Download as ppt, pdf, or txt
You might also like
- ExamPreview RN 111722Document148 pagesExamPreview RN 111722jhajj0% (3)
- Nursing Students Peritonitis Care PlanDocument2 pagesNursing Students Peritonitis Care PlanJide Manuel100% (1)
- Haad Questions (2018)Document54 pagesHaad Questions (2018)SAHYA TRADCO100% (1)
- 15 Principles of Management and Prevention of Odontogenic inDocument24 pages15 Principles of Management and Prevention of Odontogenic inVukasin VostinicNo ratings yet
- Vital SignsDocument24 pagesVital SignsQuennie Marie Moreno VillanuevaNo ratings yet
- 3 - Vital SignDocument27 pages3 - Vital SignBav VAansoqnuaetzNo ratings yet
- Pemeriksaan Tanda Vital-Kuliah PengantarDocument22 pagesPemeriksaan Tanda Vital-Kuliah PengantarDwitia IswariNo ratings yet
- Vital Signs SabansiDocument116 pagesVital Signs SabansiTariku olanaNo ratings yet
- Vital Signs LectureDocument67 pagesVital Signs LectureJayrelle D. SafranNo ratings yet
- (1a) Vital - Signs BSNDocument63 pages(1a) Vital - Signs BSNYounas PandaNo ratings yet
- Vital Signs (Blood Pressure) : Jacqueline M. Calaycay, RN, MSNDocument14 pagesVital Signs (Blood Pressure) : Jacqueline M. Calaycay, RN, MSNJacq CalaycayNo ratings yet
- FundaDocument5 pagesFundaGreggy Francisco LaraNo ratings yet
- Nurs 201Document3 pagesNurs 201Nadia SolohNo ratings yet
- Vital Sign Na (1) by ZWBDocument52 pagesVital Sign Na (1) by ZWBAshraf Ali100% (1)
- Cned Handbook Single Page1 1Document40 pagesCned Handbook Single Page1 1api-300218860No ratings yet
- Physical DiagnosisDocument42 pagesPhysical DiagnosisKhim Yalong100% (1)
- Cardiovascular AssessmentDocument73 pagesCardiovascular AssessmentmatthewsarfrazbhattiNo ratings yet
- General Survey AssessmentDocument56 pagesGeneral Survey Assessmentdanny_ng080% (1)
- VITAL SIGNS LECTUREDocument5 pagesVITAL SIGNS LECTUREchdxemailNo ratings yet
- Cardiovascular Assessment (1) - StudentsDocument70 pagesCardiovascular Assessment (1) - Studentsraima ayazNo ratings yet
- BHC RevDocument14 pagesBHC RevShaine CababatNo ratings yet
- Cot 1 Vital SignsDocument22 pagesCot 1 Vital Signscristine g. magatNo ratings yet
- Vital SignDocument100 pagesVital SignIbnu FuqonNo ratings yet
- Vital-Signs (Quiz Nalang Kulang)Document51 pagesVital-Signs (Quiz Nalang Kulang)Hannah TollenoNo ratings yet
- Lect9 CirculatoryDocument81 pagesLect9 CirculatoryTuTitNo ratings yet
- Assessment: General Survey, Measurement, Vital SignsDocument10 pagesAssessment: General Survey, Measurement, Vital SignsNathan BarrerasNo ratings yet
- VitalsDocument34 pagesVitalsMoffat MoseNo ratings yet
- Vital-Signs 042951Document37 pagesVital-Signs 042951alyssaburgos02No ratings yet
- Vital SignDocument100 pagesVital SignZubda ButtNo ratings yet
- Vital Signs or Cardinal SignsDocument5 pagesVital Signs or Cardinal SignsMadelaine Mary Rose GarciaNo ratings yet
- Vital SignDocument100 pagesVital SignMj EncinaNo ratings yet
- Assessment of CvsDocument70 pagesAssessment of CvsTouseeq ManzoorNo ratings yet
- Practical Nursing Diploma Program Nursing Skills Lab 1: Blood Pressure Week 12Document21 pagesPractical Nursing Diploma Program Nursing Skills Lab 1: Blood Pressure Week 12Taryn CorbettNo ratings yet
- Vital SignsDocument69 pagesVital SignsSamantha SunglaoNo ratings yet
- Signos VitalesDocument5 pagesSignos VitalesAndrea Correa OrtegaNo ratings yet
- Blood PressureDocument18 pagesBlood PressureChelsea BorgoniaNo ratings yet
- Demo On Vital SignsDocument5 pagesDemo On Vital SignsLawrence Cada Nofies100% (3)
- Lab Manual Physiology II Lab HPP 1104Document32 pagesLab Manual Physiology II Lab HPP 1104yuvrajsingh6966No ratings yet
- Vital SignsDocument10 pagesVital SignsEdelou Alegria JumawanNo ratings yet
- Physical ExaminationDocument32 pagesPhysical ExaminationCaroline AgathaNo ratings yet
- 4. VITAL SIGNSDocument56 pages4. VITAL SIGNSmwabalogilenisileNo ratings yet
- Clinical Procedures For Medical AssistantDocument40 pagesClinical Procedures For Medical AssistantStudent1010No ratings yet
- Vitals ObservationsDocument52 pagesVitals ObservationsletticianabunyaNo ratings yet
- NSTP12 FinalDocument16 pagesNSTP12 FinalJhonny pingolNo ratings yet
- Physical Exam Final Written Exam Study Guide 2Document51 pagesPhysical Exam Final Written Exam Study Guide 2pelly3190100% (2)
- Vital SignsDocument41 pagesVital SignsfroizkiNo ratings yet
- NCM 101 Health Assessment IiiDocument21 pagesNCM 101 Health Assessment IiiArrianne AbdonNo ratings yet
- Fakultas Kedokteran UnisbaDocument28 pagesFakultas Kedokteran UnisbadeasyahNo ratings yet
- PX FISIK Tubuh ManusiaDocument59 pagesPX FISIK Tubuh ManusiaSheila Jessica AndavaniaNo ratings yet
- Checking A Patient'S Vital SignsDocument29 pagesChecking A Patient'S Vital SignsSaid OmaryNo ratings yet
- Nursing Assessment ToolDocument3 pagesNursing Assessment Toolnjones33No ratings yet
- M.Heldi Riyanda 19334059 B InggrisDocument3 pagesM.Heldi Riyanda 19334059 B InggrisBintan NajihanNo ratings yet
- Kuliah Pemeriksaan Fisik CVDocument49 pagesKuliah Pemeriksaan Fisik CVAyu BintangNo ratings yet
- Assessing Vital SignsDocument42 pagesAssessing Vital SignsGGie Getz100% (2)
- EMT Review - Baseline Vital Signs and SAMPLE HistoryDocument7 pagesEMT Review - Baseline Vital Signs and SAMPLE HistorymrspatmoreNo ratings yet
- Assessing Apical PulseDocument5 pagesAssessing Apical PulseMatthew Ryan100% (1)
- (Nelson Hour) The CV System - HX and PEDocument30 pages(Nelson Hour) The CV System - HX and PEJustin Ng SincoNo ratings yet
- Blood and Pulse Measaurment Topic 1Document17 pagesBlood and Pulse Measaurment Topic 1Amro AzrakNo ratings yet
- Chapter 07 Taking Vital SignsDocument22 pagesChapter 07 Taking Vital SignsNephNo ratings yet
- Baseline Vital Kefah 1BDocument38 pagesBaseline Vital Kefah 1BShahd Abu SnenehNo ratings yet
- Acutely Ill ChildDocument50 pagesAcutely Ill ChildAhmed KhanNo ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- Blood Pressure: Step By Step Guide And Proven Recipes To Lower Your Blood Pressure Without Any MedicationFrom EverandBlood Pressure: Step By Step Guide And Proven Recipes To Lower Your Blood Pressure Without Any MedicationNo ratings yet
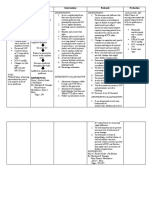
- Date/Time Cues N E E D Nursing Diagnosis Objectives of Care Nursing Interventions EvaluationDocument4 pagesDate/Time Cues N E E D Nursing Diagnosis Objectives of Care Nursing Interventions EvaluationRczhNo ratings yet
- PMH: Iv Access/Fluid/Drip: History: Notes:: SituationDocument1 pagePMH: Iv Access/Fluid/Drip: History: Notes:: SituationAneesNo ratings yet
- Resulting in Damage To Brain Tissue.: Definition: Independent: IndependentDocument4 pagesResulting in Damage To Brain Tissue.: Definition: Independent: Independentalliahjoyce ignacioNo ratings yet
- Checklist For VsDocument2 pagesChecklist For VsAngela Del CastilloNo ratings yet
- Assignment No.1 OB High Risk Grp.1Document15 pagesAssignment No.1 OB High Risk Grp.1YongNo ratings yet
- Activity #5Document11 pagesActivity #5Alpha Jay G. ManijasNo ratings yet
- Patient NCPDocument8 pagesPatient NCPlouie john abilaNo ratings yet
- Evaluation During Postpartum HemorrhageDocument10 pagesEvaluation During Postpartum HemorrhageNilfacio PradoNo ratings yet
- Appendix C Date/Time Soapie/R Nurse'S NotesDocument42 pagesAppendix C Date/Time Soapie/R Nurse'S NotesedwardNo ratings yet
- RLE NCM 107 Workbook Activities and RequirementsDocument7 pagesRLE NCM 107 Workbook Activities and RequirementsJustine CagatanNo ratings yet
- Vital Signs PowerPointDocument29 pagesVital Signs PowerPointMeegs EstabilloNo ratings yet
- Vital SignsDocument90 pagesVital SignsAngelina CoffieNo ratings yet
- NCP For PCAPCDocument6 pagesNCP For PCAPCEnrique Lu100% (1)
- Physical Assessment Health AssessmentDocument6 pagesPhysical Assessment Health AssessmentADOLF FRUELAN HIDALGONo ratings yet
- Casepres NCPDocument6 pagesCasepres NCPdencio1992No ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanVic Intia PaaNo ratings yet
- NCP For PostpartumDocument1 pageNCP For PostpartumMary Hope BacutaNo ratings yet
- Nurses' Notes: Patient Name: AGE: 19 Years Old Hospital No.: Physician: SEX: Female Ward/Room: Nurse SignatureDocument3 pagesNurses' Notes: Patient Name: AGE: 19 Years Old Hospital No.: Physician: SEX: Female Ward/Room: Nurse SignatureNicxx GamingNo ratings yet
- English Task: Indah Febranambela Jovie 1710311061 Faculty of Medicine Andalas UniversityDocument4 pagesEnglish Task: Indah Febranambela Jovie 1710311061 Faculty of Medicine Andalas UniversityEvi YuniwatiNo ratings yet
- Nursing Care PlanDocument44 pagesNursing Care PlanBiway RegalaNo ratings yet
- Dibas PHD SynopsisDocument8 pagesDibas PHD SynopsisDibash HembramNo ratings yet
- Incomplete Spinal Cord Injury Nursing Care Plan (ACTUAL) Patient's Name: Alvarez, Marcelo Age: 59y.o. Sex: M Address: Bacolod CityDocument6 pagesIncomplete Spinal Cord Injury Nursing Care Plan (ACTUAL) Patient's Name: Alvarez, Marcelo Age: 59y.o. Sex: M Address: Bacolod CityTherese MargaretNo ratings yet
- TriageDocument40 pagesTriagerizka50% (2)
- NCP!!!!Document2 pagesNCP!!!!April Grace LopezNo ratings yet
- Quarter 3 Health - 9 Week 3-LAS: Things To Remember in Doing Secondary SurveyDocument4 pagesQuarter 3 Health - 9 Week 3-LAS: Things To Remember in Doing Secondary Surveybelinda dagohoyNo ratings yet
- Assessment: General Survey, Measurement, Vital SignsDocument10 pagesAssessment: General Survey, Measurement, Vital SignsNathan BarrerasNo ratings yet