Download as pptx, pdf, or txt
You might also like
- Shaukat Khanum Memorial Cancer Hospital & Research Centre: Endocrine PanelDocument1 pageShaukat Khanum Memorial Cancer Hospital & Research Centre: Endocrine PanelRehan Ahmad Baig0% (2)
- Tilt by Lambcullen COMPLETEDocument161 pagesTilt by Lambcullen COMPLETEjoni0127100% (1)
- Egg Heads AnalysisDocument5 pagesEgg Heads AnalysisAlex DaoNo ratings yet
- UTI - Concept MapDocument1 pageUTI - Concept MapZam Pamate50% (2)
- Uwise HYDocument3 pagesUwise HYJack GuccioneNo ratings yet
- Modeling and Prediction of Outcome For The Superovulation Stage in in Vitro Fertilization Jfiv.1000122Document8 pagesModeling and Prediction of Outcome For The Superovulation Stage in in Vitro Fertilization Jfiv.1000122Reni ReniNo ratings yet
- In-Vitro Fertilisation (Ivf) in Singapore: Charges and Success RatesDocument4 pagesIn-Vitro Fertilisation (Ivf) in Singapore: Charges and Success RatesLászló ÉvaNo ratings yet
- Treatment With Piroxicam Before Embryo Transfer Increases The Pregnancy Rate After in Vitro Fertilization and Embryo TransferDocument5 pagesTreatment With Piroxicam Before Embryo Transfer Increases The Pregnancy Rate After in Vitro Fertilization and Embryo TransferVasantham HospitalNo ratings yet
- Procedures and Techniques-Clinical: ArtDocument2 pagesProcedures and Techniques-Clinical: ArtGeos KarNo ratings yet
- 2019 IVF Fee Schedule: Points of ContactDocument9 pages2019 IVF Fee Schedule: Points of ContactamirNo ratings yet
- Fendo 14 1331640Document8 pagesFendo 14 1331640Muhammad Alim MajidNo ratings yet
- Ovary JumpingDocument4 pagesOvary JumpingTess SixNo ratings yet
- Best Ivf Clinic in The PhilippinesDocument14 pagesBest Ivf Clinic in The PhilippinesGeraldine CamannongNo ratings yet
- The Current Status of IVF Are We Putting The Needs of The 2023 EClinicalMedDocument2 pagesThe Current Status of IVF Are We Putting The Needs of The 2023 EClinicalMedronaldquezada038No ratings yet
- OVARIAN RESERVE DR NADDocument40 pagesOVARIAN RESERVE DR NADanindhita_vaniaNo ratings yet
- Ivf and Icsi Consent FormDocument10 pagesIvf and Icsi Consent FormSantosoNo ratings yet
- Bovine in Vitro Fertilization: in Vitro Oocyte Maturation and Sperm Capacitation With HeparinDocument2 pagesBovine in Vitro Fertilization: in Vitro Oocyte Maturation and Sperm Capacitation With HeparinCilica Marius DanielNo ratings yet
- In Vitro Fertilization Treatment in UdaipurDocument3 pagesIn Vitro Fertilization Treatment in Udaipurrkivf58No ratings yet
- Genetic and Phenotypic Parameters of Performance Traits in White Leghorn LayersDocument8 pagesGenetic and Phenotypic Parameters of Performance Traits in White Leghorn LayersTJPRC PublicationsNo ratings yet
- Infertilityivf Icsi 200409081730Document37 pagesInfertilityivf Icsi 200409081730Mohamed ElhelalyNo ratings yet
- Increased Risk of Preterm Birth and Low Birthweight With Very High Number of Oocytes Following IVFDocument8 pagesIncreased Risk of Preterm Birth and Low Birthweight With Very High Number of Oocytes Following IVFIsabelle EvrardNo ratings yet
- Pediatric Department, Pingtung Christian HospitalDocument41 pagesPediatric Department, Pingtung Christian Hospitalwawa chenNo ratings yet
- Optimizing The First-Line Fertility Treatment: Gynecological EndocrinologyDocument6 pagesOptimizing The First-Line Fertility Treatment: Gynecological EndocrinologyKarlin ReyesNo ratings yet
- FEMALE INFERTILITY (Autosaved)Document157 pagesFEMALE INFERTILITY (Autosaved)Cecilia CabanagNo ratings yet
- 10.preterm BirthDocument91 pages10.preterm BirthChayanika KumarNo ratings yet
- Assisted Hatching For in Vitro Fertilization-Embryo Transfer: An UpdateDocument3 pagesAssisted Hatching For in Vitro Fertilization-Embryo Transfer: An UpdateandriNo ratings yet
- Chausiaux 2011 EOGDocument3 pagesChausiaux 2011 EOGMFSNo ratings yet
- In Vitro Fertilization (IVF) : PresentationDocument25 pagesIn Vitro Fertilization (IVF) : PresentationAnshul RanaNo ratings yet
- Pi Is 0015028216620101Document1 pagePi Is 0015028216620101GayathriMaranNo ratings yet
- Sperm Morphology of Domestic Animals J H Koziol Full Chapter PDFDocument69 pagesSperm Morphology of Domestic Animals J H Koziol Full Chapter PDFgjekijabele100% (6)
- Understanding IVF Success Rates and Legal Recourses For MisrepresentationDocument4 pagesUnderstanding IVF Success Rates and Legal Recourses For MisrepresentationAinur 'iin' RahmahNo ratings yet
- IVF RelatedDocument1 pageIVF RelatedMeera Al AliNo ratings yet
- Vitamin D and PCOSDocument39 pagesVitamin D and PCOSsyafiraNo ratings yet
- Sperm Morphology of Domestic Animals J H Koziol All ChapterDocument67 pagesSperm Morphology of Domestic Animals J H Koziol All Chapterglenn.price788100% (6)
- Samper2010 Artificial Insemination EquineDocument5 pagesSamper2010 Artificial Insemination EquineSandra TaboadaNo ratings yet
- Management of Recurrent Pregnancy LossDocument29 pagesManagement of Recurrent Pregnancy Lossshilpi sumanNo ratings yet
- Unique Scientific Publishers: Animal Health PerspectivesDocument7 pagesUnique Scientific Publishers: Animal Health Perspectivesbou rihaneNo ratings yet
- In Vitro FertilizationDocument11 pagesIn Vitro FertilizationCeeNo ratings yet
- Oocyte Cryopreservation: DR Astha Gupta Consultant Reproductive MedicineDocument26 pagesOocyte Cryopreservation: DR Astha Gupta Consultant Reproductive MedicineDrAstha GuptaNo ratings yet
- Hansen Genetics and Fertility Torreon 2007Document37 pagesHansen Genetics and Fertility Torreon 2007Zavala H IrvingNo ratings yet
- 1 s2.0 S0093691X24000372 MainDocument5 pages1 s2.0 S0093691X24000372 Mainmincuandrada10No ratings yet
- ART 2015 Clinic Report Tables ID NY PDFDocument177 pagesART 2015 Clinic Report Tables ID NY PDFmeltwithsnow163.comNo ratings yet
- Cervical Ripening & Induction of Labour: Obstetric Guideline 1Document10 pagesCervical Ripening & Induction of Labour: Obstetric Guideline 1Maizura Syahirah MohtadaNo ratings yet
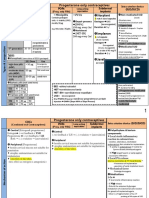
- Overview of Family Planning MethodsDocument30 pagesOverview of Family Planning Methodsganapa247No ratings yet
- Midwest Center For Reproductive Health IVF Fresh - Frozen HandbookDocument141 pagesMidwest Center For Reproductive Health IVF Fresh - Frozen Handbookandi hamatajNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument5 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologySri HariNo ratings yet
- Comparison of Live Birth Rate in Ivf Patients With Severe Oats and Normozoospermic in Male Factor InfertilityDocument4 pagesComparison of Live Birth Rate in Ivf Patients With Severe Oats and Normozoospermic in Male Factor InfertilityIJAR JOURNALNo ratings yet
- Treatment Strategy for Unexplained Infertility and Recurrent MiscarriageFrom EverandTreatment Strategy for Unexplained Infertility and Recurrent MiscarriageKeiji KurodaNo ratings yet
- Preterm Labor: Evidence Based ViewDocument68 pagesPreterm Labor: Evidence Based ViewAmmar FardhanaNo ratings yet
- Alcântara Neto Et Al., 2020.2 (Oviduct Fluid Extrecellular Vesicles Regulate Polyspermy During Porcine in Vitro Fertilization)Document10 pagesAlcântara Neto Et Al., 2020.2 (Oviduct Fluid Extrecellular Vesicles Regulate Polyspermy During Porcine in Vitro Fertilization)asanetoNo ratings yet
- Pi Is 0015028209011005Document6 pagesPi Is 0015028209011005Meli AnaNo ratings yet
- Thin Endometrium: Dr. Astha Gupta Senior Ivf and Infertility Consultant Milann Fertility, DelhiDocument56 pagesThin Endometrium: Dr. Astha Gupta Senior Ivf and Infertility Consultant Milann Fertility, DelhiDrAstha Gupta100% (2)
- PT-1-IN-SCIENCE (1) .OdtDocument14 pagesPT-1-IN-SCIENCE (1) .OdtJhersy CentenoNo ratings yet
- Improving Reproductive EfficiencyDocument16 pagesImproving Reproductive EfficiencyNitty MafefaNo ratings yet
- YA-Baruselli 2021Document16 pagesYA-Baruselli 2021Sofi Albertini WeilerNo ratings yet
- 1 s2.0 S0301211523003202 main (科研通 ablesci.com)Document28 pages1 s2.0 S0301211523003202 main (科研通 ablesci.com)Carlos ParraNo ratings yet
- Artificial Insemination and Semen HandlingDocument124 pagesArtificial Insemination and Semen HandlingADUGNA DEGEFENo ratings yet
- Ojog 2018041214473648Document10 pagesOjog 2018041214473648RiniNo ratings yet
- Raja EA-2022Document12 pagesRaja EA-2022HAVIZ YUADNo ratings yet
- Recent Studies On Nutritional Factors Affecting Reproductive Efficiency in US Dairy HerdsDocument13 pagesRecent Studies On Nutritional Factors Affecting Reproductive Efficiency in US Dairy HerdsfrankyNo ratings yet
- Lecture 10 Repeat Breeding in Cattle and BuffaloDocument37 pagesLecture 10 Repeat Breeding in Cattle and BuffalognpobsNo ratings yet
- Effect of Myo-Inositol and Melatonin Versus Myoinositol in A Randomized Controlled TrialDocument6 pagesEffect of Myo-Inositol and Melatonin Versus Myoinositol in A Randomized Controlled TriallizandrobNo ratings yet
- Ivf and EconomyDocument17 pagesIvf and EconomyPooja vidhyasagarNo ratings yet
- Tocomin SupraBio - Hair Growth StudyDocument6 pagesTocomin SupraBio - Hair Growth StudyjassenNo ratings yet
- High - Risk PregnancyDocument110 pagesHigh - Risk PregnancyAndre DityaNo ratings yet
- Module 8 Uts Quiz ReviewerDocument4 pagesModule 8 Uts Quiz ReviewerCHARLES LUIGI MESANo ratings yet
- Placental HormonesDocument16 pagesPlacental HormonesSajid Aziz SamoNo ratings yet
- AIIMS Paper2004Document14 pagesAIIMS Paper2004dhavalb20No ratings yet
- Biology AssignmentDocument21 pagesBiology AssignmentKenardNo ratings yet
- Alliance For Family Foundation vs. GarinDocument2 pagesAlliance For Family Foundation vs. GarinMaphile Mae Canencia100% (1)
- Sex Writing AssignmentDocument6 pagesSex Writing AssignmentFrank0% (1)
- Abortion and Ethics 2155 9627 1000291Document2 pagesAbortion and Ethics 2155 9627 1000291niluh100% (1)
- Module 2 Sexual SelfDocument16 pagesModule 2 Sexual SelfTinay Ledesma GepetacioNo ratings yet
- Reproductive System Powerpoint LectureDocument55 pagesReproductive System Powerpoint LectureJames DaurayNo ratings yet
- Barrier MethodDocument3 pagesBarrier MethodJaninaPatriciaBNo ratings yet
- Terapi Progesteron Pada Kehamilan, Bukti Atau Tradisi (1-10) - Noroyono WibowoDocument40 pagesTerapi Progesteron Pada Kehamilan, Bukti Atau Tradisi (1-10) - Noroyono WibowoAvicena M IqbalNo ratings yet
- Research ReferencesDocument47 pagesResearch ReferencesVaishali SinghNo ratings yet
- Insect Reproduction CK Dash SAUDocument3 pagesInsect Reproduction CK Dash SAUChandra Kanta Dash100% (1)
- Position Paper New Rh971Document2 pagesPosition Paper New Rh971David DueñasNo ratings yet
- Family Welfare Program & Population PolicyDocument56 pagesFamily Welfare Program & Population PolicyNirmalya SinhaNo ratings yet
- Rhetoric AnalysisDocument4 pagesRhetoric Analysisapi-2460354490% (1)
- mg1 Video ScriptDocument3 pagesmg1 Video Scriptapi-441877801No ratings yet
- PCOS DR BasimaDocument18 pagesPCOS DR BasimaA.H.ANo ratings yet
- Behavioral EcologyDocument17 pagesBehavioral Ecologyenigmaticmind23No ratings yet
- TCN Quiz 5Document3 pagesTCN Quiz 5erven aranasNo ratings yet
- 1st Lecture On The Histology of Female Reproductive System by Dr. RoomiDocument17 pages1st Lecture On The Histology of Female Reproductive System by Dr. RoomiMudassar RoomiNo ratings yet
- Norplant: Progesterone Only ContraceptivesDocument9 pagesNorplant: Progesterone Only ContraceptivesFathy ElsheshtawyNo ratings yet
- Chapter 42: Pediatric and Adolescent Gynecology Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument3 pagesChapter 42: Pediatric and Adolescent Gynecology Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- Group 1 Physical and Sexual SelfDocument80 pagesGroup 1 Physical and Sexual SelfMarc Eric GuerreroNo ratings yet
- Reproductive Technologies WorksheetDocument5 pagesReproductive Technologies WorksheetRobinHoodCookiesNo ratings yet