Download as pptx, pdf, or txt
You might also like
- Radiographic Evaluation in Hip and Knee Replacement - HNRDocument29 pagesRadiographic Evaluation in Hip and Knee Replacement - HNRSri MahadhanaNo ratings yet
- Risk Assessment - Tower DecommissioningDocument5 pagesRisk Assessment - Tower DecommissioningJeffery Mulei100% (1)
- Ankle FractureDocument87 pagesAnkle FractureStar Cruise100% (1)
- TKA Total Knee ARTHROPLASTY Replacement Conf 2Document96 pagesTKA Total Knee ARTHROPLASTY Replacement Conf 2haminatrafNo ratings yet
- Alingment in TKRDocument3 pagesAlingment in TKRdeepak100% (1)
- Primary Hip Arthroplasty Templating On Standard Radiographs A Stepwise ApproachDocument31 pagesPrimary Hip Arthroplasty Templating On Standard Radiographs A Stepwise ApproachMarius Chirila100% (1)
- Biomechanics of The KneeDocument8 pagesBiomechanics of The KneeJorge LopezNo ratings yet
- Correction of Foot Deformities With Ilizarov Methodology. Nuno Craveiro LopesDocument50 pagesCorrection of Foot Deformities With Ilizarov Methodology. Nuno Craveiro LopesNuno Craveiro LopesNo ratings yet
- 1-Prof DR Anees Biomechanics of HipDocument63 pages1-Prof DR Anees Biomechanics of HipAhmed M3tmdNo ratings yet
- Foot and Ankle Fractures2Document56 pagesFoot and Ankle Fractures2Ortho songoNo ratings yet
- Malunions of FracturesDocument56 pagesMalunions of FracturesDian FahmiNo ratings yet
- Osteotomies About The KneeDocument29 pagesOsteotomies About The KneeChetan PrakashNo ratings yet
- Biomechanicsofthecervicalspine 150120000612 Conversion Gate02Document62 pagesBiomechanicsofthecervicalspine 150120000612 Conversion Gate02marceloNo ratings yet
- Hip & Knee BookDocument33 pagesHip & Knee BookPrabath ChinthakaNo ratings yet
- Total Knee Arthroplasty PrinciplesDocument40 pagesTotal Knee Arthroplasty PrinciplesMitri NassarNo ratings yet
- Anatomy and Bio Mechanics of The KneeDocument15 pagesAnatomy and Bio Mechanics of The KneeaimanshalpyNo ratings yet
- Hindfoot Valgus: AP Talocalcaneal Angle (Kite's Angle)Document4 pagesHindfoot Valgus: AP Talocalcaneal Angle (Kite's Angle)JoaoNo ratings yet
- Presented By: DR Venkatesh V Moderator: DR Harish KDocument81 pagesPresented By: DR Venkatesh V Moderator: DR Harish KPankaj VatsaNo ratings yet
- Closing Wedge Osteotomy of The Tibia and The FemurDocument12 pagesClosing Wedge Osteotomy of The Tibia and The Femuralyek92No ratings yet
- Arthroscopic Anterior Cruciate Ligament Repair Single Bundle Double BundleDocument116 pagesArthroscopic Anterior Cruciate Ligament Repair Single Bundle Double BundleCipriana PetrutaNo ratings yet
- Surgical Technique For Combined D Wyer Calcaneal Osteotomy and PeronealDocument6 pagesSurgical Technique For Combined D Wyer Calcaneal Osteotomy and PeronealleahbayNo ratings yet
- Treatment of Diaphyseal Femoral Fractures With Ilizarov Frame. Maurizio A. Catagni and Francesco GuerreschiDocument4 pagesTreatment of Diaphyseal Femoral Fractures With Ilizarov Frame. Maurizio A. Catagni and Francesco GuerreschiNuno Craveiro LopesNo ratings yet
- Upload Scribd 3Document5 pagesUpload Scribd 3Yoga AninditaNo ratings yet
- Ortho Xray MeasurmentsDocument110 pagesOrtho Xray MeasurmentsPriza RazunipNo ratings yet
- Chapter 21: Surgery of The Congenital FootDocument30 pagesChapter 21: Surgery of The Congenital FootpoddataNo ratings yet
- Cubitus Varus, Elbow Joint, Mitali JoshiDocument13 pagesCubitus Varus, Elbow Joint, Mitali JoshiKapil Lakhwara100% (1)
- Lower Extremities and Pelvic Girlde PositioningDocument128 pagesLower Extremities and Pelvic Girlde Positioningcorrainnejimenez.24No ratings yet
- Pre Op PlanningDocument15 pagesPre Op PlanningRahul ReddyNo ratings yet
- Wagner 2021Document17 pagesWagner 2021Biblioteca Centro Médico De Mar del PlataNo ratings yet
- Knee Complex: 1: BiomechanicsDocument33 pagesKnee Complex: 1: BiomechanicsMichael SelvarajNo ratings yet
- AmputationDocument49 pagesAmputationJohn Paul Q.GallerosNo ratings yet
- Triple Arthrodesis: DR Chirag Patel Department of Orthopaedics ST Stephen's HospitalDocument41 pagesTriple Arthrodesis: DR Chirag Patel Department of Orthopaedics ST Stephen's HospitalImam SulemanNo ratings yet
- Femoroacetabular Impingement: DR Sandeep SinghDocument33 pagesFemoroacetabular Impingement: DR Sandeep Singhsandy singhNo ratings yet
- AmputationDocument23 pagesAmputationFloriza de LeonNo ratings yet
- TKA Total Knee ARTHROPLASTY Replacement TKR Conf 5Document245 pagesTKA Total Knee ARTHROPLASTY Replacement TKR Conf 5haminatrafNo ratings yet
- Arvee AnkleDocument50 pagesArvee AnkleDesing RajNo ratings yet
- Osteotomiesaroundthehip-160203173448 2Document134 pagesOsteotomiesaroundthehip-160203173448 2Felix SabuNo ratings yet
- Biomechanics of ArthroplastyDocument57 pagesBiomechanics of ArthroplastyUsama RafiqNo ratings yet
- 11 The Knee Floren Tri Fifah Done YeyyyDocument22 pages11 The Knee Floren Tri Fifah Done YeyyyFlorensia GladiesNo ratings yet
- 11 The Knee Floren Tri FifahDocument9 pages11 The Knee Floren Tri FifahFlorensia GladiesNo ratings yet
- Levels of AmputationsDocument6 pagesLevels of AmputationsJuanitoCabatañaLimIII100% (1)
- Robotic Unicondylar PlanningDocument17 pagesRobotic Unicondylar PlanningSuvodipBhattacharyaNo ratings yet
- Operative Techniques in Orthopaedic Surgery - 2nd - Distal Chevron OsteotomyDocument15 pagesOperative Techniques in Orthopaedic Surgery - 2nd - Distal Chevron OsteotomyakaandykayNo ratings yet
- New Doc 04-06-2020 12.16.36Document6 pagesNew Doc 04-06-2020 12.16.36Amir IqbalNo ratings yet
- Naik, S. - Biomechanics of Knee ComplexDocument25 pagesNaik, S. - Biomechanics of Knee ComplexKyle Bois100% (4)
- Spinal Osteotomies PDFDocument3 pagesSpinal Osteotomies PDFbandil deepanshuNo ratings yet
- Face Bows and Articulators PDFDocument30 pagesFace Bows and Articulators PDFggNo ratings yet
- Ankle Fractures: Winda Alviranisa/20204010293 Pembimbing: Dr. Muhammad Pandu Nugraha, SP - OTDocument28 pagesAnkle Fractures: Winda Alviranisa/20204010293 Pembimbing: Dr. Muhammad Pandu Nugraha, SP - OTwinda alviraNo ratings yet
- MSK CT Protocols Overview, Jan 2018Document26 pagesMSK CT Protocols Overview, Jan 2018grergergr grregrgrebNo ratings yet
- Patella Fracture: Mahmoud Ashour Orthopedic ResidentDocument23 pagesPatella Fracture: Mahmoud Ashour Orthopedic ResidentMohammed ahmedNo ratings yet
- Journal of Orthopaedic Surgery and ResearchDocument6 pagesJournal of Orthopaedic Surgery and ResearchDewye SartikaNo ratings yet
- Impact of Patellofemoral Design On Patellofemoral Forces and Polyethylene StressesDocument29 pagesImpact of Patellofemoral Design On Patellofemoral Forces and Polyethylene StressesupulerandaNo ratings yet
- Sport Traumatology-III Knee Complex-7Document24 pagesSport Traumatology-III Knee Complex-7kamran aliNo ratings yet
- 10 1016@j Jos 2016 04 015Document7 pages10 1016@j Jos 2016 04 015osmann52No ratings yet
- Osteotomiesaroundthehip 160203173448Document130 pagesOsteotomiesaroundthehip 160203173448Mit ParikhNo ratings yet
- Hip Complex BioDocument18 pagesHip Complex BioVijay PradeepNo ratings yet
- Does Use of A Variable Distal Femur Resection Angle Improve Radiographic Alignment in Primary Total Knee ArthroplastyDocument6 pagesDoes Use of A Variable Distal Femur Resection Angle Improve Radiographic Alignment in Primary Total Knee ArthroplastyAsmed El SalugNo ratings yet
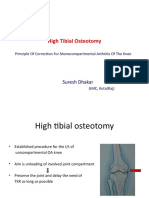
- High Tibial Osteotomy: Suresh DhakarDocument40 pagesHigh Tibial Osteotomy: Suresh DhakarAtul PandeyNo ratings yet
- Prosthetic Knee Joints: Dot IiDocument49 pagesProsthetic Knee Joints: Dot IiAlfred JacksonNo ratings yet
- Musculoskeletal Ultrasound for the Orthopaedic Surgeon OR, ER and Clinic, Volume 2From EverandMusculoskeletal Ultrasound for the Orthopaedic Surgeon OR, ER and Clinic, Volume 2No ratings yet
- The Natural Rotator Cuff Healing Guide: Heal Your Cuff, Rid the Pain All On Your Own With Natural ExercisesFrom EverandThe Natural Rotator Cuff Healing Guide: Heal Your Cuff, Rid the Pain All On Your Own With Natural ExercisesRating: 5 out of 5 stars5/5 (1)
- Willy Halim, MD, PHD, Fipp Anesthesiologist-Pain PractitionerDocument93 pagesWilly Halim, MD, PHD, Fipp Anesthesiologist-Pain PractitionerDManestesi cokicokiNo ratings yet
- Lesson 1o Head MusclesDocument19 pagesLesson 1o Head MusclesAdam LallanaNo ratings yet
- Anatomy Guidelines (Faisal Baloch)Document17 pagesAnatomy Guidelines (Faisal Baloch)zahraNo ratings yet
- Cervical Spine RotationDocument2 pagesCervical Spine RotationBaiq AnnisyaNo ratings yet
- PDF Anatomy of The Voice An Illustrated Guide For Singers Vocal Coaches and Speech Therapists Theodore Dimon Ebook Full ChapterDocument63 pagesPDF Anatomy of The Voice An Illustrated Guide For Singers Vocal Coaches and Speech Therapists Theodore Dimon Ebook Full Chapterkaren.johnson335100% (4)
- Shoulder Dystocia: Incidence, Mechanisms, and Management StrategiesDocument10 pagesShoulder Dystocia: Incidence, Mechanisms, and Management Strategiesfarida nur ainiNo ratings yet
- Mri of The Knee and Common PathologiesDocument73 pagesMri of The Knee and Common PathologiesTHESSNAVARRO100% (3)
- Anaesthesia and Acute Spinal Cord Injury: Philippa Veale BSC Mbbs Frca Joanne Lamb Mbbs FrcaDocument5 pagesAnaesthesia and Acute Spinal Cord Injury: Philippa Veale BSC Mbbs Frca Joanne Lamb Mbbs FrcaRoy Wicaksono TambunanNo ratings yet
- Stretching/Flexibility Exercises: Torso Stretch Purpose: Starting Position: ActionDocument3 pagesStretching/Flexibility Exercises: Torso Stretch Purpose: Starting Position: ActionDragisaNo ratings yet
- 09 Quiz 1-TaroDocument2 pages09 Quiz 1-TaroJosielyn TarsNo ratings yet
- Management of Acute Trauma: Samuel P. Carmichael II, Nathan T. Mowery, R. Shayn Martin, J. Wayne MeredithDocument43 pagesManagement of Acute Trauma: Samuel P. Carmichael II, Nathan T. Mowery, R. Shayn Martin, J. Wayne Meredithsportillag1No ratings yet
- Lawsuit Filed Against Surfside Beach Police Department and A Police SergantDocument8 pagesLawsuit Filed Against Surfside Beach Police Department and A Police SergantWMBF NewsNo ratings yet
- An Orthopedic Treatment That Involves Placing On A Limb, Bone or Muscle Group Using Variety ofDocument22 pagesAn Orthopedic Treatment That Involves Placing On A Limb, Bone or Muscle Group Using Variety oflemuel_que100% (2)
- Muscular System 20222023Document29 pagesMuscular System 20222023Danny Mel ManglaylayNo ratings yet
- Yoga Handbook 2023Document38 pagesYoga Handbook 2023Vijay BhaskarNo ratings yet
- Tendon and Ligament Healing: A New Approach Through Manual TherapyDocument1 pageTendon and Ligament Healing: A New Approach Through Manual TherapyMichael SelvarajNo ratings yet
- Body Regions WS AnswersDocument2 pagesBody Regions WS Answerssamba33% (3)
- Novus Actus InterveniensDocument15 pagesNovus Actus InterveniensA Prem '1010'No ratings yet
- Hierarchy of Organization: Associated SLODocument10 pagesHierarchy of Organization: Associated SLOZainne Sarip BandingNo ratings yet
- Gross HSB A - Axillary RegionDocument3 pagesGross HSB A - Axillary RegionAngelo BautistaNo ratings yet
- Standard Operating Procedure Versi InggrisDocument3 pagesStandard Operating Procedure Versi InggrisAmelia Nurul H50% (2)
- AAOS 2018 Foot and Ankle - by KhawajaDocument108 pagesAAOS 2018 Foot and Ankle - by KhawajaChristopherLawrenceNo ratings yet
- Trial PropositionDocument25 pagesTrial Propositionalexanot godNo ratings yet
- Full Download PDF of (Ebook PDF) Human Osteology 3rd Edition All ChapterDocument43 pagesFull Download PDF of (Ebook PDF) Human Osteology 3rd Edition All Chaptercelavituckx70100% (5)
- Martial Arts - Stretching - WorkoutDocument5 pagesMartial Arts - Stretching - WorkoutSPARTA100% (1)
- Neck TrainingDocument7 pagesNeck TrainingchampsNo ratings yet
- Abdullah, Hisham P. Article 262 MutilationDocument33 pagesAbdullah, Hisham P. Article 262 MutilationHisham AbdullahNo ratings yet
- RTS Automatic Transfer Switch - Technical Manual - GENERAC PDFDocument28 pagesRTS Automatic Transfer Switch - Technical Manual - GENERAC PDFpevare100% (2)
- Chapter 9Document62 pagesChapter 9Francisco GaniNo ratings yet