Download as pptx, pdf, or txt
You might also like
- Unit 05: Data Preparation & AnalysisDocument26 pagesUnit 05: Data Preparation & AnalysisTanya Malviya100% (1)
- Somatic TherapiesDocument170 pagesSomatic TherapiesDelyn Gamutan Millan100% (2)
- Pharmacology SGL 1 Introduction To The Pharmacology of CNS DrugsDocument28 pagesPharmacology SGL 1 Introduction To The Pharmacology of CNS DrugsNwa BradostNo ratings yet
- CNS StimulantsDocument89 pagesCNS StimulantsMwanja Moses100% (1)
- Introduction To Cns PharmacologyDocument66 pagesIntroduction To Cns PharmacologyYazan Emad Salem100% (1)
- Ans Drugs Pharmacology.Document81 pagesAns Drugs Pharmacology.SAMUEL - NGUNJIRINo ratings yet
- Cholinergic ReceptorsDocument50 pagesCholinergic ReceptorsAnkita GuravNo ratings yet
- Cns Trans & Drug DetoxificationDocument57 pagesCns Trans & Drug DetoxificationAlvin LaurenceNo ratings yet
- Central Nervous System StimulantsDocument20 pagesCentral Nervous System StimulantsAn LoNo ratings yet
- Pharmacology of Mood Stabilizers: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanDocument51 pagesPharmacology of Mood Stabilizers: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanFansisca SiallaganNo ratings yet
- Cns Pharmacology For Pc-IIDocument135 pagesCns Pharmacology For Pc-IItinsaeworkineh976No ratings yet
- Aashish Parihar Lecturer College of Nursing AIIMS, JodhpurDocument101 pagesAashish Parihar Lecturer College of Nursing AIIMS, JodhpurHardeep KaurNo ratings yet
- Drug Abuse, Dependence, AddictionDocument36 pagesDrug Abuse, Dependence, AddictionIan100% (1)
- Recent Advances in Understanding and Management of Benzodiazepine, Cannabinoids & Tobacco DependenceDocument54 pagesRecent Advances in Understanding and Management of Benzodiazepine, Cannabinoids & Tobacco Dependencestpeter_agraNo ratings yet
- Drugs Acting On CVS-2014Document36 pagesDrugs Acting On CVS-2014كسلان اكتب اسميNo ratings yet
- Drugs of DependencyDocument13 pagesDrugs of Dependencybrianmuthomi851No ratings yet
- Adjuvant Analgesics: Oxford American Pain LibraryDocument29 pagesAdjuvant Analgesics: Oxford American Pain LibraryRey AlwiwikhNo ratings yet
- Lecture 27 - 3rd Asessment - CNS IntroductionDocument31 pagesLecture 27 - 3rd Asessment - CNS Introductionapi-3703352100% (1)
- Toxicology: by Group 4 2018/2019 Tan Geok Eng Reena DewiDocument59 pagesToxicology: by Group 4 2018/2019 Tan Geok Eng Reena DewiTan Geok EngNo ratings yet
- 2016 Pharmacology of Sedative-HypnoticDocument46 pages2016 Pharmacology of Sedative-HypnoticFansisca SiallaganNo ratings yet
- Pharmacology Neurotropic Drugs 2015Document44 pagesPharmacology Neurotropic Drugs 2015Migz BrosasNo ratings yet
- Introduction Classification Benzodiazepines BarbituratesDocument15 pagesIntroduction Classification Benzodiazepines BarbituratesVijetha RaiNo ratings yet
- General AnestDocument35 pagesGeneral AnestMauz AshrafNo ratings yet
- Cns StimulantsDocument41 pagesCns StimulantsYIKI ISAACNo ratings yet
- CNS Stimulants 2023Document10 pagesCNS Stimulants 2023ManWol JangNo ratings yet
- Drugs That Affect Cardiovascular SystemDocument35 pagesDrugs That Affect Cardiovascular Systems.khan9211rediffmail.comNo ratings yet
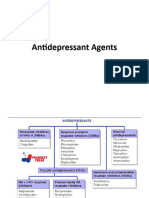
- Antidepressant AgentsDocument45 pagesAntidepressant Agentsmadeha goharNo ratings yet
- Central Nervous System Agents: Carmencita R. Pacis PHD, ManDocument52 pagesCentral Nervous System Agents: Carmencita R. Pacis PHD, ManTWINNY JOSSANNE CHEERISHANE MINIONNo ratings yet
- Sympatholytic AgentsDocument17 pagesSympatholytic AgentsofficialdanieladejumoNo ratings yet
- Farmacologia Das Drogas Ansiolà TicasDocument65 pagesFarmacologia Das Drogas Ansiolà TicasEduarda StumpfNo ratings yet
- EMOS Farmacología I Sesion 17Document22 pagesEMOS Farmacología I Sesion 17rafaelNo ratings yet
- SedativeDocument35 pagesSedativeking_goldNo ratings yet
- 4.alpa 2 AgonistsDocument44 pages4.alpa 2 AgonistsAstha ShresthaNo ratings yet
- New Developments in Cannabinoid-Based MedicineDocument14 pagesNew Developments in Cannabinoid-Based MedicineJaime AriasNo ratings yet
- CNS Depressants Oleh Dr. BramDocument124 pagesCNS Depressants Oleh Dr. BramAlvian JohanesNo ratings yet
- Anxiolytic DrugsDocument60 pagesAnxiolytic Drugsneleh grayNo ratings yet
- 2 - CNS Stimulant PDFDocument38 pages2 - CNS Stimulant PDFZaid HaiderNo ratings yet
- Introduction To CNS PharmacologyDocument22 pagesIntroduction To CNS PharmacologyTamiru KetemaNo ratings yet
- Adrenergic and NonadrenergicDocument49 pagesAdrenergic and Nonadrenergicsweta sumanNo ratings yet
- Cannabinoids and The Expanded Endocannabinoid System in Neurological DisordersDocument21 pagesCannabinoids and The Expanded Endocannabinoid System in Neurological DisordersKaren SánchezNo ratings yet
- Psychopharmacological AgentsDocument44 pagesPsychopharmacological Agentsbazet49No ratings yet
- Treatment For Mental Health IssuesDocument43 pagesTreatment For Mental Health Issuessang Nguyen DuongNo ratings yet
- The Adrenergic DrugsDocument25 pagesThe Adrenergic DrugsBareera NudratNo ratings yet
- Conscious Sedation: Hayel Gharaibeh, MD. Anesthesia ConsultantDocument84 pagesConscious Sedation: Hayel Gharaibeh, MD. Anesthesia ConsultantKhaled GharaibehNo ratings yet
- AntidepresentDocument34 pagesAntidepresentmariaNo ratings yet
- Antianxiety SedativeDocument44 pagesAntianxiety Sedativemohsen mirdamadiNo ratings yet
- Medical Marijuana PresentationDocument19 pagesMedical Marijuana Presentationsudheer vamarajuNo ratings yet
- Anxiety Disorders OutlineDocument25 pagesAnxiety Disorders OutlineCrystal MarloweNo ratings yet
- Pharmacology of CannabisDocument39 pagesPharmacology of CannabisJessiCaddell-HunsuckerNo ratings yet
- CNS Depressants: - Sedatives and Hypnotics - General Anesthetics - Narcotic AnalgesicsDocument118 pagesCNS Depressants: - Sedatives and Hypnotics - General Anesthetics - Narcotic Analgesicsbiruk getahunNo ratings yet
- Drugs Acting On The Autonomic Nervous SystemDocument21 pagesDrugs Acting On The Autonomic Nervous SystemyewollolijfikreNo ratings yet
- Ans Pharmacology 01 For Pc-IDocument54 pagesAns Pharmacology 01 For Pc-ITsegaye HailuNo ratings yet
- Drugs in Psychiatric NursingDocument38 pagesDrugs in Psychiatric NursingJSeasharkNo ratings yet
- Sedative - HypnoticsDocument62 pagesSedative - HypnoticsvijayNo ratings yet
- Antidepressants (ME216) 20 5Document40 pagesAntidepressants (ME216) 20 5Dineish MurugaiahNo ratings yet
- AntipsychoticsDocument47 pagesAntipsychoticsammar_ahmed_19No ratings yet
- Adrenergic Agonist and AntagonistDocument35 pagesAdrenergic Agonist and AntagonistFirjat AfiataNo ratings yet
- Anesthetic Agents Ga/La: Rabindra AdhikaryDocument40 pagesAnesthetic Agents Ga/La: Rabindra AdhikaryAnaliza Kitongan LantayanNo ratings yet
- ANXIOLYTICSDocument33 pagesANXIOLYTICSCletus MichaelNo ratings yet
- Sedative-Hypnotic DrugsDocument30 pagesSedative-Hypnotic DrugsdrfatimarizNo ratings yet
- Surgical Packs and ToolsDocument37 pagesSurgical Packs and Toolsstartizo001No ratings yet
- Theatre TechniqueDocument85 pagesTheatre Techniquestartizo001No ratings yet
- 1 BurnsDocument79 pages1 Burnsstartizo001No ratings yet
- Burn Injury 3Document56 pagesBurn Injury 3startizo001No ratings yet
- Everest Group PEAK Matrix™ For Healthcare Analytics Service ProvidersDocument15 pagesEverest Group PEAK Matrix™ For Healthcare Analytics Service ProvidersArnab100% (1)
- Succession Planning ReportDocument19 pagesSuccession Planning ReportSana Khan100% (3)
- Statistics For Economics Formula Sheet.Document38 pagesStatistics For Economics Formula Sheet.VivekNo ratings yet
- Flexible Classroom Assessment Activity Mechanism FCAAMDocument2 pagesFlexible Classroom Assessment Activity Mechanism FCAAMJay Jexter Selda50% (2)
- Unit 1 - ActividadesDocument9 pagesUnit 1 - ActividadesJoey MontanaNo ratings yet
- Inferno Fury ManualDocument6 pagesInferno Fury ManualJohn BurgerNo ratings yet
- Home Construction Cost Calculator - UltraTechDocument4 pagesHome Construction Cost Calculator - UltraTechKrishnareddy K.R.No ratings yet
- 1-11 бжб ,тжб баллDocument1 page1-11 бжб ,тжб баллГаухар АбильдаеваNo ratings yet
- Demand AnalysisDocument100 pagesDemand AnalysisSheikh Yajidul100% (1)
- Effect of Vacuum Packaging-Mcb FinalDocument18 pagesEffect of Vacuum Packaging-Mcb FinalIam Eilsen ObiasNo ratings yet
- Microsoft 365 - Mfa (13655)Document11 pagesMicrosoft 365 - Mfa (13655)Nioro FuriscalNo ratings yet
- PRC ApplicationDocument1 pagePRC ApplicationJericho CabungcalNo ratings yet
- Firearm TestDocument4 pagesFirearm TestAndrew Mateo de Acosta100% (1)
- SSS Clutch ProjectDocument4 pagesSSS Clutch ProjectMoustafa HelmyNo ratings yet
- Clearfrac Co2 SchlumbergerDocument2 pagesClearfrac Co2 SchlumbergerSohaibSeidNo ratings yet
- APRO Banking Gateway For Oracle Financials CloudDocument2 pagesAPRO Banking Gateway For Oracle Financials Cloudsohaibmuzaffar007No ratings yet
- BSI Marketing Code of PracticeDocument14 pagesBSI Marketing Code of PracticeAgung Dian WintaraNo ratings yet
- OM1 Chapter 2: Competitiveness, Strategy, and ProductivityDocument1 pageOM1 Chapter 2: Competitiveness, Strategy, and ProductivityRoseanne Binayao LontianNo ratings yet
- KTI Fajar Al Afghani Pengaruh Iradiasi Gamma Terhadap KrisanDocument6 pagesKTI Fajar Al Afghani Pengaruh Iradiasi Gamma Terhadap KrisanFajar Al AfghaniNo ratings yet
- Apparel Export Promotion Council, Gurgaon: TH THDocument6 pagesApparel Export Promotion Council, Gurgaon: TH THbatman arunNo ratings yet
- Realistic HTX-100 Mobile Transceiver: Care and Maintenance Features Installation Operation Specifications TroubleshootingDocument21 pagesRealistic HTX-100 Mobile Transceiver: Care and Maintenance Features Installation Operation Specifications TroubleshootingkadottNo ratings yet
- Course Title: Financial Management Course Code: FIBA601 Credit Units: 3Document3 pagesCourse Title: Financial Management Course Code: FIBA601 Credit Units: 3Mannat BhallaNo ratings yet
- Powercrete DD: Product Data SheetDocument2 pagesPowercrete DD: Product Data SheetFernando Ytozu TairaNo ratings yet
- List of PPN Hospitals in AhmedabadDocument10 pagesList of PPN Hospitals in Ahmedabadrambitcrip senguntharNo ratings yet
- Poker Cheat Sheet: by ViaDocument2 pagesPoker Cheat Sheet: by ViamaolpNo ratings yet
- The National Competency-Based Teacher StandardsDocument7 pagesThe National Competency-Based Teacher StandardsJacquelyn MendozaNo ratings yet
- OOP SE-203: Submitted By: - ANUJ 2K20/SE/21 - Anurag Munshi 2K20/Se/25Document9 pagesOOP SE-203: Submitted By: - ANUJ 2K20/SE/21 - Anurag Munshi 2K20/Se/25Anurag Munshi 25No ratings yet
- 08cDocument78 pages08cDan FarrisNo ratings yet
- Export DocumentationDocument54 pagesExport DocumentationmaninderwazirNo ratings yet