
Hematuria
Hematuria
You might also like
- NR 508 Test Bank PharmacologyDocument224 pagesNR 508 Test Bank PharmacologyChris100% (2)
- Differential Diagnosis of Flank PainDocument43 pagesDifferential Diagnosis of Flank PainDrArish Mahmood78% (9)
- Urinary Tract Disorders, PowerpointDocument63 pagesUrinary Tract Disorders, Powerpointmutia mutia100% (5)
- Common Symptoms of Kidney Diseases-1Document55 pagesCommon Symptoms of Kidney Diseases-1maruf47774No ratings yet
- Hematuria Final 2Document52 pagesHematuria Final 2aakib saifiNo ratings yet
- Urinary Symptoms - DR RashaDocument70 pagesUrinary Symptoms - DR RashaRasha TelebNo ratings yet
- Child With HematuriaDocument42 pagesChild With HematuriaalaaNo ratings yet
- HematuriaDocument51 pagesHematuriaRam ManoharNo ratings yet
- Renal ProblemsDocument23 pagesRenal ProblemsMuhammad MakkiNo ratings yet
- Approach To Hematuria and Proteinuria in ChildrenDocument52 pagesApproach To Hematuria and Proteinuria in ChildrenMysheb SS100% (1)
- Edema 7 Updated 3Document27 pagesEdema 7 Updated 3vowovan536No ratings yet
- Edema in ChildDocument16 pagesEdema in ChildKesava DassNo ratings yet
- Histopathology of Kidney: Krisna MurtiDocument58 pagesHistopathology of Kidney: Krisna MurtiYUFFANo ratings yet
- Hematuria in ChildrenDocument27 pagesHematuria in ChildrenKousik AmancharlaNo ratings yet
- Genito-Urinary Dysfunctions in Children Commonly Occurring GU DysfunctionsDocument26 pagesGenito-Urinary Dysfunctions in Children Commonly Occurring GU DysfunctionsMaira KhanNo ratings yet
- AscitesDocument63 pagesAscitesfeeo8266No ratings yet
- GI Bleeding:: From Mouth To RectumDocument31 pagesGI Bleeding:: From Mouth To RectumBendy Dwi IrawanNo ratings yet
- Ugib &lgibDocument41 pagesUgib &lgibDawex IsraelNo ratings yet
- Change in Urine Color (2Document38 pagesChange in Urine Color (2Mustafa LaithNo ratings yet
- Acute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CDocument29 pagesAcute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CEdelrose Lapitan100% (1)
- Glomerulonephritis PresentationDocument23 pagesGlomerulonephritis Presentationjacksonyu1234No ratings yet
- Hepatobiliary DiseaseDocument60 pagesHepatobiliary DiseaseFirdaus AslamNo ratings yet
- Pediatric Genitourinary DisordersDocument40 pagesPediatric Genitourinary DisordersGelsey Gelsinator JianNo ratings yet
- Nephritic, Nephrotic Syndrome and Acute Kidney Injury in ChildrenDocument79 pagesNephritic, Nephrotic Syndrome and Acute Kidney Injury in ChildrenB AuNo ratings yet
- Hematuria: Ikobho A. DDocument28 pagesHematuria: Ikobho A. DPrincewill SeiyefaNo ratings yet
- Paediatric Glomerolonephritis and NephroticDocument11 pagesPaediatric Glomerolonephritis and NephroticTiong NeeNo ratings yet
- PembahasanDocument1,129 pagesPembahasanatc100% (1)
- Urinary System and Male Genital: Fajar L. Gultom Departemen Patologi Anatomik FK UKI December 2017Document50 pagesUrinary System and Male Genital: Fajar L. Gultom Departemen Patologi Anatomik FK UKI December 2017Sona SiburianNo ratings yet
- Renal and Urinary DisordersDocument11 pagesRenal and Urinary DisordersChristian Espanilla100% (4)
- Approach To Patient With Renal DiseaseDocument74 pagesApproach To Patient With Renal DiseaseSaja SaqerNo ratings yet
- Patho SlidesDocument46 pagesPatho Slidesapi-400411160No ratings yet
- Urinary Hematologic Metabolic DisorderDocument10 pagesUrinary Hematologic Metabolic DisorderGenki Fay B. LequiganNo ratings yet
- Clinical Features A) Upper Urinary Tract (Pyelonephritis) :: T:Marwa AL-Headri 1Document16 pagesClinical Features A) Upper Urinary Tract (Pyelonephritis) :: T:Marwa AL-Headri 1abnaltag667No ratings yet
- Urine ExaminationDocument32 pagesUrine Examinationhillary temboNo ratings yet
- Nephrotic Syndrome Vs Nephritic SyndromeDocument46 pagesNephrotic Syndrome Vs Nephritic SyndromelilisNo ratings yet
- Hippo EM Board Review - Renal & GU Written SummaryDocument15 pagesHippo EM Board Review - Renal & GU Written Summarykaylawilliam01No ratings yet
- Acute Post-Streptococcal GlomerulonephritisDocument27 pagesAcute Post-Streptococcal GlomerulonephritisAlokh Saha RajNo ratings yet
- UPPER GI BLEEDING in Pediatrics Age GroupDocument28 pagesUPPER GI BLEEDING in Pediatrics Age Groupmanabhanjanmund420No ratings yet
- Acute Kidney Injury: Erika Phillie T. Chua Internal Medicine ResidentDocument48 pagesAcute Kidney Injury: Erika Phillie T. Chua Internal Medicine ResidenterikaNo ratings yet
- Sirosis HepatisDocument54 pagesSirosis HepatisaprillyaNo ratings yet
- Urologic Stone Disease 2005Document51 pagesUrologic Stone Disease 2005jamilNo ratings yet
- Henoch Schonlein Purpura: Dr. Hendratno Halim, Sp. ADocument29 pagesHenoch Schonlein Purpura: Dr. Hendratno Halim, Sp. AYulius Eka Agung Seputra, MSiNo ratings yet
- Approach To A Child With Hematuria:: Sunil Agrawal 1 Year MD Pediatrics, IOMDocument42 pagesApproach To A Child With Hematuria:: Sunil Agrawal 1 Year MD Pediatrics, IOMAnthony Salazar RodríguezNo ratings yet
- Approach To A Patient With Upper GI BleedDocument42 pagesApproach To A Patient With Upper GI BleedMuhammad Naveed AslamNo ratings yet
- Ms Reviewer Renal UrinaryDocument5 pagesMs Reviewer Renal UrinaryAlyssa Nicole CajayonNo ratings yet
- Abnormal Composition of UrineDocument77 pagesAbnormal Composition of Urineangela marie abadillaNo ratings yet
- Haematuria: Definition / Supporting InformationDocument8 pagesHaematuria: Definition / Supporting InformationdrsaleemNo ratings yet
- Acute PancreatitisDocument40 pagesAcute PancreatitisMustafa HusainNo ratings yet
- Atul Sharma Uppergi Fcccm23Document47 pagesAtul Sharma Uppergi Fcccm23Atul SharmaNo ratings yet
- Baldwin Tub Ulo InterstitialDocument36 pagesBaldwin Tub Ulo InterstitialdrryanalwynNo ratings yet
- Nephritis: Presented byDocument32 pagesNephritis: Presented byPavan SorathiyaNo ratings yet
- Acute GI BleedingDocument35 pagesAcute GI BleedingGalih GimastiarNo ratings yet
- Abdominal Distention and AscitesDocument49 pagesAbdominal Distention and AscitesNinaNo ratings yet
- Approach To Hematuria: DR - Rinsha Ravi Dept - of Pediatrics Sath TVMDocument40 pagesApproach To Hematuria: DR - Rinsha Ravi Dept - of Pediatrics Sath TVMAnoop ThoombayilNo ratings yet
- Hepatobiliary System: BY Pranjal Kulkarni Neha ManeDocument85 pagesHepatobiliary System: BY Pranjal Kulkarni Neha ManeGurneetNo ratings yet
- Approach To A Child With HematuriaDocument13 pagesApproach To A Child With HematuriaSaadNo ratings yet
- Liver Cirrhosis: DR Alex MogereDocument51 pagesLiver Cirrhosis: DR Alex MogereGladys Maina100% (1)
- RicoDocument62 pagesRicoCunCunAlAndraNo ratings yet
- F Kuliah-Nephritic Syndrome-FK UiSUDocument40 pagesF Kuliah-Nephritic Syndrome-FK UiSUandreNo ratings yet
- A Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisFrom EverandA Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisRating: 3 out of 5 stars3/5 (1)
- NEPCon-CoC-Annual-Volume Summary-template-Nov17Document12 pagesNEPCon-CoC-Annual-Volume Summary-template-Nov17abraham alonso subiria cuetoNo ratings yet
- Chi-Square and Related DistributionDocument7 pagesChi-Square and Related DistributionMohammedseid AhmedinNo ratings yet
- E. B. Magalona National High School Summative Test in CSS 10 Quarter 1 Week 1 Multiple Choice. Choose The Letter of The Correct AnswerDocument2 pagesE. B. Magalona National High School Summative Test in CSS 10 Quarter 1 Week 1 Multiple Choice. Choose The Letter of The Correct Answerric jason pedralNo ratings yet
- Filipino American RelationshipDocument3 pagesFilipino American RelationshipSamuel Grant ZabalaNo ratings yet
- Engineering Mathematics Questions and Answers - Laplace Transform by Properties - 1Document9 pagesEngineering Mathematics Questions and Answers - Laplace Transform by Properties - 1RAHUL SOLANKENo ratings yet
- Urban Coherence: A Morphological DefinitionDocument19 pagesUrban Coherence: A Morphological DefinitionOlgu CaliskanNo ratings yet
- Gartner MQ On EAM For Delivery UtilitiesDocument25 pagesGartner MQ On EAM For Delivery UtilitiesGnana ShekaranNo ratings yet
- A Poison Tree: The Poet's Background William Blake (28 November 1757 - 12 August 1827) Was An English Poet, Painter, andDocument6 pagesA Poison Tree: The Poet's Background William Blake (28 November 1757 - 12 August 1827) Was An English Poet, Painter, andwan fadhilahNo ratings yet
- SimpleNursing Study GuidesDocument5 pagesSimpleNursing Study Guidessilgabernard100% (1)
- Build Tight RangeDocument8 pagesBuild Tight RangeMihai MunteanuNo ratings yet
- I 0610026377Document15 pagesI 0610026377Arif KurniawanNo ratings yet
- Church GovernmentDocument28 pagesChurch Governmentchris NgonoMNo ratings yet
- Some Oral Chief Mate QuestionsDocument6 pagesSome Oral Chief Mate QuestionsKapil KhandelwalNo ratings yet
- SHS Core - Reading and Writing CG PDFDocument8 pagesSHS Core - Reading and Writing CG PDFRoy Ivan Manuel Reyes67% (6)
- Nisbet Idea of Progress PDFDocument31 pagesNisbet Idea of Progress PDFHernan Cuevas ValenzuelaNo ratings yet
- What Are Free Particles in Quantum MechanicsDocument21 pagesWhat Are Free Particles in Quantum MechanicskalshinokovNo ratings yet
- Brunssen Onevoiceone 2017Document8 pagesBrunssen Onevoiceone 2017stephenieleevos1No ratings yet
- Jordan's LemmaDocument3 pagesJordan's LemmaSergey LiflandskyNo ratings yet
- Chapter 1: Why Study Money, Banking, and Financial Markets?Document23 pagesChapter 1: Why Study Money, Banking, and Financial Markets?Nguyễn Thanh TrangNo ratings yet
- Improved WoodDocument17 pagesImproved WoodPavo33% (3)
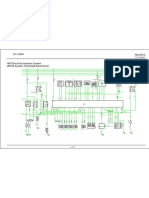
- Circuit Diagram: Ecu A/7Document1 pageCircuit Diagram: Ecu A/7RubénNo ratings yet
- History of Nestorian ChristianityDocument235 pagesHistory of Nestorian ChristianityXu Weiyi100% (3)
- Smart Grid LaboratoriesDocument112 pagesSmart Grid LaboratoriesFahdAhmed0% (1)
- Confessions of Some High Ranking 1Document111 pagesConfessions of Some High Ranking 1Habilian AssociationNo ratings yet
- Diagnosis of Hirschsprung Disease: Lusine Ambartsumyan, Caitlin Smith, and Raj P KapurDocument15 pagesDiagnosis of Hirschsprung Disease: Lusine Ambartsumyan, Caitlin Smith, and Raj P KapurGhina Mauizha WulandariNo ratings yet
- 6 Key Challenges For Financial Close and ReportingDocument7 pages6 Key Challenges For Financial Close and ReportingGodfrey KakalaNo ratings yet
- Lab 3Document23 pagesLab 3RAMESH KUMARNo ratings yet
- Iterative Business Model Innovation A Conceptual Proc - 2023 - Journal of BusinDocument14 pagesIterative Business Model Innovation A Conceptual Proc - 2023 - Journal of Busintranhungduc1995No ratings yet






















































































Download as pptx, pdf, or txt
You might also like
- NR 508 Test Bank PharmacologyDocument224 pagesNR 508 Test Bank PharmacologyChris100% (2)
- Differential Diagnosis of Flank PainDocument43 pagesDifferential Diagnosis of Flank PainDrArish Mahmood78% (9)
- Urinary Tract Disorders, PowerpointDocument63 pagesUrinary Tract Disorders, Powerpointmutia mutia100% (5)
- Common Symptoms of Kidney Diseases-1Document55 pagesCommon Symptoms of Kidney Diseases-1maruf47774No ratings yet
- Hematuria Final 2Document52 pagesHematuria Final 2aakib saifiNo ratings yet
- Urinary Symptoms - DR RashaDocument70 pagesUrinary Symptoms - DR RashaRasha TelebNo ratings yet
- Child With HematuriaDocument42 pagesChild With HematuriaalaaNo ratings yet
- HematuriaDocument51 pagesHematuriaRam ManoharNo ratings yet
- Renal ProblemsDocument23 pagesRenal ProblemsMuhammad MakkiNo ratings yet
- Approach To Hematuria and Proteinuria in ChildrenDocument52 pagesApproach To Hematuria and Proteinuria in ChildrenMysheb SS100% (1)
- Edema 7 Updated 3Document27 pagesEdema 7 Updated 3vowovan536No ratings yet
- Edema in ChildDocument16 pagesEdema in ChildKesava DassNo ratings yet
- Histopathology of Kidney: Krisna MurtiDocument58 pagesHistopathology of Kidney: Krisna MurtiYUFFANo ratings yet
- Hematuria in ChildrenDocument27 pagesHematuria in ChildrenKousik AmancharlaNo ratings yet
- Genito-Urinary Dysfunctions in Children Commonly Occurring GU DysfunctionsDocument26 pagesGenito-Urinary Dysfunctions in Children Commonly Occurring GU DysfunctionsMaira KhanNo ratings yet
- AscitesDocument63 pagesAscitesfeeo8266No ratings yet
- GI Bleeding:: From Mouth To RectumDocument31 pagesGI Bleeding:: From Mouth To RectumBendy Dwi IrawanNo ratings yet
- Ugib &lgibDocument41 pagesUgib &lgibDawex IsraelNo ratings yet
- Change in Urine Color (2Document38 pagesChange in Urine Color (2Mustafa LaithNo ratings yet
- Acute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CDocument29 pagesAcute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CEdelrose Lapitan100% (1)
- Glomerulonephritis PresentationDocument23 pagesGlomerulonephritis Presentationjacksonyu1234No ratings yet
- Hepatobiliary DiseaseDocument60 pagesHepatobiliary DiseaseFirdaus AslamNo ratings yet
- Pediatric Genitourinary DisordersDocument40 pagesPediatric Genitourinary DisordersGelsey Gelsinator JianNo ratings yet
- Nephritic, Nephrotic Syndrome and Acute Kidney Injury in ChildrenDocument79 pagesNephritic, Nephrotic Syndrome and Acute Kidney Injury in ChildrenB AuNo ratings yet
- Hematuria: Ikobho A. DDocument28 pagesHematuria: Ikobho A. DPrincewill SeiyefaNo ratings yet
- Paediatric Glomerolonephritis and NephroticDocument11 pagesPaediatric Glomerolonephritis and NephroticTiong NeeNo ratings yet
- PembahasanDocument1,129 pagesPembahasanatc100% (1)
- Urinary System and Male Genital: Fajar L. Gultom Departemen Patologi Anatomik FK UKI December 2017Document50 pagesUrinary System and Male Genital: Fajar L. Gultom Departemen Patologi Anatomik FK UKI December 2017Sona SiburianNo ratings yet
- Renal and Urinary DisordersDocument11 pagesRenal and Urinary DisordersChristian Espanilla100% (4)
- Approach To Patient With Renal DiseaseDocument74 pagesApproach To Patient With Renal DiseaseSaja SaqerNo ratings yet
- Patho SlidesDocument46 pagesPatho Slidesapi-400411160No ratings yet
- Urinary Hematologic Metabolic DisorderDocument10 pagesUrinary Hematologic Metabolic DisorderGenki Fay B. LequiganNo ratings yet
- Clinical Features A) Upper Urinary Tract (Pyelonephritis) :: T:Marwa AL-Headri 1Document16 pagesClinical Features A) Upper Urinary Tract (Pyelonephritis) :: T:Marwa AL-Headri 1abnaltag667No ratings yet
- Urine ExaminationDocument32 pagesUrine Examinationhillary temboNo ratings yet
- Nephrotic Syndrome Vs Nephritic SyndromeDocument46 pagesNephrotic Syndrome Vs Nephritic SyndromelilisNo ratings yet
- Hippo EM Board Review - Renal & GU Written SummaryDocument15 pagesHippo EM Board Review - Renal & GU Written Summarykaylawilliam01No ratings yet
- Acute Post-Streptococcal GlomerulonephritisDocument27 pagesAcute Post-Streptococcal GlomerulonephritisAlokh Saha RajNo ratings yet
- UPPER GI BLEEDING in Pediatrics Age GroupDocument28 pagesUPPER GI BLEEDING in Pediatrics Age Groupmanabhanjanmund420No ratings yet
- Acute Kidney Injury: Erika Phillie T. Chua Internal Medicine ResidentDocument48 pagesAcute Kidney Injury: Erika Phillie T. Chua Internal Medicine ResidenterikaNo ratings yet
- Sirosis HepatisDocument54 pagesSirosis HepatisaprillyaNo ratings yet
- Urologic Stone Disease 2005Document51 pagesUrologic Stone Disease 2005jamilNo ratings yet
- Henoch Schonlein Purpura: Dr. Hendratno Halim, Sp. ADocument29 pagesHenoch Schonlein Purpura: Dr. Hendratno Halim, Sp. AYulius Eka Agung Seputra, MSiNo ratings yet
- Approach To A Child With Hematuria:: Sunil Agrawal 1 Year MD Pediatrics, IOMDocument42 pagesApproach To A Child With Hematuria:: Sunil Agrawal 1 Year MD Pediatrics, IOMAnthony Salazar RodríguezNo ratings yet
- Approach To A Patient With Upper GI BleedDocument42 pagesApproach To A Patient With Upper GI BleedMuhammad Naveed AslamNo ratings yet
- Ms Reviewer Renal UrinaryDocument5 pagesMs Reviewer Renal UrinaryAlyssa Nicole CajayonNo ratings yet
- Abnormal Composition of UrineDocument77 pagesAbnormal Composition of Urineangela marie abadillaNo ratings yet
- Haematuria: Definition / Supporting InformationDocument8 pagesHaematuria: Definition / Supporting InformationdrsaleemNo ratings yet
- Acute PancreatitisDocument40 pagesAcute PancreatitisMustafa HusainNo ratings yet
- Atul Sharma Uppergi Fcccm23Document47 pagesAtul Sharma Uppergi Fcccm23Atul SharmaNo ratings yet
- Baldwin Tub Ulo InterstitialDocument36 pagesBaldwin Tub Ulo InterstitialdrryanalwynNo ratings yet
- Nephritis: Presented byDocument32 pagesNephritis: Presented byPavan SorathiyaNo ratings yet
- Acute GI BleedingDocument35 pagesAcute GI BleedingGalih GimastiarNo ratings yet
- Abdominal Distention and AscitesDocument49 pagesAbdominal Distention and AscitesNinaNo ratings yet
- Approach To Hematuria: DR - Rinsha Ravi Dept - of Pediatrics Sath TVMDocument40 pagesApproach To Hematuria: DR - Rinsha Ravi Dept - of Pediatrics Sath TVMAnoop ThoombayilNo ratings yet
- Hepatobiliary System: BY Pranjal Kulkarni Neha ManeDocument85 pagesHepatobiliary System: BY Pranjal Kulkarni Neha ManeGurneetNo ratings yet
- Approach To A Child With HematuriaDocument13 pagesApproach To A Child With HematuriaSaadNo ratings yet
- Liver Cirrhosis: DR Alex MogereDocument51 pagesLiver Cirrhosis: DR Alex MogereGladys Maina100% (1)
- RicoDocument62 pagesRicoCunCunAlAndraNo ratings yet
- F Kuliah-Nephritic Syndrome-FK UiSUDocument40 pagesF Kuliah-Nephritic Syndrome-FK UiSUandreNo ratings yet
- A Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisFrom EverandA Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisRating: 3 out of 5 stars3/5 (1)
- NEPCon-CoC-Annual-Volume Summary-template-Nov17Document12 pagesNEPCon-CoC-Annual-Volume Summary-template-Nov17abraham alonso subiria cuetoNo ratings yet
- Chi-Square and Related DistributionDocument7 pagesChi-Square and Related DistributionMohammedseid AhmedinNo ratings yet
- E. B. Magalona National High School Summative Test in CSS 10 Quarter 1 Week 1 Multiple Choice. Choose The Letter of The Correct AnswerDocument2 pagesE. B. Magalona National High School Summative Test in CSS 10 Quarter 1 Week 1 Multiple Choice. Choose The Letter of The Correct Answerric jason pedralNo ratings yet
- Filipino American RelationshipDocument3 pagesFilipino American RelationshipSamuel Grant ZabalaNo ratings yet
- Engineering Mathematics Questions and Answers - Laplace Transform by Properties - 1Document9 pagesEngineering Mathematics Questions and Answers - Laplace Transform by Properties - 1RAHUL SOLANKENo ratings yet
- Urban Coherence: A Morphological DefinitionDocument19 pagesUrban Coherence: A Morphological DefinitionOlgu CaliskanNo ratings yet
- Gartner MQ On EAM For Delivery UtilitiesDocument25 pagesGartner MQ On EAM For Delivery UtilitiesGnana ShekaranNo ratings yet
- A Poison Tree: The Poet's Background William Blake (28 November 1757 - 12 August 1827) Was An English Poet, Painter, andDocument6 pagesA Poison Tree: The Poet's Background William Blake (28 November 1757 - 12 August 1827) Was An English Poet, Painter, andwan fadhilahNo ratings yet
- SimpleNursing Study GuidesDocument5 pagesSimpleNursing Study Guidessilgabernard100% (1)
- Build Tight RangeDocument8 pagesBuild Tight RangeMihai MunteanuNo ratings yet
- I 0610026377Document15 pagesI 0610026377Arif KurniawanNo ratings yet
- Church GovernmentDocument28 pagesChurch Governmentchris NgonoMNo ratings yet
- Some Oral Chief Mate QuestionsDocument6 pagesSome Oral Chief Mate QuestionsKapil KhandelwalNo ratings yet
- SHS Core - Reading and Writing CG PDFDocument8 pagesSHS Core - Reading and Writing CG PDFRoy Ivan Manuel Reyes67% (6)
- Nisbet Idea of Progress PDFDocument31 pagesNisbet Idea of Progress PDFHernan Cuevas ValenzuelaNo ratings yet
- What Are Free Particles in Quantum MechanicsDocument21 pagesWhat Are Free Particles in Quantum MechanicskalshinokovNo ratings yet
- Brunssen Onevoiceone 2017Document8 pagesBrunssen Onevoiceone 2017stephenieleevos1No ratings yet
- Jordan's LemmaDocument3 pagesJordan's LemmaSergey LiflandskyNo ratings yet
- Chapter 1: Why Study Money, Banking, and Financial Markets?Document23 pagesChapter 1: Why Study Money, Banking, and Financial Markets?Nguyễn Thanh TrangNo ratings yet
- Improved WoodDocument17 pagesImproved WoodPavo33% (3)
- Circuit Diagram: Ecu A/7Document1 pageCircuit Diagram: Ecu A/7RubénNo ratings yet
- History of Nestorian ChristianityDocument235 pagesHistory of Nestorian ChristianityXu Weiyi100% (3)
- Smart Grid LaboratoriesDocument112 pagesSmart Grid LaboratoriesFahdAhmed0% (1)
- Confessions of Some High Ranking 1Document111 pagesConfessions of Some High Ranking 1Habilian AssociationNo ratings yet
- Diagnosis of Hirschsprung Disease: Lusine Ambartsumyan, Caitlin Smith, and Raj P KapurDocument15 pagesDiagnosis of Hirschsprung Disease: Lusine Ambartsumyan, Caitlin Smith, and Raj P KapurGhina Mauizha WulandariNo ratings yet
- 6 Key Challenges For Financial Close and ReportingDocument7 pages6 Key Challenges For Financial Close and ReportingGodfrey KakalaNo ratings yet
- Lab 3Document23 pagesLab 3RAMESH KUMARNo ratings yet
- Iterative Business Model Innovation A Conceptual Proc - 2023 - Journal of BusinDocument14 pagesIterative Business Model Innovation A Conceptual Proc - 2023 - Journal of Busintranhungduc1995No ratings yet