Download as pptx, pdf, or txt
You might also like
- Want Will Won't List PDFDocument12 pagesWant Will Won't List PDFjoku jokunen100% (2)
- Lesson Plan On MenopauseDocument16 pagesLesson Plan On MenopauseRavina Patel100% (6)
- 2nd Quarter Summative Test Science 5Document3 pages2nd Quarter Summative Test Science 5Summer R. Dominguez100% (2)
- Infections of Female Genital TractDocument67 pagesInfections of Female Genital TractSana AftabNo ratings yet
- Syndromic Management of Sexually Transmitted InfectionsDocument76 pagesSyndromic Management of Sexually Transmitted Infectionsnamita100% (2)
- Business Communication Building Critical Skills 6th Edition Locker Test BankDocument34 pagesBusiness Communication Building Critical Skills 6th Edition Locker Test Bankrubepazuqo88% (8)
- CDC, 2006 Prof. Aboubakr ElnasharDocument25 pagesCDC, 2006 Prof. Aboubakr Elnasharkhadzx100% (2)
- Lower Genital Tract Infections & Sexually Transmitted DiseasesDocument38 pagesLower Genital Tract Infections & Sexually Transmitted Diseasesraed faisalNo ratings yet
- A. Tunica Albuguinea: NCM 102: Assessment ExamDocument9 pagesA. Tunica Albuguinea: NCM 102: Assessment ExamdubhieNo ratings yet
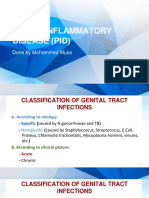
- Pelvic Inflammatory DiseaseDocument25 pagesPelvic Inflammatory DiseasedeepaNo ratings yet
- Cervicitis Infection: N. Gonorrhea C. TrachomatisDocument5 pagesCervicitis Infection: N. Gonorrhea C. TrachomatisMiguel MansillaNo ratings yet
- Lec.12 Genital Tract Infection (Part 1)Document26 pagesLec.12 Genital Tract Infection (Part 1)شريف محمد حسين شريف يوسفNo ratings yet
- Genital Infections: Assoc Prof Suna KABİL KUCURDocument41 pagesGenital Infections: Assoc Prof Suna KABİL KUCURasdNo ratings yet
- Infections in OB/GYN: Vaginitis, STI'sDocument52 pagesInfections in OB/GYN: Vaginitis, STI'sMiftahurrahmah GmsNo ratings yet
- Genital Tract Infections: Xu Jian Xuj@zju - Edu.cnDocument70 pagesGenital Tract Infections: Xu Jian Xuj@zju - Edu.cnAygulNo ratings yet
- Lower Genital Tract InfectionDocument51 pagesLower Genital Tract InfectionSarisa SupawimonNo ratings yet
- VaginitisDocument27 pagesVaginitisdrtancerNo ratings yet
- Pelvic Inflammatory Disease (PID)Document16 pagesPelvic Inflammatory Disease (PID)CHRISTIAN RAY ALPAS PASILIAONo ratings yet
- Bacterial VaginosisDocument4 pagesBacterial VaginosisjoycesiosonNo ratings yet
- Sexually Transmitted Infections and PregnancyDocument19 pagesSexually Transmitted Infections and PregnancyBeyins TiuNo ratings yet
- Vulvovaginal Infections, Cervicitis and Bartholin's Cyst: Suparna Chhibber, MDDocument44 pagesVulvovaginal Infections, Cervicitis and Bartholin's Cyst: Suparna Chhibber, MDTeguh Imana NugrahaNo ratings yet
- Leukorrhea, STDS, HIV Infection.13032018 PDFDocument128 pagesLeukorrhea, STDS, HIV Infection.13032018 PDFrujiraNo ratings yet
- 12 Lower Female Genital Tract InfectionsDocument42 pages12 Lower Female Genital Tract InfectionsAwal Sher khanNo ratings yet
- Vaginal Infections Update: Original ReviewDocument6 pagesVaginal Infections Update: Original ReviewEpi PanjaitanNo ratings yet
- Cervicitis and VaginitisDocument18 pagesCervicitis and VaginitisAqua ForceNo ratings yet
- Pid13032018 PDFDocument50 pagesPid13032018 PDFrujiraNo ratings yet
- 54.vaginal DischargeDocument40 pages54.vaginal DischargebenNo ratings yet
- Obstetrics GynacologyDocument19 pagesObstetrics GynacologyAhmad SobihNo ratings yet
- Genital Tract InfectionsDocument4 pagesGenital Tract Infectionsmed.progressNo ratings yet
- 9- Abnormal Vaginal DischargeDocument29 pages9- Abnormal Vaginal DischargeBlind DlawarNo ratings yet
- Alaa PrometricDocument67 pagesAlaa PrometricqasimNo ratings yet
- MGT of STIDocument53 pagesMGT of STIhasefa136No ratings yet
- Bacterial VaginosisDocument20 pagesBacterial VaginosisTum M. TansakulNo ratings yet
- Practical Guide To Diagnosing and Treating Vaginitis (Medscape)Document16 pagesPractical Guide To Diagnosing and Treating Vaginitis (Medscape)Nur Ilmi SofiahNo ratings yet
- Gyn Revalida Review CSL 2 2017Document101 pagesGyn Revalida Review CSL 2 2017Mara Medina - BorleoNo ratings yet
- HIVAIDS and PregnancyDocument44 pagesHIVAIDS and PregnancyAnastasiafynnNo ratings yet
- 8.sti 2Document44 pages8.sti 2Mahrukh SiddiquiNo ratings yet
- Office and Laboratory ManagementDocument8 pagesOffice and Laboratory ManagementEman BayoumiNo ratings yet
- Gyne - (Section B) PID-STI-1Document45 pagesGyne - (Section B) PID-STI-1Kailash KhatriNo ratings yet
- PID PresentationDocument23 pagesPID Presentationakankiza.lucky83No ratings yet
- Vulvovaginitis: by James Holencik, DODocument70 pagesVulvovaginitis: by James Holencik, DOSyarifa YuliaNo ratings yet
- A Clinical Conundrum - Chronic CervicitisDocument3 pagesA Clinical Conundrum - Chronic CervicitisRanna HertenizaNo ratings yet
- K10 - ISK AtasDocument39 pagesK10 - ISK AtasfelixNo ratings yet
- Genital Tract InfectionDocument96 pagesGenital Tract InfectiondhitaapriliaNo ratings yet
- PID LectureDocument41 pagesPID LectureHarold Gabriel Sanchez DelgadoNo ratings yet
- Sexually Transmitted DiseaseDocument3 pagesSexually Transmitted DiseaseBrianna ValerioNo ratings yet
- Infections of The Upper Genital TractDocument40 pagesInfections of The Upper Genital TractBernard Palarca SantosNo ratings yet
- STIs O & GDocument59 pagesSTIs O & GNoraNo ratings yet
- By. Dr. Wondifraw ADocument30 pagesBy. Dr. Wondifraw ASebliNo ratings yet
- Pelvic Inflammatory Disease: Bibo Yuan M.D.,PH.DDocument51 pagesPelvic Inflammatory Disease: Bibo Yuan M.D.,PH.DNorman AjxNo ratings yet
- Descarga VaginalDocument8 pagesDescarga VaginalMELVYN HAROLD CHAVEZ MAURICIONo ratings yet
- RPS Penyakit KelaminDocument133 pagesRPS Penyakit KelaminArdana WindriyaNo ratings yet
- Slide 1 STIDocument50 pagesSlide 1 STIMatth N. ErejerNo ratings yet
- Pid 180131145647 1Document41 pagesPid 180131145647 1Smriti GroverNo ratings yet
- LUPALS Sexual Health and Contraception QuizDocument107 pagesLUPALS Sexual Health and Contraception QuizShan PatelNo ratings yet
- Duh Tubuh Wanita, DR SAYU.,SpKK, WMDocument62 pagesDuh Tubuh Wanita, DR SAYU.,SpKK, WMdickypranataNo ratings yet
- Pelvic Inflammatory DiseaseDocument34 pagesPelvic Inflammatory DiseaseOhunakin AfolabiNo ratings yet
- Rep 1Document50 pagesRep 1bbbbbvvvvv1No ratings yet
- Pelvic Inflammatory DiseaseDocument43 pagesPelvic Inflammatory DiseaseFauzia Jamiri - Abdurasid100% (2)
- Infeksi Saluran Kemih: Oleh Hendra Santoso Pembimbing Dr. Hasnawaty SP - OGDocument22 pagesInfeksi Saluran Kemih: Oleh Hendra Santoso Pembimbing Dr. Hasnawaty SP - OGHendra SantosoNo ratings yet
- Vaginitis and Vaginal DischargeDocument52 pagesVaginitis and Vaginal Dischargedrdoaabakhet148No ratings yet
- MAX Vaginal Panel WhitepaperDocument8 pagesMAX Vaginal Panel WhitepaperDevi OktaviannyNo ratings yet
- Lower Genital Tract Precancer: Colposcopy, Pathology and TreatmentFrom EverandLower Genital Tract Precancer: Colposcopy, Pathology and TreatmentNo ratings yet
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Abnormal Uterine Bleeding MCQDocument8 pagesAbnormal Uterine Bleeding MCQCommunity Round3 G1100% (1)
- 3 2 Human Reproductive SystemDocument38 pages3 2 Human Reproductive SystemMarcStep De GuzmanNo ratings yet
- Reproductive System MMDocument1 pageReproductive System MMKhaled Abdel-saterNo ratings yet
- Benign Neoplasms of The Genital 2Document22 pagesBenign Neoplasms of The Genital 2ugonna nwokeNo ratings yet
- 1341-Article Text-4651-2-10-20211223Document7 pages1341-Article Text-4651-2-10-20211223Alwiyah amd. kebNo ratings yet
- HypopediasisDocument8 pagesHypopediasisv_vijayakanth7656No ratings yet
- Evaluation of The Infertility CoupleDocument19 pagesEvaluation of The Infertility Coupleapi-3705046No ratings yet
- 4 - Hormonal ContraceptivesDocument109 pages4 - Hormonal ContraceptivesNoskcire OremorNo ratings yet
- Femalereproductiveorgan 150117083020 Conversion Gate01Document57 pagesFemalereproductiveorgan 150117083020 Conversion Gate01SARABIA, ARVIN JR.No ratings yet
- Artificial Insemination: TypesDocument3 pagesArtificial Insemination: Typessagi muNo ratings yet
- Summative Test Q2 - Week 1Document5 pagesSummative Test Q2 - Week 1Beverly CuyaNo ratings yet
- EAU Guidelines On Sexual and Reproductive Health 2022Document292 pagesEAU Guidelines On Sexual and Reproductive Health 2022Melqart bazino100% (1)
- A Case Study About Cervical PolypsDocument8 pagesA Case Study About Cervical PolypsJisel-Apple BulanNo ratings yet
- (REVALIDA) OB-REVALIDA-Gyne-Topics-Crash-CourseDocument11 pages(REVALIDA) OB-REVALIDA-Gyne-Topics-Crash-CourseAlexa Lorenzo CiprianoNo ratings yet
- Las Science 5 Melc 1 q2 Week1Document10 pagesLas Science 5 Melc 1 q2 Week1Marjun BartoloNo ratings yet
- Growing Up OkDocument44 pagesGrowing Up OkKhamiddinov OyatilloNo ratings yet
- Gender Identity Disorder Not Otherwise SpecifiedDocument4 pagesGender Identity Disorder Not Otherwise SpecifiedJona AddatuNo ratings yet
- Vulva Vagina Uterus - MODIFIED PDFDocument141 pagesVulva Vagina Uterus - MODIFIED PDFBatool SherbiniNo ratings yet
- Course Information For Current Semester/Term: Maklumat Kursus Untuk Semester/Penggal SemasaDocument5 pagesCourse Information For Current Semester/Term: Maklumat Kursus Untuk Semester/Penggal SemasaNurul IrhamnaNo ratings yet
- Angel Moon - Bad End - Chapter 2Document1 pageAngel Moon - Bad End - Chapter 2GarNo ratings yet
- Munce y 2021Document11 pagesMunce y 2021Your Imaginary StarNo ratings yet
- Katerero KunyazaDocument6 pagesKaterero KunyazaPeter Kamala100% (1)
- GynaecologyDocument123 pagesGynaecologyKiranNo ratings yet
- Study Guide For Introduction To Maternity and Pediatric Nursing 5th Edition Leifer Test BankDocument36 pagesStudy Guide For Introduction To Maternity and Pediatric Nursing 5th Edition Leifer Test Banknephriteprimelyqihx100% (26)
- Aim4aiims - In: 30-GynecologyDocument13 pagesAim4aiims - In: 30-GynecologyAnwaar YousafNo ratings yet
- Female Reproductive SystemDocument14 pagesFemale Reproductive SystemChintan Chavda100% (1)