Download as pptx, pdf, or txt
You might also like
- Unexpected Joy at Dawn - Docx AnalysisDocument8 pagesUnexpected Joy at Dawn - Docx AnalysisBasil Ekwenye100% (1)
- Urine Analysis PracticalDocument53 pagesUrine Analysis PracticalMubasharAbrar100% (3)
- Abnormal Constituents of Urine Interpretation PracticalDocument42 pagesAbnormal Constituents of Urine Interpretation PracticalTEJASWI ModiNo ratings yet
- Mbbs 2k23 Aim - To Identify The Abnormal Constitutes of UrineDocument22 pagesMbbs 2k23 Aim - To Identify The Abnormal Constitutes of Urine8harshul8No ratings yet
- Analysis of Abnormal UrineDocument12 pagesAnalysis of Abnormal Urinesingonstrings365No ratings yet
- Urine AnalysisDocument41 pagesUrine AnalysisAjay SomeshwarNo ratings yet
- Urinalysis (Part-2) Constituents of Urine: AbnormalDocument49 pagesUrinalysis (Part-2) Constituents of Urine: AbnormalArnab GhoshNo ratings yet
- Urine AnalysisDocument42 pagesUrine AnalysisajaysomNo ratings yet
- Abnormal Constituents of Urine - 1Document5 pagesAbnormal Constituents of Urine - 1kalpithareddynomulaNo ratings yet
- 1 - GueDocument24 pages1 - GueQasmNo ratings yet
- Urine Analysis: Dr. Janani MathialaganDocument67 pagesUrine Analysis: Dr. Janani MathialaganGunjan sahuNo ratings yet
- Renal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesDocument44 pagesRenal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesajaysomNo ratings yet
- Analysis of Abnormal Constituents of Urine - 16th December 2019Document28 pagesAnalysis of Abnormal Constituents of Urine - 16th December 2019mubashirNo ratings yet
- Rine Analysis: Dr. Ola Samir Ziara Modified by Dr. Amal Al MaqadmaDocument39 pagesRine Analysis: Dr. Ola Samir Ziara Modified by Dr. Amal Al Maqadmaiman zainuddin100% (1)
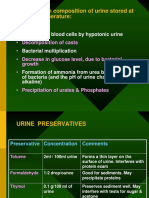
- Changes in Composition of Urine Stored at Room TemperatureDocument39 pagesChanges in Composition of Urine Stored at Room TemperatureAjay SomeshwarNo ratings yet
- Urinalysis PDFDocument56 pagesUrinalysis PDFTio AjhaNo ratings yet
- Formation of Urine: NephronDocument44 pagesFormation of Urine: NephronajaysomNo ratings yet
- Urine ComponentsDocument31 pagesUrine ComponentsLarry MagwegweNo ratings yet
- UrinalysisDocument3 pagesUrinalysisKim MoranoNo ratings yet
- UrinalysisDocument67 pagesUrinalysisumairzafar5261No ratings yet
- بايو عملي م١Document5 pagesبايو عملي م١tm31880388No ratings yet
- Glomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsDocument45 pagesGlomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsajaysomNo ratings yet
- Glomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsDocument42 pagesGlomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsajaysomNo ratings yet
- Urine AnalysisDocument33 pagesUrine AnalysisajaysomNo ratings yet
- Urine JSJ EoDocument9 pagesUrine JSJ EokeiNo ratings yet
- Urine-Analysis 140420Document74 pagesUrine-Analysis 140420sabao kizuiteNo ratings yet
- Urine AnalysisDocument31 pagesUrine AnalysisajaysomNo ratings yet
- Urine Examination New-1Document81 pagesUrine Examination New-1H GondaliyaNo ratings yet
- Urine ChemDocument38 pagesUrine ChemDr MurariNo ratings yet
- 2.physical ch. urine د.هناديDocument22 pages2.physical ch. urine د.هناديAbdulmalik Al-harthyNo ratings yet
- Urine Examination# DivyaDocument69 pagesUrine Examination# DivyaMedicine 0786No ratings yet
- Urine Analysis FinalDocument112 pagesUrine Analysis FinalNischita JayarajNo ratings yet
- Urinalysis 1 - 2Document25 pagesUrinalysis 1 - 2ahmadhasham86No ratings yet
- Renal Function TestsDocument31 pagesRenal Function TestsPhysiology by Dr RaghuveerNo ratings yet
- Analysis of Abnormal Urine NotesDocument6 pagesAnalysis of Abnormal Urine Notesahteshammirji575No ratings yet
- Characteristics of UrineDocument32 pagesCharacteristics of UrineMEGHANA GOSWAMINo ratings yet
- Term III Practical FileDocument31 pagesTerm III Practical FileShivam kumarNo ratings yet
- Experiment No. 3 Chemical Examination of UrineDocument7 pagesExperiment No. 3 Chemical Examination of UrineShanzayNo ratings yet
- Abnormal Constituents of UrineDocument18 pagesAbnormal Constituents of UrinesaswatsovitNo ratings yet
- Physical Characteristics of UrineDocument36 pagesPhysical Characteristics of Urinemuhammad saad100% (1)
- URINALYSISDocument80 pagesURINALYSISredr7131No ratings yet
- Urine Examination & Analysis: Assigned By: DR - Javeria Khan Presented By: DR - Noor-ul-Ain SarwarDocument123 pagesUrine Examination & Analysis: Assigned By: DR - Javeria Khan Presented By: DR - Noor-ul-Ain SarwarErenjaeger TitanNo ratings yet
- Clinical Microscopy - MTDocument200 pagesClinical Microscopy - MTJihrus Mendoza100% (1)
- Chemical Examination of UrineDocument46 pagesChemical Examination of UrineH GondaliyaNo ratings yet
- Theory 10 - Lipid Profile - Electrolytes Part 2Document71 pagesTheory 10 - Lipid Profile - Electrolytes Part 2Navoda ThathsaraniNo ratings yet
- Interpretasi Urine RutinDocument118 pagesInterpretasi Urine Rutinboy jendri huluNo ratings yet
- Urine AnalysisDocument98 pagesUrine AnalysisLucia SurduNo ratings yet
- Investigations in Renal DiseaseDocument32 pagesInvestigations in Renal Diseaseadamu mohammadNo ratings yet
- Rta Final Year 23.2.23Document36 pagesRta Final Year 23.2.23S.ayesh HasanNo ratings yet
- 1.6.5.4c - URINALISISDocument30 pages1.6.5.4c - URINALISISBilqis ElfariantiNo ratings yet
- Qualitative Analysis of Normal and Abnormal UrineDocument28 pagesQualitative Analysis of Normal and Abnormal UrineVirendra JoshiNo ratings yet
- 4 BodyDocument35 pages4 Bodysinte beyuNo ratings yet
- Fluid Therapy Cases VZSDocument36 pagesFluid Therapy Cases VZSbiankaNo ratings yet
- Renal FABS ONLINE RefresherDocument69 pagesRenal FABS ONLINE RefresherAu CassieNo ratings yet
- Chem Lect Unit 7 Kidney FunctionDocument38 pagesChem Lect Unit 7 Kidney FunctionMustafa KhandgawiNo ratings yet
- Urine Analysis: Sbmitted To:dr - Jayganeesh Asst - Professor Dept - of Modern Diagnosis Submitted By:manisha Nandan 3 Year BNYSDocument30 pagesUrine Analysis: Sbmitted To:dr - Jayganeesh Asst - Professor Dept - of Modern Diagnosis Submitted By:manisha Nandan 3 Year BNYSMeera NandanNo ratings yet
- Odour: Physical ExaminationDocument27 pagesOdour: Physical ExaminationajaysomNo ratings yet
- Urine AnalysisDocument53 pagesUrine AnalysisMaath KhalidNo ratings yet
- Urinalysis 150313040235 Conversion Gate01Document30 pagesUrinalysis 150313040235 Conversion Gate01AbhishiktaAbhi100% (1)
- Biochemistry of Urine: By: Jerome S. Montano, RMTDocument28 pagesBiochemistry of Urine: By: Jerome S. Montano, RMTAhuNo ratings yet
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- Key Issues ReflectionDocument7 pagesKey Issues ReflectionLee SuarezNo ratings yet
- Api 575Document37 pagesApi 575Sakthi Pk100% (3)
- AGC 2022 R4 QP Class 5.412e46feDocument1 pageAGC 2022 R4 QP Class 5.412e46fereachsricharanvasireddyNo ratings yet
- Implen Smart Grid ColombiaDocument6 pagesImplen Smart Grid ColombiapabloNo ratings yet
- Dokumen 2Document1 pageDokumen 2Balamurugan HNo ratings yet
- Sugar Beet Ref BookDocument108 pagesSugar Beet Ref Bookdpaciura3388No ratings yet
- मजदुर २०७७-११-५ बर्ष २३ अंक २६Document8 pagesमजदुर २०७७-११-५ बर्ष २३ अंक २६Ganga DahalNo ratings yet
- IT Week1Document11 pagesIT Week1Mustafa AdilNo ratings yet
- Die Bosch ABS The World's First System For Closed-Loop Control of Vehicle DynamicsDocument27 pagesDie Bosch ABS The World's First System For Closed-Loop Control of Vehicle DynamicsMamdouhAlhanafy100% (1)
- Krebs Cycle: TCA/ Citric Acid CycleDocument24 pagesKrebs Cycle: TCA/ Citric Acid Cyclejahanzeb aliNo ratings yet
- Module in Earth and Life Science: Levels of Organization of Living ThingsDocument20 pagesModule in Earth and Life Science: Levels of Organization of Living ThingsAna Kristelle Grace SyNo ratings yet
- The Safety Culture Stack - The Next Evolution of Safety Culture?Document19 pagesThe Safety Culture Stack - The Next Evolution of Safety Culture?Deisy QuevedoNo ratings yet
- Science Q 3 3wk 5 - 3Document3 pagesScience Q 3 3wk 5 - 3Junior FelipzNo ratings yet
- APA Format For Annotated Bibliographies: Updated For 5th EditionDocument3 pagesAPA Format For Annotated Bibliographies: Updated For 5th EditionSafat Al Mamun RonoNo ratings yet
- Refrigeration P&ID)Document3 pagesRefrigeration P&ID)ratheesh0% (1)
- Passage Planning - Sharjah To Abu Dhabi 13 July 2010Document4 pagesPassage Planning - Sharjah To Abu Dhabi 13 July 2010Kunal Singh100% (2)
- Canopius Reinsurance AG Financial Condition Report 2018Document50 pagesCanopius Reinsurance AG Financial Condition Report 2018saxobobNo ratings yet
- Co2 04Document16 pagesCo2 04Poojitha BondalapatiNo ratings yet
- Lab - Fossil EvidenceDocument3 pagesLab - Fossil Evidenceapi-223694170No ratings yet
- Lost Links and Mid Air Collisions-The Problems With Domestic DronesDocument105 pagesLost Links and Mid Air Collisions-The Problems With Domestic DronesEyemanProphetNo ratings yet
- P6 Science SA1 2017 Rosyth Exam PapersDocument40 pagesP6 Science SA1 2017 Rosyth Exam PapersKui LiuNo ratings yet
- Thin Layer Chromatography (TLC) PDFDocument11 pagesThin Layer Chromatography (TLC) PDFValeriaCusumanoNo ratings yet
- Chapter 5, David Besanko Microeconomics. Assignment2.KobraDocument6 pagesChapter 5, David Besanko Microeconomics. Assignment2.KobrabaqirNo ratings yet
- Territorial Patterns and Relations in HungaryDocument31 pagesTerritorial Patterns and Relations in HungarymrrwhoNo ratings yet
- Solid Shape Pro 10Document71 pagesSolid Shape Pro 10Lukman Tarigan SumatraNo ratings yet
- CX200 Sales Spec Sheet (Euro 5) R09Document2 pagesCX200 Sales Spec Sheet (Euro 5) R09RobertNo ratings yet
- Designing and Implementing A Datawarehousing (Step1) : Chapter-4Document8 pagesDesigning and Implementing A Datawarehousing (Step1) : Chapter-4Mohamoud Farah Abdilahi AliNo ratings yet
- Muscle-Building Cookbook - Lose Fat, Build Muscle - Ovs To Help You Get The Body You Want - Nancy SilvermanDocument75 pagesMuscle-Building Cookbook - Lose Fat, Build Muscle - Ovs To Help You Get The Body You Want - Nancy Silvermanscribd2100% (1)
- Airway PositioningDocument34 pagesAirway PositioningAsep PurnomosidiNo ratings yet