocument17 pagesCase Based Disscusion: Rifqi Ali Zaki (01.208.5765) Advisor Dr. Erwin Budi Cahyono, Sp. PDana0% (1)
- ECGDocument154 pagesECGSandeep BansalNo ratings yet
- Primary SurveyDocument30 pagesPrimary SurveyLeo SihombingNo ratings yet
- 2020 10th Week Repetition of Cardiovascular SystemDocument26 pages2020 10th Week Repetition of Cardiovascular SystemBibo BobiNo ratings yet
- ECG InterpretationDocument108 pagesECG InterpretationMohammad SalehNo ratings yet
- 6 - CardiovascularDocument22 pages6 - Cardiovasculardona donneNo ratings yet
- 1.2 Intro To Oxy Diagnostic Procedures For Problems in OxygentionDocument3 pages1.2 Intro To Oxy Diagnostic Procedures For Problems in OxygentionCamille Joy BaliliNo ratings yet
- Module 4aDocument24 pagesModule 4aMaseaNo ratings yet
- CNS (Sensory System) CompiledDocument111 pagesCNS (Sensory System) CompiledChaudhry F MasoodNo ratings yet
- Self-Study - 18 - NeuropsychiatricDocument137 pagesSelf-Study - 18 - NeuropsychiatricAdeyemi OlusolaNo ratings yet
- CBD - Alifa Puspita P - 30101507367Document103 pagesCBD - Alifa Puspita P - 30101507367Jihan NabilaNo ratings yet
- Path Movement-Disorders Tuite SlidesDocument38 pagesPath Movement-Disorders Tuite Slidesberna chuaNo ratings yet
- 07.01 - 12 Lead ECG Interpretation 2019Document141 pages07.01 - 12 Lead ECG Interpretation 2019Lana LocoNo ratings yet
- Paralysis in Dogs and CatsDocument56 pagesParalysis in Dogs and Catscat clinic pdhbNo ratings yet
- ECG Rhythm InterpretationDocument200 pagesECG Rhythm InterpretationabramNo ratings yet
- BALI Respiratory Emergencies BEATTYDocument58 pagesBALI Respiratory Emergencies BEATTYdendikomalaNo ratings yet
- (NS) Arrhythmia Tutorial QuestionsDocument11 pages(NS) Arrhythmia Tutorial QuestionsJoei “Jojo” GohNo ratings yet
- Module 4aDocument22 pagesModule 4aSamer ThaherNo ratings yet
- Nclex RN Review Notes 2018 Triple eDocument30 pagesNclex RN Review Notes 2018 Triple eEndla SriniNo ratings yet
- K5 - Disorders of Autonomic Nervous SystemDocument47 pagesK5 - Disorders of Autonomic Nervous Systemengkiii100% (1)
- For More Free Medical Powerpoint Presentations Visit WebsiteDocument24 pagesFor More Free Medical Powerpoint Presentations Visit Websitevanstar7No ratings yet
- Presentasi Ws Ekg SakinahDocument40 pagesPresentasi Ws Ekg SakinahsiskaNo ratings yet
- Sinus Brad, Tach, PAC, PVCDocument17 pagesSinus Brad, Tach, PAC, PVCEdRobertArnadNo ratings yet
- Upload 9.06 Nerve Impulse Notes To EbackpackDocument24 pagesUpload 9.06 Nerve Impulse Notes To EbackpackPAMELA CASTILLONo ratings yet
- Cellular Components 2Document37 pagesCellular Components 2farzadcop1No ratings yet
- Tutorial Dr. SaugiDocument33 pagesTutorial Dr. SaugifemmytaniaNo ratings yet
- Lesson 18 - Orgasmic Disorder in The MaleDocument9 pagesLesson 18 - Orgasmic Disorder in The MaleJay JiangNo ratings yet
- 20230413083839Document2 pages20230413083839Jay JiangNo ratings yet
- ENT Competitveness - Concerns For Future 2015 - Kaplan PDFDocument3 pagesENT Competitveness - Concerns For Future 2015 - Kaplan PDFJay JiangNo ratings yet
- Author's Accepted Manuscript: 10.1016/j.urpr.2017.04.005Document23 pagesAuthor's Accepted Manuscript: 10.1016/j.urpr.2017.04.005Jay JiangNo ratings yet
- AUA Guideline On RUTI 10-12-22 FinalDocument44 pagesAUA Guideline On RUTI 10-12-22 FinalJay JiangNo ratings yet
- National Trends and Characteristics of Success in The Urology Match ProcessDocument6 pagesNational Trends and Characteristics of Success in The Urology Match ProcessJay JiangNo ratings yet
- EKGDocument31 pagesEKGJay JiangNo ratings yet
- Campbell Biology 12th Edition SummaryDocument6 pagesCampbell Biology 12th Edition Summaryprincesje05No ratings yet
- Notes Ankita KashyapDocument49 pagesNotes Ankita Kashyapkharsatikevin92No ratings yet
- Tort of NegligenceDocument10 pagesTort of NegligenceHETRAM SIYAGNo ratings yet
- TOAD Getting Started GuideDocument50 pagesTOAD Getting Started Guidesmruti_2012No ratings yet
- Joseph Kyle Neibert v. Computer Sciences Corporation, 11th Cir. (2015)Document20 pagesJoseph Kyle Neibert v. Computer Sciences Corporation, 11th Cir. (2015)Scribd Government DocsNo ratings yet
- Puri Brothers: Tax Type: ExemptedDocument66 pagesPuri Brothers: Tax Type: Exemptedmukesh puriNo ratings yet
- Snapshots of A Daughter in LawDocument2 pagesSnapshots of A Daughter in LawReshal AroraNo ratings yet
- Activity STSDocument1 pageActivity STSRalph ZeusNo ratings yet
- Chavara Brochure Edited CompressedDocument13 pagesChavara Brochure Edited CompressedShameer ShajiNo ratings yet
- METHODS OF TEACHING Lesson 1Document19 pagesMETHODS OF TEACHING Lesson 1Joey Bojo Tromes BolinasNo ratings yet
- Grumpy Bear: Some Questions ..Document2 pagesGrumpy Bear: Some Questions ..Mike BNo ratings yet
- Factors Responsible For Burnout Among College StudentsDocument7 pagesFactors Responsible For Burnout Among College StudentsRaj naveenNo ratings yet
- Billy Elliot EssayDocument2 pagesBilly Elliot Essayafabkgddu100% (1)
- Lifestyle Upper Intermediate CB 2012 177p PDFDocument177 pagesLifestyle Upper Intermediate CB 2012 177p PDFԿորյուն ՕհանյանNo ratings yet
- Storification - The Next Big Content Marketing Trend and 3 Benefits Marketers Shouldn't Miss Out OnDocument3 pagesStorification - The Next Big Content Marketing Trend and 3 Benefits Marketers Shouldn't Miss Out OnKetan JhaNo ratings yet
- Applied Economics Syllabus DeclassifiedDocument4 pagesApplied Economics Syllabus DeclassifiedAl Jay MejosNo ratings yet
- Ca. Bhagchand Chechani (Maheshwari)Document8 pagesCa. Bhagchand Chechani (Maheshwari)chechaniNo ratings yet
- Task 2Document4 pagesTask 2Gerardo LanzaNo ratings yet
- Glossary of Terms Relating To Signs and Symptoms: DictionaryDocument9 pagesGlossary of Terms Relating To Signs and Symptoms: DictionaryMishael Octaviany JirehNo ratings yet
- 08 Investmentquestfinal PDFDocument13 pages08 Investmentquestfinal PDFralphalonzo0% (1)
- Young - Coco Chanel Enseñanzas ModaDocument151 pagesYoung - Coco Chanel Enseñanzas ModaLuis Ángel Bejarano MaluquishNo ratings yet
- Aeco136 - Final Term Report (Manatal Multipurpose Cooperatives)Document20 pagesAeco136 - Final Term Report (Manatal Multipurpose Cooperatives)JoyDianneGumatayNo ratings yet
- 【拉图尔】临界区域:关键区域Critical ZonesDocument472 pages【拉图尔】临界区域:关键区域Critical Zoneszhang yanNo ratings yet
- Laguna Tayabas Bus Co V The Public Service CommissionDocument1 pageLaguna Tayabas Bus Co V The Public Service CommissionAnonymous byhgZINo ratings yet
- HR ManualDocument130 pagesHR Manualshikha khanejaNo ratings yet
- Research Design MBA MK02 UNIT IIDocument15 pagesResearch Design MBA MK02 UNIT IIAmit Kumar100% (3)