Download as pptx, pdf, or txt
You might also like
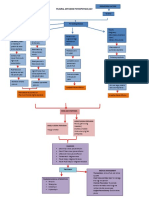
- Pleurl Effusion Pathophysiology DiagramDocument2 pagesPleurl Effusion Pathophysiology DiagramAkiraMamo67% (3)
- Chapter Practice Test: Home Chapter 22: The Respiratory SystemDocument4 pagesChapter Practice Test: Home Chapter 22: The Respiratory SystemHUAWEI HUAWEINo ratings yet
- Oxygen TherapyDocument44 pagesOxygen TherapyChhabilal BastolaNo ratings yet
- Pre-Lab Questions:: Deep Breathing & Coughing Exercises Oxygen TherapyDocument3 pagesPre-Lab Questions:: Deep Breathing & Coughing Exercises Oxygen TherapyaliNo ratings yet
- Oxygen Therapy: Prepared By: Moza Sulaiman Rashid Al-KaldiDocument31 pagesOxygen Therapy: Prepared By: Moza Sulaiman Rashid Al-Kaldimoza92sNo ratings yet
- Oxygen TherapyDocument24 pagesOxygen TherapyXavier EstalloNo ratings yet
- 5 Oxygen Therapy& DevicesDocument73 pages5 Oxygen Therapy& Devicesdrnasir31No ratings yet
- COPDDocument42 pagesCOPDAnoos rabayarabayaNo ratings yet
- Oxygen TherapyDocument20 pagesOxygen TherapyBeri NyuydzefonNo ratings yet
- Oxygen Therapy 2012Document34 pagesOxygen Therapy 2012Niko KautsarNo ratings yet
- OxygenotherapyDocument20 pagesOxygenotherapyrobcaleb123No ratings yet
- 2 O2 Therapy 2021Document58 pages2 O2 Therapy 2021Marceline GarciaNo ratings yet
- Oxygen TherapyDocument14 pagesOxygen TherapyELISION OFFICIALNo ratings yet
- Oxygen 2222Document19 pagesOxygen 2222Salim AlmetewtyNo ratings yet
- Oxygen Therapy, Trach Care and SuctioningDocument44 pagesOxygen Therapy, Trach Care and SuctioningEmily Boehmer100% (1)
- Medical Gas TherapyDocument84 pagesMedical Gas TherapyJohn Carlo TanNo ratings yet
- Oxygen TherapyDocument5 pagesOxygen TherapyReena MathewNo ratings yet
- Sarabjit SeminarDocument290 pagesSarabjit SeminarparmeshoriNo ratings yet
- Care of Clients With Problems in OxygenationDocument8 pagesCare of Clients With Problems in OxygenationRed StohlNo ratings yet
- 1 6 - Oxygen-TherapyDocument62 pages1 6 - Oxygen-TherapyJUSTIN ALZATENo ratings yet
- Administering Oxygen Therapy Powerpoint 3Document58 pagesAdministering Oxygen Therapy Powerpoint 3RajaNo ratings yet
- Care of Client With Oxygenation Problem: SEPTEMBER 9-10,2021Document22 pagesCare of Client With Oxygenation Problem: SEPTEMBER 9-10,2021Ong KarlNo ratings yet
- Oxygen TherapyDocument8 pagesOxygen TherapyElmoi DoguilesNo ratings yet
- Oxygen Delivery Devices: Getting Inspired AboutDocument4 pagesOxygen Delivery Devices: Getting Inspired AboutTubagus HidayatullahNo ratings yet
- OXYGENATION - Nov. 5Document85 pagesOXYGENATION - Nov. 5academic purposesNo ratings yet
- O2 AdministrationDocument35 pagesO2 AdministrationSakthi DeviNo ratings yet
- Asthama & COPDDocument84 pagesAsthama & COPDAbdullah BhattiNo ratings yet
- Systems Plus College Foundation Macarthur Highway, Balibago, Angeles CityDocument13 pagesSystems Plus College Foundation Macarthur Highway, Balibago, Angeles CityLeanne Princess GamboaNo ratings yet
- Oxygen TherapyDocument21 pagesOxygen TherapyScribdTranslationsNo ratings yet
- CODPDocument34 pagesCODPNeeraja M SureshNo ratings yet
- Basic Principles of Oxygen TherapyDocument20 pagesBasic Principles of Oxygen TherapyAdikurniawan100% (1)
- Oxygen TherapyDocument25 pagesOxygen TherapyIsaiah AmolatoNo ratings yet
- OxygenDocument34 pagesOxygenSamson AyalewNo ratings yet
- OxygenationcasestudyDocument6 pagesOxygenationcasestudyLee CelNo ratings yet
- Oxygen AdministrationDocument26 pagesOxygen AdministrationVichico Jane ZuluetaNo ratings yet
- Respiratory DiseasesDocument58 pagesRespiratory DiseasesSarahNo ratings yet
- Hyperbaric Oxygen and Oral and Maxillofacial SurgeryDocument59 pagesHyperbaric Oxygen and Oral and Maxillofacial SurgeryKassim OboghenaNo ratings yet
- Respiratory FailureDocument15 pagesRespiratory FailureKennedy Ng'andweNo ratings yet
- Basics of OxygenDocument78 pagesBasics of OxygenClarisse AcacioNo ratings yet
- Assessing Patients For Oxygen Therapy: Figure. I May Be Jus..Document4 pagesAssessing Patients For Oxygen Therapy: Figure. I May Be Jus..Angeline Monilla Pante100% (1)
- Oxygen TherapyDocument20 pagesOxygen TherapyPaul Gabriel CasquejoNo ratings yet
- Airway ManagementDocument30 pagesAirway ManagementFuad TalNo ratings yet
- Nclex Review Pneumonia COPD AsDocument11 pagesNclex Review Pneumonia COPD Asmj078No ratings yet
- Administering Oxygen Therapy Powerpoint 3Document58 pagesAdministering Oxygen Therapy Powerpoint 3reema_rt75% (8)
- Oxygen TherapyDocument31 pagesOxygen Therapymedical.student.messiNo ratings yet
- Oxygen TherapyDocument28 pagesOxygen TherapyMIR JALALNo ratings yet
- 418-M1-Cu 5 Resp. Emergencies 2Document12 pages418-M1-Cu 5 Resp. Emergencies 2Paradillo Regatuna LesterNo ratings yet
- Oxygenation and Orygen TherapyDocument87 pagesOxygenation and Orygen Therapyபிரேம் குமார் ராஜாமணிNo ratings yet
- Respiratory NeedsDocument24 pagesRespiratory NeedsJoyceNo ratings yet
- ARDSDocument28 pagesARDSKAMLESH RATHODNo ratings yet
- Chronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredDocument25 pagesChronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredOmar AbdillahiNo ratings yet
- Oxygen AdministrationDocument38 pagesOxygen AdministrationKate Angelique RodriguezNo ratings yet
- DrowningDocument9 pagesDrowningAkshata HingeNo ratings yet
- Oxygen Therapy: by DR Finny Theo, MBBS, (DNB)Document59 pagesOxygen Therapy: by DR Finny Theo, MBBS, (DNB)The Telugu DoctorNo ratings yet
- Impaired Gas ExchangeDocument4 pagesImpaired Gas ExchangeNuraini Hamzah100% (1)
- Terapi OksigenDocument21 pagesTerapi OksigenAlyssa Kp UnscioNo ratings yet
- Respiratory Distress SyndromeDocument30 pagesRespiratory Distress SyndromeDennis MiritiNo ratings yet
- OxygenationDocument50 pagesOxygenationLulu MushiNo ratings yet
- Oxygen Therapy Systems: NCM 107.1 Evangeline B. MananquilDocument48 pagesOxygen Therapy Systems: NCM 107.1 Evangeline B. Mananquilacademic purposesNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document23 pagesChronic Obstructive Pulmonary Disease (COPD)akoeljames8543No ratings yet
- A Simple Guide to Hypoxemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypoxemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- A Simple Guide to Oxygen Therapy, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Oxygen Therapy, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Ax PneumothoraxDocument8 pagesAx Pneumothoraxapi-3797941100% (2)
- SAMPLE NCP For PneumoniaDocument3 pagesSAMPLE NCP For Pneumoniakana_mercado100% (6)
- Pneumothorax: Algorithm: Queen's Dect: KGH BleepDocument2 pagesPneumothorax: Algorithm: Queen's Dect: KGH BleepRachmi Merrina0% (1)
- A-A Gradient (Fi02) (Pa02) (PA02) (Oxygenation)Document7 pagesA-A Gradient (Fi02) (Pa02) (PA02) (Oxygenation)Zach ShulmanNo ratings yet
- Chest Trauma: Nursing 410 Western Carolina University BSN ProgramDocument29 pagesChest Trauma: Nursing 410 Western Carolina University BSN ProgramShimmering MoonNo ratings yet
- CPDprogram RESPIRATORYTHERAPY-10918Document10 pagesCPDprogram RESPIRATORYTHERAPY-10918PRC BoardNo ratings yet
- (Ebook PDF) Kendig's Disorders of The Respiratory Tract in Children 9th Edition Robert W. Wilmott - Ebook PDF All ChapterDocument69 pages(Ebook PDF) Kendig's Disorders of The Respiratory Tract in Children 9th Edition Robert W. Wilmott - Ebook PDF All Chapterdjuveguigas100% (15)
- Transient Tachypnea of The Newborn EnglishDocument2 pagesTransient Tachypnea of The Newborn EnglishDyan Friska Yanty LbsNo ratings yet
- Internal MedicineDocument146 pagesInternal MedicineSh. RamNo ratings yet
- Automation of Mechanical VentilationDocument12 pagesAutomation of Mechanical VentilationjuanNo ratings yet
- Puritan Bennett Bi Level Breath Mode White PaperDocument12 pagesPuritan Bennett Bi Level Breath Mode White PaperEndar SulistyoNo ratings yet
- Hyperinflated LungsDocument10 pagesHyperinflated LungsGplsHub.comNo ratings yet
- A. 2021 22 Report From The Philippine College of Chest PhysiciansDocument15 pagesA. 2021 22 Report From The Philippine College of Chest PhysiciansDivye GuptaNo ratings yet
- Aviation MedicineDocument11 pagesAviation MedicineTrans Trades100% (1)
- Prof. Mohammad Khairy.... Symptoms & Signs of Chest DiseasesDocument121 pagesProf. Mohammad Khairy.... Symptoms & Signs of Chest DiseasesMans FansNo ratings yet
- Indicator Dilution Method of Blood Flow MeasurementDocument3 pagesIndicator Dilution Method of Blood Flow MeasurementabhilashkrishnantkNo ratings yet
- Nursing Care of Clients Nursing Care of Clients With Altered Ventilatory With Altered Ventilatory Function FunctionDocument179 pagesNursing Care of Clients Nursing Care of Clients With Altered Ventilatory With Altered Ventilatory Function FunctionPia Rose RoqueNo ratings yet
- Key Ventilation Specifications - MIT E-Vent - MIT Emergency VentilatorDocument2 pagesKey Ventilation Specifications - MIT E-Vent - MIT Emergency VentilatorArduinoPeru IotNo ratings yet
- Problem ListDocument2 pagesProblem List22 - Fernandez, Lyza Mae D.No ratings yet
- 08 10 Main3Document41 pages08 10 Main3Lindsey RobbinsNo ratings yet
- Airway ObstructionDocument7 pagesAirway ObstructionPrincess May Delos ReyesNo ratings yet
- PhysioEx Exercise 7 ActivityDocument3 pagesPhysioEx Exercise 7 ActivityCLAUDIA ELISABET BECERRA GONZALESNo ratings yet
- Status AsthmaticusDocument15 pagesStatus AsthmaticusDaianne Joy DonatoNo ratings yet
- The KISS Principle and How To Treat Lower Respiratory Tract DiseaseDocument8 pagesThe KISS Principle and How To Treat Lower Respiratory Tract DiseaseAndrew SordylNo ratings yet
- AsthmaDocument2 pagesAsthmaZyra AmbaganNo ratings yet
- Pneumothorax and Pneumomediastinum: Dr. Emad EfatDocument89 pagesPneumothorax and Pneumomediastinum: Dr. Emad Efatinterna MANADONo ratings yet
- Bunnell Life Pulse 204 Quick Reference GuideDocument12 pagesBunnell Life Pulse 204 Quick Reference GuideRafael RamirezNo ratings yet
- PhysiotherapyDocument1 pagePhysiotherapyFares EL DeenNo ratings yet