
5_6109514227494420945 (1)
5_6109514227494420945 (1)
You might also like
- Malawi 2014 Malawi Obstetric and Gynaecology Protocols GuidelinesDocument105 pagesMalawi 2014 Malawi Obstetric and Gynaecology Protocols GuidelinesHải Ly Đào67% (3)
- Pituitary Tumors: A Clinical CasebookFrom EverandPituitary Tumors: A Clinical CasebookLisa B. NachtigallNo ratings yet
- Gestational Trophoblastic Tumours UG LECT.Document70 pagesGestational Trophoblastic Tumours UG LECT.TiwiNo ratings yet
- Gestational Trophoblastic Disease - OBS & GYN NOTESDocument52 pagesGestational Trophoblastic Disease - OBS & GYN NOTESNagulan ChanemougameNo ratings yet
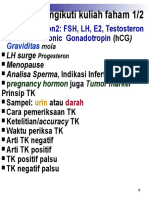
- Setelah Mengikuti Kuliah Faham 1/2: Faham Hormon2: FSH, LH, E2, Testosteron Human Chorionic GonadotropinDocument32 pagesSetelah Mengikuti Kuliah Faham 1/2: Faham Hormon2: FSH, LH, E2, Testosteron Human Chorionic Gonadotropinruth thauladanNo ratings yet
- Testing During Pregnancy: David G. Grenache, PHD University of Utah & Arup Laboratories Salt Lake City, UtDocument54 pagesTesting During Pregnancy: David G. Grenache, PHD University of Utah & Arup Laboratories Salt Lake City, Utمحمد عمران راناNo ratings yet
- Gestational Trophoblastic DiseaseDocument37 pagesGestational Trophoblastic DiseaseOlisa 'phage' Onyebuchi100% (1)
- Graviditas: Faham Hormon2: FSH, LH, E2, Testosteron Human Chorionic GonadotropinDocument32 pagesGraviditas: Faham Hormon2: FSH, LH, E2, Testosteron Human Chorionic Gonadotropinruth thauladanNo ratings yet
- 。18. Molar PregnancyDocument29 pages。18. Molar Pregnancygenaong2003No ratings yet
- Molar Pregnancy & ChoriocarcinomaDocument16 pagesMolar Pregnancy & ChoriocarcinomaIbrahim JameelallaNo ratings yet
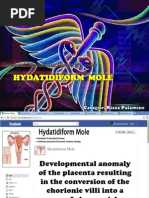
- Hydatidiform MoleDocument38 pagesHydatidiform Molesushma silwalNo ratings yet
- Gestational Trophoblastic Diseases (GTD)Document39 pagesGestational Trophoblastic Diseases (GTD)moreen kipkemoiNo ratings yet
- Ectopi C PregnancyDocument28 pagesEctopi C PregnancySazzad HossainNo ratings yet
- Diagnosis of PregnancyDocument23 pagesDiagnosis of PregnancyNeelesh BhandariNo ratings yet
- Gestational Trophoblastic Disease: Prepared By: Nikita PatelDocument20 pagesGestational Trophoblastic Disease: Prepared By: Nikita PatelVaishaliNo ratings yet
- Elevated Beta Human Chorionic Gonadotropin in A Non-Pregnant Female Diagnosed With Anal Squamous Cell CarcinomaDocument4 pagesElevated Beta Human Chorionic Gonadotropin in A Non-Pregnant Female Diagnosed With Anal Squamous Cell CarcinomaKatherine Elizabeth Urbina QuispeNo ratings yet
- 2b Case StudyDocument5 pages2b Case StudyCkaye MontilNo ratings yet
- Pregnancy Handbook: "Am I Pregnant?" All B-HCG Levels ExplainedDocument74 pagesPregnancy Handbook: "Am I Pregnant?" All B-HCG Levels ExplainedDr0Web100% (1)
- Pregnancytests 180321025548Document51 pagesPregnancytests 180321025548Dorin PathakNo ratings yet
- Kuliah PK2 TESKehamilanJULI2010Document38 pagesKuliah PK2 TESKehamilanJULI2010Fetty NataliaNo ratings yet
- Abnormal Uterine BleedingDocument46 pagesAbnormal Uterine BleedingNur Aliah Amirah AmranNo ratings yet
- H MoleDocument71 pagesH MoleDoc AchondoNo ratings yet
- With DR WajeihDocument62 pagesWith DR WajeihZeeshan AhmedNo ratings yet
- Fertility: Assessment and Treatment For People With Fertility ProblemsDocument4 pagesFertility: Assessment and Treatment For People With Fertility ProblemsPatrick CoghlanNo ratings yet
- (Hich2) Recurrent Pregnancy LossDocument33 pages(Hich2) Recurrent Pregnancy LossAli B. SafadiNo ratings yet
- Beta HCGDocument23 pagesBeta HCGpawchanNo ratings yet
- Transient Thyrotoxicosis in Molar PregnancyDocument2 pagesTransient Thyrotoxicosis in Molar PregnancyWilliam OttoNo ratings yet
- Menstrual Disorders and PCOS Webinar EMBRYO FKUI 2022Document49 pagesMenstrual Disorders and PCOS Webinar EMBRYO FKUI 2022angelinputri100% (1)
- CCD Obstetric GynecologyDocument43 pagesCCD Obstetric GynecologyHanif GandohNo ratings yet
- Sero FullDocument30 pagesSero Fullmihret geneneNo ratings yet
- Thyroid and ReproductionDocument42 pagesThyroid and Reproductionabraham winartoNo ratings yet
- Gestational Trophoblastic DiseasesDocument37 pagesGestational Trophoblastic DiseasesEdwin OkonNo ratings yet
- Follicle Stimulating HormoneDocument13 pagesFollicle Stimulating HormoneAgustinus SuryaNo ratings yet
- NurseryDocument30 pagesNurserymirandaNo ratings yet
- Determination of Hormones: Mohamed A.Ali BSC - HLS, Admls, DmlsDocument43 pagesDetermination of Hormones: Mohamed A.Ali BSC - HLS, Admls, Dmlsmoha3liNo ratings yet
- Pregnancy Test and Semen Analysis PDFDocument8 pagesPregnancy Test and Semen Analysis PDFबुद्ध मोक्तानNo ratings yet
- 5 PcosDocument67 pages5 PcosyewollolijfikreNo ratings yet
- Polycystic OvaryDocument25 pagesPolycystic OvaryAli AbdElnaby SalimNo ratings yet
- Hydatidiform MoleDocument5 pagesHydatidiform MoleReynaldo SutantoNo ratings yet
- Assisted Reproductive TechniquesDocument146 pagesAssisted Reproductive TechniquesGouravNo ratings yet
- Tumor Markers Some Laboratory Aspects of Pregnancy Cerebrospinal Fluid AnalysisDocument40 pagesTumor Markers Some Laboratory Aspects of Pregnancy Cerebrospinal Fluid AnalysisMans FansNo ratings yet
- Seminar Gestational Trophoblastic DiseaseDocument27 pagesSeminar Gestational Trophoblastic Diseasehusnajihah18No ratings yet
- Activity No. 10 Qualitative HCG DeterminationDocument9 pagesActivity No. 10 Qualitative HCG DeterminationCruz JenniferNo ratings yet
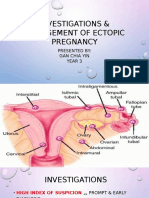
- 3 Investigation & Management of Ectopic PregnancyDocument38 pages3 Investigation & Management of Ectopic PregnancyMegavarnen GobinathanNo ratings yet
- AbortionDocument32 pagesAbortionD & S SeriesNo ratings yet
- Pregnancy DXDocument20 pagesPregnancy DXyewollolijfikreNo ratings yet
- Thrombophilia: Duha Alharbi, MD InternDocument30 pagesThrombophilia: Duha Alharbi, MD InternabrarNo ratings yet
- Acute Parenchymal Liver DiseaseDocument29 pagesAcute Parenchymal Liver Diseasejeevan ghimireNo ratings yet
- Hormones of The PlacentaDocument75 pagesHormones of The PlacentaAbdikadir AhmedNo ratings yet
- HCG Strip (OneStep)Document2 pagesHCG Strip (OneStep)Rita WidaningsihNo ratings yet
- PIDC Grand Round FinalDocument32 pagesPIDC Grand Round Finalhailu henockNo ratings yet
- Hormones of The PlacentaDocument67 pagesHormones of The PlacentagibreilNo ratings yet
- DiscussionDocument28 pagesDiscussionJee AmanteNo ratings yet
- Quantitative and QualitativeDocument4 pagesQuantitative and QualitativekukadiyaNo ratings yet
- Ahmed Mohamed Abdel Rahim Rammah: Senior Registrar Obstetrics and Gynecology Department Al - Adan Hospital, KuwaitDocument32 pagesAhmed Mohamed Abdel Rahim Rammah: Senior Registrar Obstetrics and Gynecology Department Al - Adan Hospital, Kuwaithossam626No ratings yet
- BVGH-University of Rwanda Virtual Gynecologic Oncology CourseDocument43 pagesBVGH-University of Rwanda Virtual Gynecologic Oncology CourseEmmanuel NdikuryayoNo ratings yet
- Precociou S Puberty: BY Vishnupriya Ravimohandoss Year-6 Group-1Document31 pagesPrecociou S Puberty: BY Vishnupriya Ravimohandoss Year-6 Group-1Priya RaviNo ratings yet
- Comportamiento de La Gonadotropina en El Embarazo 240308 192849Document10 pagesComportamiento de La Gonadotropina en El Embarazo 240308 192849VictorRojasNo ratings yet
- Biochemical Investigation of Infertile Couple-My PresentationDocument91 pagesBiochemical Investigation of Infertile Couple-My PresentationOlukoyejo OluwaboriNo ratings yet
- Precocious PubertyDocument4 pagesPrecocious PubertyHa Jae kyeongNo ratings yet
- 2nd Trimester BleedingDocument50 pages2nd Trimester BleedingRaiden VizcondeNo ratings yet
- Jurnal Mola HidatidosaDocument8 pagesJurnal Mola HidatidosaDebby SofianaNo ratings yet
- Abnormal Obstetrics EditedDocument11 pagesAbnormal Obstetrics EditedAbhie Gayle Erbon AbonallaNo ratings yet
- (GYNE) 3.05 Gestational Trophoblastic Disease - Co-HidalgoDocument7 pages(GYNE) 3.05 Gestational Trophoblastic Disease - Co-HidalgoMeg MisaNo ratings yet
- Gestational Trophoblastic Disease (GTD) : Ahmed Refaat Abd ElzaherDocument41 pagesGestational Trophoblastic Disease (GTD) : Ahmed Refaat Abd ElzaherJessica NadiaNo ratings yet
- Mola HidatidosaDocument53 pagesMola HidatidosaJeanyanty Yoesteyn DjaranjoeraNo ratings yet
- OB ComplicDocument103 pagesOB ComplicmanilynNo ratings yet
- RHD & H - Mole - Case PresDocument90 pagesRHD & H - Mole - Case PresGhra CiousNo ratings yet
- MCQ's 3 Flashcards - QuizletDocument12 pagesMCQ's 3 Flashcards - Quizletbmhsh100% (1)
- Parental Chromosomal Abnormalities Uterine Abnormalities (Anatomical) Immunological EndocrineDocument4 pagesParental Chromosomal Abnormalities Uterine Abnormalities (Anatomical) Immunological EndocrineShienna Marie SalvioNo ratings yet
- Application of Betty NeumanDocument22 pagesApplication of Betty NeumanMary Janet Pinili100% (2)
- Hormones Beta HCG - SerumDocument1 pageHormones Beta HCG - SerumsaniyaNo ratings yet
- Benign Gestational Trophoblastic DiseaseDocument31 pagesBenign Gestational Trophoblastic Diseaseبسيل أبوهلالNo ratings yet
- FSRH Guideline Emergency Contraception03dec2020 Amendedjuly2023 11julDocument68 pagesFSRH Guideline Emergency Contraception03dec2020 Amendedjuly2023 11julmirunahorgaNo ratings yet
- CHORIOCARCINOMADocument4 pagesCHORIOCARCINOMAShyn CieloNo ratings yet
- Reproductive Arranged (MedicalBooksVN - Com)Document63 pagesReproductive Arranged (MedicalBooksVN - Com)Rabooh AyashiNo ratings yet
- Hydatidiform MoleDocument17 pagesHydatidiform MoleRizzamwah Catague0% (1)
- Gestational Trophoblastic DiseaseDocument7 pagesGestational Trophoblastic DiseaseChristine Evan HoNo ratings yet
- 3 CH 19 20 High Risk PregnancyDocument20 pages3 CH 19 20 High Risk PregnancyabyNo ratings yet
- Nidhi Blood ReportDocument1 pageNidhi Blood ReportSmitha GowdaNo ratings yet
- Ectopic Pregnancy H Mole Posted Jan 10 2024Document10 pagesEctopic Pregnancy H Mole Posted Jan 10 2024hsgarolacanNo ratings yet
- Gestational Choriocarcinoma OranuDocument8 pagesGestational Choriocarcinoma Oranuapi-3705046No ratings yet
- 2-Complications of Pregnancy Pt1Document37 pages2-Complications of Pregnancy Pt1pavi7muruganathanNo ratings yet
- Gestational Trophoblastic DiseaseDocument25 pagesGestational Trophoblastic Diseaseapi-3705046100% (1)
- C2b - Hydatidiform Mole (H-Mole Pregnancy) ContentDocument4 pagesC2b - Hydatidiform Mole (H-Mole Pregnancy) ContentGLADYS MAY GUDELOS MEJIASNo ratings yet
- Management and Therapy of Early Pregnancy Complication PDFDocument367 pagesManagement and Therapy of Early Pregnancy Complication PDFGopal Kumar DasNo ratings yet
- Hydatidiform Mole/ Molar Pregnancy: College of Health SciencesDocument11 pagesHydatidiform Mole/ Molar Pregnancy: College of Health SciencesAngelu Gabrielle CastroNo ratings yet
- Hydatidiform MoleDocument2 pagesHydatidiform MoleIrfan HardiNo ratings yet
- Ectopic and Molar PregnancyDocument22 pagesEctopic and Molar Pregnancyapi-381845148No ratings yet























































































Download as pptx, pdf, or txt
You might also like
- Malawi 2014 Malawi Obstetric and Gynaecology Protocols GuidelinesDocument105 pagesMalawi 2014 Malawi Obstetric and Gynaecology Protocols GuidelinesHải Ly Đào67% (3)
- Pituitary Tumors: A Clinical CasebookFrom EverandPituitary Tumors: A Clinical CasebookLisa B. NachtigallNo ratings yet
- Gestational Trophoblastic Tumours UG LECT.Document70 pagesGestational Trophoblastic Tumours UG LECT.TiwiNo ratings yet
- Gestational Trophoblastic Disease - OBS & GYN NOTESDocument52 pagesGestational Trophoblastic Disease - OBS & GYN NOTESNagulan ChanemougameNo ratings yet
- Setelah Mengikuti Kuliah Faham 1/2: Faham Hormon2: FSH, LH, E2, Testosteron Human Chorionic GonadotropinDocument32 pagesSetelah Mengikuti Kuliah Faham 1/2: Faham Hormon2: FSH, LH, E2, Testosteron Human Chorionic Gonadotropinruth thauladanNo ratings yet
- Testing During Pregnancy: David G. Grenache, PHD University of Utah & Arup Laboratories Salt Lake City, UtDocument54 pagesTesting During Pregnancy: David G. Grenache, PHD University of Utah & Arup Laboratories Salt Lake City, Utمحمد عمران راناNo ratings yet
- Gestational Trophoblastic DiseaseDocument37 pagesGestational Trophoblastic DiseaseOlisa 'phage' Onyebuchi100% (1)
- Graviditas: Faham Hormon2: FSH, LH, E2, Testosteron Human Chorionic GonadotropinDocument32 pagesGraviditas: Faham Hormon2: FSH, LH, E2, Testosteron Human Chorionic Gonadotropinruth thauladanNo ratings yet
- 。18. Molar PregnancyDocument29 pages。18. Molar Pregnancygenaong2003No ratings yet
- Molar Pregnancy & ChoriocarcinomaDocument16 pagesMolar Pregnancy & ChoriocarcinomaIbrahim JameelallaNo ratings yet
- Hydatidiform MoleDocument38 pagesHydatidiform Molesushma silwalNo ratings yet
- Gestational Trophoblastic Diseases (GTD)Document39 pagesGestational Trophoblastic Diseases (GTD)moreen kipkemoiNo ratings yet
- Ectopi C PregnancyDocument28 pagesEctopi C PregnancySazzad HossainNo ratings yet
- Diagnosis of PregnancyDocument23 pagesDiagnosis of PregnancyNeelesh BhandariNo ratings yet
- Gestational Trophoblastic Disease: Prepared By: Nikita PatelDocument20 pagesGestational Trophoblastic Disease: Prepared By: Nikita PatelVaishaliNo ratings yet
- Elevated Beta Human Chorionic Gonadotropin in A Non-Pregnant Female Diagnosed With Anal Squamous Cell CarcinomaDocument4 pagesElevated Beta Human Chorionic Gonadotropin in A Non-Pregnant Female Diagnosed With Anal Squamous Cell CarcinomaKatherine Elizabeth Urbina QuispeNo ratings yet
- 2b Case StudyDocument5 pages2b Case StudyCkaye MontilNo ratings yet
- Pregnancy Handbook: "Am I Pregnant?" All B-HCG Levels ExplainedDocument74 pagesPregnancy Handbook: "Am I Pregnant?" All B-HCG Levels ExplainedDr0Web100% (1)
- Pregnancytests 180321025548Document51 pagesPregnancytests 180321025548Dorin PathakNo ratings yet
- Kuliah PK2 TESKehamilanJULI2010Document38 pagesKuliah PK2 TESKehamilanJULI2010Fetty NataliaNo ratings yet
- Abnormal Uterine BleedingDocument46 pagesAbnormal Uterine BleedingNur Aliah Amirah AmranNo ratings yet
- H MoleDocument71 pagesH MoleDoc AchondoNo ratings yet
- With DR WajeihDocument62 pagesWith DR WajeihZeeshan AhmedNo ratings yet
- Fertility: Assessment and Treatment For People With Fertility ProblemsDocument4 pagesFertility: Assessment and Treatment For People With Fertility ProblemsPatrick CoghlanNo ratings yet
- (Hich2) Recurrent Pregnancy LossDocument33 pages(Hich2) Recurrent Pregnancy LossAli B. SafadiNo ratings yet
- Beta HCGDocument23 pagesBeta HCGpawchanNo ratings yet
- Transient Thyrotoxicosis in Molar PregnancyDocument2 pagesTransient Thyrotoxicosis in Molar PregnancyWilliam OttoNo ratings yet
- Menstrual Disorders and PCOS Webinar EMBRYO FKUI 2022Document49 pagesMenstrual Disorders and PCOS Webinar EMBRYO FKUI 2022angelinputri100% (1)
- CCD Obstetric GynecologyDocument43 pagesCCD Obstetric GynecologyHanif GandohNo ratings yet
- Sero FullDocument30 pagesSero Fullmihret geneneNo ratings yet
- Thyroid and ReproductionDocument42 pagesThyroid and Reproductionabraham winartoNo ratings yet
- Gestational Trophoblastic DiseasesDocument37 pagesGestational Trophoblastic DiseasesEdwin OkonNo ratings yet
- Follicle Stimulating HormoneDocument13 pagesFollicle Stimulating HormoneAgustinus SuryaNo ratings yet
- NurseryDocument30 pagesNurserymirandaNo ratings yet
- Determination of Hormones: Mohamed A.Ali BSC - HLS, Admls, DmlsDocument43 pagesDetermination of Hormones: Mohamed A.Ali BSC - HLS, Admls, Dmlsmoha3liNo ratings yet
- Pregnancy Test and Semen Analysis PDFDocument8 pagesPregnancy Test and Semen Analysis PDFबुद्ध मोक्तानNo ratings yet
- 5 PcosDocument67 pages5 PcosyewollolijfikreNo ratings yet
- Polycystic OvaryDocument25 pagesPolycystic OvaryAli AbdElnaby SalimNo ratings yet
- Hydatidiform MoleDocument5 pagesHydatidiform MoleReynaldo SutantoNo ratings yet
- Assisted Reproductive TechniquesDocument146 pagesAssisted Reproductive TechniquesGouravNo ratings yet
- Tumor Markers Some Laboratory Aspects of Pregnancy Cerebrospinal Fluid AnalysisDocument40 pagesTumor Markers Some Laboratory Aspects of Pregnancy Cerebrospinal Fluid AnalysisMans FansNo ratings yet
- Seminar Gestational Trophoblastic DiseaseDocument27 pagesSeminar Gestational Trophoblastic Diseasehusnajihah18No ratings yet
- Activity No. 10 Qualitative HCG DeterminationDocument9 pagesActivity No. 10 Qualitative HCG DeterminationCruz JenniferNo ratings yet
- 3 Investigation & Management of Ectopic PregnancyDocument38 pages3 Investigation & Management of Ectopic PregnancyMegavarnen GobinathanNo ratings yet
- AbortionDocument32 pagesAbortionD & S SeriesNo ratings yet
- Pregnancy DXDocument20 pagesPregnancy DXyewollolijfikreNo ratings yet
- Thrombophilia: Duha Alharbi, MD InternDocument30 pagesThrombophilia: Duha Alharbi, MD InternabrarNo ratings yet
- Acute Parenchymal Liver DiseaseDocument29 pagesAcute Parenchymal Liver Diseasejeevan ghimireNo ratings yet
- Hormones of The PlacentaDocument75 pagesHormones of The PlacentaAbdikadir AhmedNo ratings yet
- HCG Strip (OneStep)Document2 pagesHCG Strip (OneStep)Rita WidaningsihNo ratings yet
- PIDC Grand Round FinalDocument32 pagesPIDC Grand Round Finalhailu henockNo ratings yet
- Hormones of The PlacentaDocument67 pagesHormones of The PlacentagibreilNo ratings yet
- DiscussionDocument28 pagesDiscussionJee AmanteNo ratings yet
- Quantitative and QualitativeDocument4 pagesQuantitative and QualitativekukadiyaNo ratings yet
- Ahmed Mohamed Abdel Rahim Rammah: Senior Registrar Obstetrics and Gynecology Department Al - Adan Hospital, KuwaitDocument32 pagesAhmed Mohamed Abdel Rahim Rammah: Senior Registrar Obstetrics and Gynecology Department Al - Adan Hospital, Kuwaithossam626No ratings yet
- BVGH-University of Rwanda Virtual Gynecologic Oncology CourseDocument43 pagesBVGH-University of Rwanda Virtual Gynecologic Oncology CourseEmmanuel NdikuryayoNo ratings yet
- Precociou S Puberty: BY Vishnupriya Ravimohandoss Year-6 Group-1Document31 pagesPrecociou S Puberty: BY Vishnupriya Ravimohandoss Year-6 Group-1Priya RaviNo ratings yet
- Comportamiento de La Gonadotropina en El Embarazo 240308 192849Document10 pagesComportamiento de La Gonadotropina en El Embarazo 240308 192849VictorRojasNo ratings yet
- Biochemical Investigation of Infertile Couple-My PresentationDocument91 pagesBiochemical Investigation of Infertile Couple-My PresentationOlukoyejo OluwaboriNo ratings yet
- Precocious PubertyDocument4 pagesPrecocious PubertyHa Jae kyeongNo ratings yet
- 2nd Trimester BleedingDocument50 pages2nd Trimester BleedingRaiden VizcondeNo ratings yet
- Jurnal Mola HidatidosaDocument8 pagesJurnal Mola HidatidosaDebby SofianaNo ratings yet
- Abnormal Obstetrics EditedDocument11 pagesAbnormal Obstetrics EditedAbhie Gayle Erbon AbonallaNo ratings yet
- (GYNE) 3.05 Gestational Trophoblastic Disease - Co-HidalgoDocument7 pages(GYNE) 3.05 Gestational Trophoblastic Disease - Co-HidalgoMeg MisaNo ratings yet
- Gestational Trophoblastic Disease (GTD) : Ahmed Refaat Abd ElzaherDocument41 pagesGestational Trophoblastic Disease (GTD) : Ahmed Refaat Abd ElzaherJessica NadiaNo ratings yet
- Mola HidatidosaDocument53 pagesMola HidatidosaJeanyanty Yoesteyn DjaranjoeraNo ratings yet
- OB ComplicDocument103 pagesOB ComplicmanilynNo ratings yet
- RHD & H - Mole - Case PresDocument90 pagesRHD & H - Mole - Case PresGhra CiousNo ratings yet
- MCQ's 3 Flashcards - QuizletDocument12 pagesMCQ's 3 Flashcards - Quizletbmhsh100% (1)
- Parental Chromosomal Abnormalities Uterine Abnormalities (Anatomical) Immunological EndocrineDocument4 pagesParental Chromosomal Abnormalities Uterine Abnormalities (Anatomical) Immunological EndocrineShienna Marie SalvioNo ratings yet
- Application of Betty NeumanDocument22 pagesApplication of Betty NeumanMary Janet Pinili100% (2)
- Hormones Beta HCG - SerumDocument1 pageHormones Beta HCG - SerumsaniyaNo ratings yet
- Benign Gestational Trophoblastic DiseaseDocument31 pagesBenign Gestational Trophoblastic Diseaseبسيل أبوهلالNo ratings yet
- FSRH Guideline Emergency Contraception03dec2020 Amendedjuly2023 11julDocument68 pagesFSRH Guideline Emergency Contraception03dec2020 Amendedjuly2023 11julmirunahorgaNo ratings yet
- CHORIOCARCINOMADocument4 pagesCHORIOCARCINOMAShyn CieloNo ratings yet
- Reproductive Arranged (MedicalBooksVN - Com)Document63 pagesReproductive Arranged (MedicalBooksVN - Com)Rabooh AyashiNo ratings yet
- Hydatidiform MoleDocument17 pagesHydatidiform MoleRizzamwah Catague0% (1)
- Gestational Trophoblastic DiseaseDocument7 pagesGestational Trophoblastic DiseaseChristine Evan HoNo ratings yet
- 3 CH 19 20 High Risk PregnancyDocument20 pages3 CH 19 20 High Risk PregnancyabyNo ratings yet
- Nidhi Blood ReportDocument1 pageNidhi Blood ReportSmitha GowdaNo ratings yet
- Ectopic Pregnancy H Mole Posted Jan 10 2024Document10 pagesEctopic Pregnancy H Mole Posted Jan 10 2024hsgarolacanNo ratings yet
- Gestational Choriocarcinoma OranuDocument8 pagesGestational Choriocarcinoma Oranuapi-3705046No ratings yet
- 2-Complications of Pregnancy Pt1Document37 pages2-Complications of Pregnancy Pt1pavi7muruganathanNo ratings yet
- Gestational Trophoblastic DiseaseDocument25 pagesGestational Trophoblastic Diseaseapi-3705046100% (1)
- C2b - Hydatidiform Mole (H-Mole Pregnancy) ContentDocument4 pagesC2b - Hydatidiform Mole (H-Mole Pregnancy) ContentGLADYS MAY GUDELOS MEJIASNo ratings yet
- Management and Therapy of Early Pregnancy Complication PDFDocument367 pagesManagement and Therapy of Early Pregnancy Complication PDFGopal Kumar DasNo ratings yet
- Hydatidiform Mole/ Molar Pregnancy: College of Health SciencesDocument11 pagesHydatidiform Mole/ Molar Pregnancy: College of Health SciencesAngelu Gabrielle CastroNo ratings yet
- Hydatidiform MoleDocument2 pagesHydatidiform MoleIrfan HardiNo ratings yet
- Ectopic and Molar PregnancyDocument22 pagesEctopic and Molar Pregnancyapi-381845148No ratings yet