Download as pptx, pdf, or txt
You might also like
- Strabismus SimplifiedDocument530 pagesStrabismus SimplifiedIsaac Aleman100% (1)
- Assistive DevicesDocument30 pagesAssistive DevicesrlinaoNo ratings yet
- 13 Principles of Sterile TechniqueDocument3 pages13 Principles of Sterile TechniqueOlive Keithy Ascaño ReyesNo ratings yet
- Lect. 3 (Test 2) - 2023Document22 pagesLect. 3 (Test 2) - 2023nagyrashad123No ratings yet
- Posture 2022Document22 pagesPosture 2022Loreli HornbyNo ratings yet
- Kinetics & Kinematics Od ADLDocument26 pagesKinetics & Kinematics Od ADLPriyanka kedare100% (1)
- 5-Flexibility TestsDocument62 pages5-Flexibility TestsMr. MixerNo ratings yet
- Does Increasing Core Strength Aid in Speed of Recovery?: Team 2 - Robyn, Vikki and SusanDocument27 pagesDoes Increasing Core Strength Aid in Speed of Recovery?: Team 2 - Robyn, Vikki and SusanPratik DiyoraNo ratings yet
- Kine 2nd YearDocument21 pagesKine 2nd YearzeeshanNo ratings yet
- Core StrengtheningDocument27 pagesCore StrengtheningNidhin Jose100% (3)
- Trunk Stability by Calvin Morriss, PHD.: What Exactly Is Trunk Stability For A Rugby Player?Document9 pagesTrunk Stability by Calvin Morriss, PHD.: What Exactly Is Trunk Stability For A Rugby Player?Justice Man100% (1)
- C Biomechanics and AdvantageDocument18 pagesC Biomechanics and Advantageno thanksNo ratings yet
- Body Mechanics: Efficient, Coordinated, and SafeDocument31 pagesBody Mechanics: Efficient, Coordinated, and SafeRhea Lyn LamosteNo ratings yet
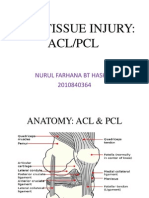
- Acl PCL PresentationDocument17 pagesAcl PCL PresentationSafwan Idham RamlanNo ratings yet
- Bullworker Bow Classic ONLINE 1 PDFDocument64 pagesBullworker Bow Classic ONLINE 1 PDFRahul Runwal100% (5)
- Core Training 1 1Document24 pagesCore Training 1 1painaganmilescent09No ratings yet
- Assessment of The Musculo-Skeletal SystemDocument46 pagesAssessment of The Musculo-Skeletal SystemRaquel M. MendozaNo ratings yet
- Functional Reeducation Techniques: Presenter by Arambam Meiteileima Chanu 1 Year, MPT (Neuro)Document38 pagesFunctional Reeducation Techniques: Presenter by Arambam Meiteileima Chanu 1 Year, MPT (Neuro)deepuphysio94% (18)
- Ace Personal Trainer Chapter 3Document45 pagesAce Personal Trainer Chapter 3Daan van der Meulen100% (2)
- Core EssentialsDocument33 pagesCore EssentialsGul RockzzNo ratings yet
- Penuntun Praktikum Musculoskeletal System: Suyasning HIDocument32 pagesPenuntun Praktikum Musculoskeletal System: Suyasning HIkomang nickoNo ratings yet
- Muscle TermsDocument26 pagesMuscle Termscandace728No ratings yet
- Body MechanicsDocument34 pagesBody MechanicsAngel CauilanNo ratings yet
- Frozen Shoulder: By: Kanchan SharmaDocument21 pagesFrozen Shoulder: By: Kanchan SharmaKanchan SharmaNo ratings yet
- Meniscus Injury: Khairul Nizam Abdul Rahman 4262143008Document22 pagesMeniscus Injury: Khairul Nizam Abdul Rahman 4262143008Soumashree MondalNo ratings yet
- Body MechanicsDocument42 pagesBody MechanicsLouzaldy Earl ThorntonNo ratings yet
- Exercise: Cristina M. Medina, RN, MAN Jayme P. Hipolito, RN, MAN Lorna Mendoza, RN, MANDocument26 pagesExercise: Cristina M. Medina, RN, MAN Jayme P. Hipolito, RN, MAN Lorna Mendoza, RN, MANAlma Janella TOSINONo ratings yet
- 9 HRF SRFDocument33 pages9 HRF SRFrichard aballeNo ratings yet
- Pelvic Conditions 1 3Document39 pagesPelvic Conditions 1 3Princess DomingoNo ratings yet
- Sport Traumatology-III Knee Complex-10Document26 pagesSport Traumatology-III Knee Complex-10kamran aliNo ratings yet
- Scapular DyskinesisDocument32 pagesScapular DyskinesisorthodoctorvinayNo ratings yet
- Pelvic, Hip-Knee Joints & RehabDocument110 pagesPelvic, Hip-Knee Joints & Rehabkhorrami4100% (2)
- Examination of The ShoulderDocument20 pagesExamination of The ShoulderMalvino Giovanni100% (1)
- Hip Joint ExaminationDocument53 pagesHip Joint ExaminationmybabyistaeNo ratings yet
- Act.2 MenuofexercisesDocument12 pagesAct.2 MenuofexercisesLouisa TaypinNo ratings yet
- Walking Aids: By: Reeta Sawlani Lecturer Iprs PumhswDocument52 pagesWalking Aids: By: Reeta Sawlani Lecturer Iprs PumhswNoman SamiNo ratings yet
- Spine Exam 2Document44 pagesSpine Exam 2Azmi FarhadiNo ratings yet
- Fitness Assessment 1Document17 pagesFitness Assessment 1Yeona BaeNo ratings yet
- Basic Body MechanicsDocument83 pagesBasic Body MechanicsCyrille Aira AndresaNo ratings yet
- Lesson 6 - Warm-Up & Cool Down ExercisesDocument60 pagesLesson 6 - Warm-Up & Cool Down ExercisesRishiel Dimple BalonesNo ratings yet
- Shoulder Syndromes: P. Gunnar Brolinson, DO, FAOASM, FACOFP, FAAFPDocument79 pagesShoulder Syndromes: P. Gunnar Brolinson, DO, FAOASM, FACOFP, FAAFPYS NateNo ratings yet
- HPHE 4450: Section 07 - Muscular Strength, Endurance, FlexibilityDocument63 pagesHPHE 4450: Section 07 - Muscular Strength, Endurance, FlexibilityChristopher CheathamNo ratings yet
- Physical Ex of ElbowDocument23 pagesPhysical Ex of ElbowNgurah AndhikaNo ratings yet
- GALS AssessmentDocument46 pagesGALS AssessmentdrindrasNo ratings yet
- Scapular Stabilization ExercisesDocument2 pagesScapular Stabilization ExercisesnimitrisNo ratings yet
- Crawling Exercise: Dr. Hiral Katakia MPT (Neuro)Document20 pagesCrawling Exercise: Dr. Hiral Katakia MPT (Neuro)Rohan LAl100% (3)
- Assessment of The Musclo-Skletal SystemDocument25 pagesAssessment of The Musclo-Skletal SystemjacnpoyNo ratings yet
- ACL Reconstruction 2020Document39 pagesACL Reconstruction 2020محمد عقلNo ratings yet
- Core TrainingDocument18 pagesCore Trainingrqpz9rppx4No ratings yet
- Fundamental Movement PatternsDocument14 pagesFundamental Movement PatternsAnna Imaysay100% (1)
- Balance - 11118 - PT 1111-T - 30-12-2021Document23 pagesBalance - 11118 - PT 1111-T - 30-12-2021fernandesmarceia1975No ratings yet
- Biofeedback Stabilizer Manual PDFDocument188 pagesBiofeedback Stabilizer Manual PDFEugenio López Recio100% (1)
- Keeping Your Shoulders HealthyDocument38 pagesKeeping Your Shoulders Healthyxyz84No ratings yet
- Lumbar SpondylosisDocument49 pagesLumbar Spondylosisfreska ayu wardhaniNo ratings yet
- 6 Elbow and WristDocument76 pages6 Elbow and Wristalinaziyad3No ratings yet
- Lesson 1 Aerobic and Anaerobic ExercisesDocument39 pagesLesson 1 Aerobic and Anaerobic ExercisesAnthea ImalayNo ratings yet
- WK 6 Study QsDocument7 pagesWK 6 Study Qsapi-479720222No ratings yet
- Lecture 4 - Basic Anatomy and BiomechanicsDocument14 pagesLecture 4 - Basic Anatomy and BiomechanicsRon Budnar100% (2)
- Tight Hip Flexors: Comprehensive Guide on How to Efficiently Relieve All Kinds of Pain Associated with Tight Hip Flexors in less Than 5 minutes; Tight Hip Flexor Home/Gym Remedies (Beginner's Guide)From EverandTight Hip Flexors: Comprehensive Guide on How to Efficiently Relieve All Kinds of Pain Associated with Tight Hip Flexors in less Than 5 minutes; Tight Hip Flexor Home/Gym Remedies (Beginner's Guide)No ratings yet
- Simplified Strength Training using your Bodyweight and a Towel at Home Vol. 1: Legs/Quads: VolFrom EverandSimplified Strength Training using your Bodyweight and a Towel at Home Vol. 1: Legs/Quads: VolNo ratings yet
- Summary of Dr. Aaron Horschig, Dr. Kevin Sonthana & Travis Neff's The Squat BibleFrom EverandSummary of Dr. Aaron Horschig, Dr. Kevin Sonthana & Travis Neff's The Squat BibleNo ratings yet
- Trial Ospe 1 Year: From PPSP UsmkkDocument43 pagesTrial Ospe 1 Year: From PPSP UsmkkEddy Loo100% (1)
- The Boundaries of The Anterior Abdominal Wall AreDocument62 pagesThe Boundaries of The Anterior Abdominal Wall ArebeeNo ratings yet
- Abdomen - 1Document48 pagesAbdomen - 1rohanshah1No ratings yet
- Your Ultimate 4-Week Core Strength Plan: Cloud - DownloadDocument30 pagesYour Ultimate 4-Week Core Strength Plan: Cloud - DownloadLuis QuintanillaNo ratings yet
- Black S Medical Dictionary PDFDocument2,413 pagesBlack S Medical Dictionary PDFAlexandr Trotsky100% (1)
- Cystostomy NewDocument32 pagesCystostomy Newkuncupcupu1368No ratings yet
- TBL Abdomen & Ingunal Canal QxsDocument5 pagesTBL Abdomen & Ingunal Canal QxsKAYISIRE EMERYNo ratings yet
- Leg RaisesDocument81 pagesLeg RaisesFlakko137100% (9)
- Mymianmian Swiss Ball ExerciseDocument129 pagesMymianmian Swiss Ball ExerciseFlavius Murariu100% (14)
- Obstetrics Study Guide 2: in The Name of GodDocument122 pagesObstetrics Study Guide 2: in The Name of GodGa B B OrlonganNo ratings yet
- Inguinal Region AnatomyDocument6 pagesInguinal Region AnatomysimonaNo ratings yet
- Abdomen For PHDocument219 pagesAbdomen For PHD TekNo ratings yet
- Abdominal HerniaDocument2 pagesAbdominal HerniaAshan BopitiyaNo ratings yet
- Covered Exstrophy. A Rare Variant of Classical BladderDocument4 pagesCovered Exstrophy. A Rare Variant of Classical BladderGunduz AgaNo ratings yet
- Development and Reliability of The Modified Tool For Assessment of Diastasis RectiDocument3 pagesDevelopment and Reliability of The Modified Tool For Assessment of Diastasis RectiInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Abdominal Supporting Belt 1 PDFDocument5 pagesAbdominal Supporting Belt 1 PDFcepiNo ratings yet
- Simply Shredded AbsDocument23 pagesSimply Shredded AbsARJUN BEDI204005100% (2)
- Netter's Anatomy Coloring BookfeffsdfhujDocument2 pagesNetter's Anatomy Coloring BookfeffsdfhujAndreea GheorgheNo ratings yet
- Hernia Supp 2011Document76 pagesHernia Supp 2011bogdanotiNo ratings yet
- Restore Your CoreDocument44 pagesRestore Your CoreKristi Kashta100% (1)
- Human AnatomyDocument2 pagesHuman AnatomyBabylove GoalsNo ratings yet
- PARmedX For PregnancyDocument4 pagesPARmedX For PregnancySP Samuel CrespoNo ratings yet
- CoreWalking Eworkbook PDFDocument79 pagesCoreWalking Eworkbook PDFmike100% (1)
- Anatomy of Abdomen PDFDocument10 pagesAnatomy of Abdomen PDFSiva ShanmugamNo ratings yet
- Abdominal Wall, Omentum, Mesentery and RetroperitoneumDocument8 pagesAbdominal Wall, Omentum, Mesentery and RetroperitoneumRae Marie AquinoNo ratings yet
- Chapter 4 - Spine and ThoraxDocument24 pagesChapter 4 - Spine and ThoraxmassagekevinNo ratings yet
- Abdomen ExaminationDocument37 pagesAbdomen ExaminationJaaydevNo ratings yet
- The Best Abs WorkoutDocument5 pagesThe Best Abs WorkoutGuillaume VingtcentNo ratings yet