Download as ppt, pdf, or txt
You might also like
- Biochemical Markers of Bone Metabolism PPT LectureDocument89 pagesBiochemical Markers of Bone Metabolism PPT LectureNeil Vincent De AsisNo ratings yet
- Calcium & Phosphorus AnishDocument52 pagesCalcium & Phosphorus AnishAnish JoshiNo ratings yet
- HyperparathyroidismDocument23 pagesHyperparathyroidismSivajothyNo ratings yet
- EndocrinologyDocument34 pagesEndocrinologymiyuchix100% (2)
- I Clone 7Document1,164 pagesI Clone 7FERNANDO VELASCO100% (3)
- Disorders of The Parathyroid GlandsDocument30 pagesDisorders of The Parathyroid Glandsikram ullah khan100% (1)
- Parathyroid DisordersDocument37 pagesParathyroid DisordersMannat ZaidiNo ratings yet
- The Parathyroid Gland: DR - Umalkhayr Omar, MDDocument36 pagesThe Parathyroid Gland: DR - Umalkhayr Omar, MDgibreilNo ratings yet
- The Parathyroid GlandDocument66 pagesThe Parathyroid GlandMohammed GamalNo ratings yet
- Parathyroid DiseaseDocument10 pagesParathyroid Diseasemohammedghassan53No ratings yet
- Disorders of Parathyroid GlandDocument36 pagesDisorders of Parathyroid GlandJamesNo ratings yet
- Hiperparatiroid: Dr. Dr. Shahrul Rahman, SP - PD, FINASIMDocument50 pagesHiperparatiroid: Dr. Dr. Shahrul Rahman, SP - PD, FINASIMBonitavanyNo ratings yet
- Parathyroid DisordersDocument44 pagesParathyroid DisordersBIAN ALKHAZMARI100% (1)
- Lec#49 Calcium DisordersDocument105 pagesLec#49 Calcium DisordersKhaldoun AlmomaniNo ratings yet
- Vitamin DDocument25 pagesVitamin DSyeda AlizaNo ratings yet
- Parathyroid GlandsDocument17 pagesParathyroid GlandsMalik TamimiNo ratings yet
- Parathyroid Disordorders: By: Garmyan YawarDocument36 pagesParathyroid Disordorders: By: Garmyan Yawarsarhang talebaniNo ratings yet
- Parathyroid DiseaseDocument29 pagesParathyroid DiseaseTara AzadNo ratings yet
- Calcium Metabolism-Board Questions 2018: Azar Khosravi April 2018Document55 pagesCalcium Metabolism-Board Questions 2018: Azar Khosravi April 2018Abdullah SiddiqiNo ratings yet
- HiperparatiroidDocument15 pagesHiperparatiroidDoni PrasetioNo ratings yet
- Hypocalcemia: Dr. Nicolette Du Plessis Department PaediatricsDocument40 pagesHypocalcemia: Dr. Nicolette Du Plessis Department PaediatricsBharath Reddy DNo ratings yet
- Hypercalcemia: Bibek Ghimire 3 Batch, PAHSDocument25 pagesHypercalcemia: Bibek Ghimire 3 Batch, PAHSBibek GhimireNo ratings yet
- Parathyroid GlandsDocument4 pagesParathyroid GlandsMary Grace Buscargas PolancosNo ratings yet
- 2 - Parathyroid GlandDocument21 pages2 - Parathyroid Glandtaha55860No ratings yet
- Disorders of Calcium and Phosphate MetabolismDocument20 pagesDisorders of Calcium and Phosphate MetabolismAli TawbeNo ratings yet
- 0815 Skugor HyperAndHypocalcemiaDocument79 pages0815 Skugor HyperAndHypocalcemiaSirNorman BalinoNo ratings yet
- Aminoacid MetabolismDocument25 pagesAminoacid MetabolismMischief ManagerNo ratings yet
- Parathyroid, HyperparathyroidismDocument4 pagesParathyroid, Hyperparathyroidismjamil aoudeNo ratings yet
- Parathyroid Gland Diseases: Classification of Diseases of PTGDocument11 pagesParathyroid Gland Diseases: Classification of Diseases of PTGgashbin latifNo ratings yet
- Acid base balanceDocument60 pagesAcid base balanceburagohainaviNo ratings yet
- Disorders of Parathyroid Gland: by DR Irum Siddiquie PGR PediatricsDocument54 pagesDisorders of Parathyroid Gland: by DR Irum Siddiquie PGR PediatricsJamesNo ratings yet
- Hyperparathyroidism and HypoparathyroidismDocument44 pagesHyperparathyroidism and Hypoparathyroidismshweta singhNo ratings yet
- HYPOCALCEMIADocument27 pagesHYPOCALCEMIAJeffri SetiawanNo ratings yet
- Hyper para Thyroid Is MDocument3 pagesHyper para Thyroid Is MAriefNo ratings yet
- Hyper para Thyroid Is MDocument13 pagesHyper para Thyroid Is MRismaya NovitasariNo ratings yet
- LEC 3 Parathyroid Gland DisordersDocument39 pagesLEC 3 Parathyroid Gland Disordersalhusien.abd2000No ratings yet
- Disorders of Parathyroid Gland: BY: Dr. Rakesh Dr. Karthik Dr. Soumya BY: Dr. Rakesh Dr. Karthik Dr. SoumyaDocument59 pagesDisorders of Parathyroid Gland: BY: Dr. Rakesh Dr. Karthik Dr. Soumya BY: Dr. Rakesh Dr. Karthik Dr. SoumyaAirdorid LoginidNo ratings yet
- Parathyroid Glands: Serum PTH Levels Are Inappropriately Elevated For The LevelDocument4 pagesParathyroid Glands: Serum PTH Levels Are Inappropriately Elevated For The LevelNada MuchNo ratings yet
- Endocrine Physiology - Part 3 Parathyroid GlandDocument30 pagesEndocrine Physiology - Part 3 Parathyroid GlandTerrence Beniasi CharumbiraNo ratings yet
- Disorders of Calcium and Phosphate MetabolismDocument20 pagesDisorders of Calcium and Phosphate MetabolismAhmed Noureldin AhmedNo ratings yet
- Paratiroid Dan KalsiumDocument80 pagesParatiroid Dan KalsiumFebrina EvaNo ratings yet
- Parathyroid Glands: Presented By: Dr. Mohammed Alshehri Pgy2Document28 pagesParathyroid Glands: Presented By: Dr. Mohammed Alshehri Pgy2Omar Alruwaili100% (1)
- Hypercalcemia Secondary To Primary HyperparathyroidismDocument26 pagesHypercalcemia Secondary To Primary HyperparathyroidismClaudia IrimieNo ratings yet
- Hypocalcaemia: Done By: Saja Dmour Supervised By: DR. Ahmad MdallalDocument16 pagesHypocalcaemia: Done By: Saja Dmour Supervised By: DR. Ahmad Mdallalraed faisalNo ratings yet
- ParathyroidDocument24 pagesParathyroidLeonard AcsinteNo ratings yet
- Parathyroid GlandsDocument3 pagesParathyroid GlandsStrong Woman Bong SoonNo ratings yet
- Hypocalcemia: Dept of Nephrology PsriDocument40 pagesHypocalcemia: Dept of Nephrology Psriind78No ratings yet
- Hypo and Hyper ParathyrodismDocument31 pagesHypo and Hyper ParathyrodismJazh AyochokNo ratings yet
- Diseases of The Parathyroid GlandDocument60 pagesDiseases of The Parathyroid GlandRuDy RaviNo ratings yet
- HyperparathyroidismDocument15 pagesHyperparathyroidismMuhamad ZulfiqarNo ratings yet
- Disorders of Parathyroid GlandsDocument52 pagesDisorders of Parathyroid GlandsDr. Akash GuptaNo ratings yet
- FE2 OutlineDocument9 pagesFE2 Outlineapi-3697326No ratings yet
- Pathology of Parathyrid Gland FinalDocument63 pagesPathology of Parathyrid Gland FinalGurpreet Kaur SagooNo ratings yet
- Name Olusegun SDocument10 pagesName Olusegun SIsrael OlusegunNo ratings yet
- Disorders of The Thyroid and Parathyroid Glands: Ms TeamDocument36 pagesDisorders of The Thyroid and Parathyroid Glands: Ms TeamShy Dela PuertaNo ratings yet
- HyperparaDocument5 pagesHyperparaMaria Christina Paola CariñoNo ratings yet
- Primary HyperparathyroidismDocument13 pagesPrimary Hyperparathyroidismqayyum consultantfpscNo ratings yet
- Anaesthesia in Parathyroid Gland DisordersDocument25 pagesAnaesthesia in Parathyroid Gland DisordersAshiyan IrfanNo ratings yet
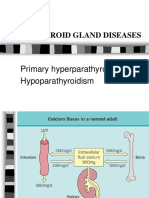
- Parathyroid Gland Diseases: Primary Hyperparathyroidism HypoparathyroidismDocument25 pagesParathyroid Gland Diseases: Primary Hyperparathyroidism HypoparathyroidismZahrah El FaradisaNo ratings yet
- HiperparatiroidDocument23 pagesHiperparatiroidrahmaNo ratings yet
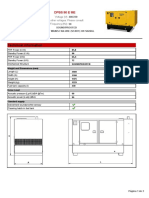
- Technical Information: Dpbs 90 E MeDocument3 pagesTechnical Information: Dpbs 90 E MeЛулу ТраедNo ratings yet
- Lab Report 7Document7 pagesLab Report 7Iena KasimNo ratings yet
- Se4 Rocker ArmDocument5 pagesSe4 Rocker ArmfkldjgkdljglkfjdlNo ratings yet
- JSW New Final ProjetDocument48 pagesJSW New Final ProjetRajender SinghNo ratings yet
- Definition of The CaribbeanDocument2 pagesDefinition of The CaribbeanBrianna AllenNo ratings yet
- Ebook Ebook PDF Principles of Human Physiology 6th Edition PDFDocument41 pagesEbook Ebook PDF Principles of Human Physiology 6th Edition PDFdonita.nichols650100% (43)
- Nabl 126Document31 pagesNabl 126Gazal GuptaNo ratings yet
- NTP 2020 Kakatiya - Mega - Textile - ParkDocument2 pagesNTP 2020 Kakatiya - Mega - Textile - ParkNv MannaNo ratings yet
- 10 Herbal Medicines Approved by The DohDocument13 pages10 Herbal Medicines Approved by The DohLark SantiagoNo ratings yet
- Lo2012 TPFDocument114 pagesLo2012 TPFramjoceNo ratings yet
- ProjectDocument13 pagesProjectAkshat UniyalNo ratings yet
- Solve System of Equations Using GraphingDocument42 pagesSolve System of Equations Using Graphingapi-265481804No ratings yet
- Fleming's Left Hand Rule (ForDocument8 pagesFleming's Left Hand Rule (Forb_geyl4286No ratings yet
- S.No Description Qty Unit Assumed by HWPL: Scope of Work - Supply PSSDocument14 pagesS.No Description Qty Unit Assumed by HWPL: Scope of Work - Supply PSSASR REDDYNo ratings yet
- Introducing MPLS Traffic Engineering Components-L01Document35 pagesIntroducing MPLS Traffic Engineering Components-L01Cuong HaNo ratings yet
- Bodie Investments 12e IM CH27Document3 pagesBodie Investments 12e IM CH27lexon_kbNo ratings yet
- Datasheet LTH-1550-01Document4 pagesDatasheet LTH-1550-01AntonellaBogadoNo ratings yet
- EE 413-Engg ElectromagneticsDocument2 pagesEE 413-Engg ElectromagneticsVan GonzalesNo ratings yet
- 14th Jan 330pm NuptialsDocument30 pages14th Jan 330pm Nuptialsvivsubs18No ratings yet
- The Hamburger Ate Boy Isn't Acceptable (Odd) But The Boy Ate The Hamburger Is Hamburger Doesn't Have This Property and The Noun Boy DoesDocument6 pagesThe Hamburger Ate Boy Isn't Acceptable (Odd) But The Boy Ate The Hamburger Is Hamburger Doesn't Have This Property and The Noun Boy DoesDania SaviraNo ratings yet
- Wallace Stevens - Thirteen Ways of Looking at A BlackbirdDocument1 pageWallace Stevens - Thirteen Ways of Looking at A Blackbirdba belNo ratings yet
- Chapter 03-A - 20111108094508Document29 pagesChapter 03-A - 20111108094508Heri YantiNo ratings yet
- Air System - Atlas Copco FX 1 Instruction Book (Page 13) - ManualsLibDocument1 pageAir System - Atlas Copco FX 1 Instruction Book (Page 13) - ManualsLibYoseph EdyNo ratings yet
- PCS Manager Job DescriptionDocument3 pagesPCS Manager Job DescriptionravirajabNo ratings yet
- 2019 JC2 H2 Physics Anderson Serangoon Junior CollegeDocument90 pages2019 JC2 H2 Physics Anderson Serangoon Junior Collegeeternal vorceNo ratings yet
- Metabolit SekunderDocument76 pagesMetabolit SekunderCempaka Kusuma DewiNo ratings yet
- Sig Decomp MproxDocument60 pagesSig Decomp MproxOri CarmiNo ratings yet
- Practice Question Ffor Module 7Document6 pagesPractice Question Ffor Module 7hemkumar DahalNo ratings yet
- Page Proofs: Continuous Probability DistributionsDocument44 pagesPage Proofs: Continuous Probability DistributionsApoorva PanchalNo ratings yet