Download as pptx, pdf, or txt
You might also like
- PF2 S01-15 - The Blooming CatastropheDocument35 pagesPF2 S01-15 - The Blooming CatastropheJared PrestonNo ratings yet
- Advanced Pharmaceutical analysisFrom EverandAdvanced Pharmaceutical analysisRating: 4.5 out of 5 stars4.5/5 (2)
- Asamyutha Hastha - PicDocument4 pagesAsamyutha Hastha - PicGeethaAmidala100% (1)
- MOSHELL Commands v14Document91 pagesMOSHELL Commands v14AshishChadha100% (1)
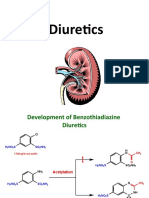
- Diuretics: Excretion of Water and ElectrolytesDocument33 pagesDiuretics: Excretion of Water and ElectrolytesSujeet SinghNo ratings yet
- Sulphonamides: Mr. Dharmendrasinh A BariaDocument20 pagesSulphonamides: Mr. Dharmendrasinh A BariaRaju NiraulaNo ratings yet
- DM pp81-104Document24 pagesDM pp81-104MLUNGISI MkhwanaziNo ratings yet
- Nama Ana Atika Surur NIM 18040011: Fenol 4-Metil FenolDocument8 pagesNama Ana Atika Surur NIM 18040011: Fenol 4-Metil FenolThata ThataNo ratings yet
- AminaDocument31 pagesAminaRedyNo ratings yet
- Sulpha DrugsDocument19 pagesSulpha DrugsPraveen T MNo ratings yet
- Amines, Reactions: Basic NucleophilicDocument37 pagesAmines, Reactions: Basic NucleophilicM. MoizNo ratings yet
- محاضره ٣Document28 pagesمحاضره ٣ecosystem200410myNo ratings yet
- Nisa Slide Icnp2015Document19 pagesNisa Slide Icnp2015Yun NikNo ratings yet
- Diuretics IIDocument14 pagesDiuretics IIأمجد محمدNo ratings yet
- Synthesis of MoleculesDocument25 pagesSynthesis of MoleculesAmit GohriNo ratings yet
- UntitledDocument36 pagesUntitledRida Aslam DHND ROLL NO 01No ratings yet
- DiureticDocument45 pagesDiureticHamdy Abdel-RahmanNo ratings yet
- Amides: in Amides, An Amino Group Replaces The - OH Group of Carboxylic AcidsDocument25 pagesAmides: in Amides, An Amino Group Replaces The - OH Group of Carboxylic AcidsByakuya BleachNo ratings yet
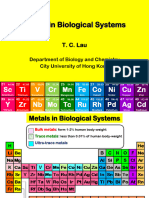
- Asset-V1 HKVU+COSAS+2021 Q4 R1+type@asset+block@metal-SeminarDocument37 pagesAsset-V1 HKVU+COSAS+2021 Q4 R1+type@asset+block@metal-Seminar1126playpubgNo ratings yet
- TutorialDocument27 pagesTutorialSiti NuraqidahNo ratings yet
- Sulfa Antibiotics Synthesis of SulfanilamideDocument10 pagesSulfa Antibiotics Synthesis of SulfanilamidePablo AguilarNo ratings yet
- 20 Reaction of AlcoholsDocument18 pages20 Reaction of AlcoholsHamid Hussain HamidNo ratings yet
- Benzene Synthesis Page 51-53Document3 pagesBenzene Synthesis Page 51-53Ung HhNo ratings yet
- Anthelmintics: DR - Amal Belaid 6Document24 pagesAnthelmintics: DR - Amal Belaid 6Mustafa RihanNo ratings yet
- NEPHAR 305 Metabolism - 12Document61 pagesNEPHAR 305 Metabolism - 12Ra'fat RaheemNo ratings yet
- P-IV U-1 Azodyes PDFDocument51 pagesP-IV U-1 Azodyes PDFdarshanNo ratings yet
- Chapter 13 Compound Contaning NitrogenDocument27 pagesChapter 13 Compound Contaning NitrogenTanvi ShahNo ratings yet
- SDF PDFDocument7 pagesSDF PDFdefender paintsNo ratings yet
- Article Chem Med ChemDocument37 pagesArticle Chem Med ChemgejaNo ratings yet
- Conversion 2080Document9 pagesConversion 2080Shashak MishraNo ratings yet
- DGT Organic Compounds C NitrogenDocument15 pagesDGT Organic Compounds C Nitrogensc5753972No ratings yet
- Descarboxilación Del PiruvatoDocument51 pagesDescarboxilación Del PiruvatoMajo CurtidorNo ratings yet
- Strecker Reaction and Its ApplicationsDocument14 pagesStrecker Reaction and Its ApplicationssairachudharyNo ratings yet
- Sandmeyer Isatin Synthesis 2010 PDFDocument4 pagesSandmeyer Isatin Synthesis 2010 PDFSamrat MazumdarNo ratings yet
- Lect. 7 Nitro CompoundsDocument13 pagesLect. 7 Nitro CompoundsAbdo HaiderNo ratings yet
- AminesDocument23 pagesAminesfhtzzzzzzNo ratings yet
- Acfrogcxqpd3dqml GQHMZQ B0c089di81vpcrvgphrwcu4gh Bzezvshldjt4clxztdrke4cieuxds1wlvk6scla 0byn2rmeu4btdaq8ckybm0chweegnztu7u2olcnli2lia5txmf386nyikuDocument6 pagesAcfrogcxqpd3dqml GQHMZQ B0c089di81vpcrvgphrwcu4gh Bzezvshldjt4clxztdrke4cieuxds1wlvk6scla 0byn2rmeu4btdaq8ckybm0chweegnztu7u2olcnli2lia5txmf386nyikuAchal ParekhNo ratings yet
- Document PDFDocument4 pagesDocument PDFzainNo ratings yet
- Synthesis and Antifungal Activity of Isatin-3-Semicarbazone: S.N. P, K T and S KDocument4 pagesSynthesis and Antifungal Activity of Isatin-3-Semicarbazone: S.N. P, K T and S KzainNo ratings yet
- Heter 0Document22 pagesHeter 0Lot AdewumilotNo ratings yet
- VitaminDocument32 pagesVitamingopal jhaNo ratings yet
- Crazy Groups For UdemyDocument1 pageCrazy Groups For UdemygabrielpoulsonNo ratings yet
- Urinary Tract Antiinfective AgentsDocument4 pagesUrinary Tract Antiinfective AgentsMaanvi SharmaNo ratings yet
- Ultraviolet-Visible Spectrophotometry: Submitted by Paritala Jagadeesh B.PharmDocument14 pagesUltraviolet-Visible Spectrophotometry: Submitted by Paritala Jagadeesh B.Pharmkavya nainitaNo ratings yet
- Antitubercular Agents: Mycobacterium Especially Mycobacterium Tuberculosis Which Is An Acid Fast AerobicDocument5 pagesAntitubercular Agents: Mycobacterium Especially Mycobacterium Tuberculosis Which Is An Acid Fast AerobicGopal JoshiNo ratings yet
- ReductionDocument36 pagesReductionSayed Newaj ChowdhuryNo ratings yet
- Punya FadamDocument1 pagePunya Fadam57-AdityaNo ratings yet
- PS 3 ContDocument3 pagesPS 3 ContDenisse Leonoras-PatersonNo ratings yet
- Nucleophilic SubstitutionDocument22 pagesNucleophilic Substitutionnishitagupta790No ratings yet
- CH CooDocument2 pagesCH CooPawan SharmaNo ratings yet
- Mines: NANO WWW - Online.nanoeducation - Co.inDocument33 pagesMines: NANO WWW - Online.nanoeducation - Co.inSajaNo ratings yet
- Tutorial-2 - Heterocycles Nomenclature-Part-IIDocument18 pagesTutorial-2 - Heterocycles Nomenclature-Part-IIamirNo ratings yet
- Methods For C-N Bond FormationDocument21 pagesMethods For C-N Bond FormationSudrajatNo ratings yet
- NONAROMATIC HETEROCYCLES Saturated Five Membered HeterocyclesDocument10 pagesNONAROMATIC HETEROCYCLES Saturated Five Membered Heterocyclesouc89571No ratings yet
- AnilineDocument21 pagesAnilineDr M K GuptaNo ratings yet
- 65b7901c061a0300189494ba - ## - Alcohols, Ethers and Phenols Short NotesDocument4 pages65b7901c061a0300189494ba - ## - Alcohols, Ethers and Phenols Short Notesdibyaprakash451No ratings yet
- Diazonium Salts, Azo DyesDocument8 pagesDiazonium Salts, Azo DyesDotsha Raheem100% (4)
- DiazepamDocument1 pageDiazepamRaaj TilakNo ratings yet
- Diazonium Salts Azo DyesDocument8 pagesDiazonium Salts Azo DyesAnthony Basanta100% (1)
- Matriculation Chemistry (Amino Acids) Part 2Document10 pagesMatriculation Chemistry (Amino Acids) Part 2ridwanNo ratings yet
- IŞIL IRMAK UZUNGEL-Methyl Orange-PhenolphthaleinDocument10 pagesIŞIL IRMAK UZUNGEL-Methyl Orange-PhenolphthaleinIrmak UzungelNo ratings yet
- KS0 Operation Manual-EN-V2.0Document19 pagesKS0 Operation Manual-EN-V2.0Freddie ChanNo ratings yet
- Identifying The Form of Digital Marketing Strategy Most Effective To Millennial's Brand PerceptionDocument16 pagesIdentifying The Form of Digital Marketing Strategy Most Effective To Millennial's Brand PerceptionElisabeth HenangerNo ratings yet
- Cargo Handling 5Document21 pagesCargo Handling 5LilCent MmanuelNo ratings yet
- Corrective Justice (PDFDrive) PDFDocument365 pagesCorrective Justice (PDFDrive) PDFAnonymous 94TBTBRksNo ratings yet
- Quarter1 WK 4 - WHLPLAN - ARLENE CATHERINE T. ASIA - 2021-2022Document12 pagesQuarter1 WK 4 - WHLPLAN - ARLENE CATHERINE T. ASIA - 2021-2022Bernard T. AsiaNo ratings yet
- Risk ManagementDocument60 pagesRisk ManagementarunapecNo ratings yet
- Daniel Gorenstein - The Classification of The Finite Simple Groups PDFDocument176 pagesDaniel Gorenstein - The Classification of The Finite Simple Groups PDFAnna Sabater100% (1)
- Komatsu Bulldozer D65ex PX 15 E0 Operation Maintenance ManualDocument20 pagesKomatsu Bulldozer D65ex PX 15 E0 Operation Maintenance Manualjulia100% (49)
- Ccts Maine Standards Rev 11 20Document11 pagesCcts Maine Standards Rev 11 20api-607068017No ratings yet
- EOU UNIT 11 - Đáp Án Eou 11Document8 pagesEOU UNIT 11 - Đáp Án Eou 11Trường Sơn NguyễnNo ratings yet
- Psychology 4th Edition Schacter Test BankDocument22 pagesPsychology 4th Edition Schacter Test BankWilliamBeckymce100% (43)
- Occupations: Lesson Plan Prathom 5Document11 pagesOccupations: Lesson Plan Prathom 5Raymond RainMan DizonNo ratings yet
- Pediatric Distal Radius FracturesDocument34 pagesPediatric Distal Radius FracturesRamzi ShukriNo ratings yet
- Course Application Form: Celta at Ih Bogotá: Cambridge Certificate ELT To AdultsDocument5 pagesCourse Application Form: Celta at Ih Bogotá: Cambridge Certificate ELT To AdultsAndrea Marcela Peña SegoviaNo ratings yet
- CSC 2105: D S I: ATA Tructure NtroductionDocument22 pagesCSC 2105: D S I: ATA Tructure NtroductionFahim AhmedNo ratings yet
- Wesleyan University-Philippines: Basic Education Department PahintulotDocument1 pageWesleyan University-Philippines: Basic Education Department Pahintulotthyme 02No ratings yet
- ISYE 530 Spring 2020 SyllabusDocument2 pagesISYE 530 Spring 2020 SyllabusswapnilNo ratings yet
- Relationship Between Diversity and Conflict Management Among Different OrganizationsDocument8 pagesRelationship Between Diversity and Conflict Management Among Different OrganizationsSajjad GulNo ratings yet
- STD 6 SSSV SST Hist CH 1 1st SemDocument2 pagesSTD 6 SSSV SST Hist CH 1 1st Sempurvesh2510No ratings yet
- Being A Team CaptainDocument6 pagesBeing A Team CaptainCoach OlsonNo ratings yet
- Vastushant - SamagriDocument6 pagesVastushant - Samagrirajeshjoshi23No ratings yet
- Voting System Using Face RecognitionDocument18 pagesVoting System Using Face RecognitionbalaNo ratings yet
- Children's WearDocument44 pagesChildren's Wearra s100% (1)
- Antazo Vs DobladaDocument6 pagesAntazo Vs DobladaCel C. CaintaNo ratings yet
- 3rd Simposium On SCCDocument11 pages3rd Simposium On SCCNuno FerreiraNo ratings yet
- Artificial Intelligence in 2019 Presentation by Chandravadan RautDocument72 pagesArtificial Intelligence in 2019 Presentation by Chandravadan RautChandravadan Raut100% (1)
- A A Chemistry Model Exam 2012Document13 pagesA A Chemistry Model Exam 2012Kerod MohamedNo ratings yet