Download as pptx, pdf, or txt
You might also like
- Pediatric Infectious Disease - A Practically Painless Review (2015)Document213 pagesPediatric Infectious Disease - A Practically Painless Review (2015)Fajrin Ashari100% (2)
- Virus Hepatitis RevDocument83 pagesVirus Hepatitis RevSukma WinahyuNo ratings yet
- Viral InfectionsDocument59 pagesViral Infectionsrenato renatoNo ratings yet
- Hepatitis: Dr. Amany A. GhazyDocument44 pagesHepatitis: Dr. Amany A. GhazyJosé Luis García GarcíaNo ratings yet
- Part 2 of Medical VirologyDocument113 pagesPart 2 of Medical Virologygatete samNo ratings yet
- 1010 M Balm - Viral HepatitisDocument17 pages1010 M Balm - Viral HepatitisSaad KhanNo ratings yet
- 8.hepatitis VirusesDocument33 pages8.hepatitis VirusesShaibin MuhammadNo ratings yet
- Hepatitis A GDocument23 pagesHepatitis A Gapi-3712326No ratings yet
- Hepatitis Virus: Bagian Mikrobiologi FK UnissulaDocument36 pagesHepatitis Virus: Bagian Mikrobiologi FK UnissulaKarina Mega WNo ratings yet
- HepatitisDocument55 pagesHepatitisdebdeepbhattacharya411No ratings yet
- Presented By:-Himanshu Dev DMLT VI TH Sem. VMMC & SJHDocument55 pagesPresented By:-Himanshu Dev DMLT VI TH Sem. VMMC & SJHKailash Nagar100% (1)
- HepatitisDocument29 pagesHepatitisRose Anne AbivaNo ratings yet
- HepatitisDocument33 pagesHepatitisThomas UtomoNo ratings yet
- Viral Hepatitis Training Manual: Federal Ministry of Health National Hepatitis Control Program 2017Document44 pagesViral Hepatitis Training Manual: Federal Ministry of Health National Hepatitis Control Program 2017Eleni HagosNo ratings yet
- Hepatitis B & DDocument40 pagesHepatitis B & DMeena CtNo ratings yet
- 1 HepatitisDocument62 pages1 HepatitisKamal AhmedNo ratings yet
- Presented By:-Himanshu Dev DMLT VI TH Sem. VMMC & SJHDocument55 pagesPresented By:-Himanshu Dev DMLT VI TH Sem. VMMC & SJHwira guna pratiwiNo ratings yet
- HepatitisDocument19 pagesHepatitisDayana PrasanthNo ratings yet
- Hepatitis - An Overview: Dr. JayalakshmiDocument77 pagesHepatitis - An Overview: Dr. JayalakshmiNithin SundarNo ratings yet
- 15 HepatitisDocument48 pages15 HepatitisAlvin LaurenceNo ratings yet
- HEPATOBILIER Pemicu 2 AlfindraDocument107 pagesHEPATOBILIER Pemicu 2 AlfindraHartomas BumiharjoNo ratings yet
- Hepatitis Viruses: Dr. Muna. M. A. Yousif M.D Clinical MicrobiologyDocument45 pagesHepatitis Viruses: Dr. Muna. M. A. Yousif M.D Clinical MicrobiologyMAxeneNo ratings yet
- Infectious Gastrointestinal Diseases: MicrobiologyDocument37 pagesInfectious Gastrointestinal Diseases: MicrobiologyRakesh KumarNo ratings yet
- HIV&HepatitisDocument46 pagesHIV&HepatitisRaja RuzannaNo ratings yet
- Hepato-Billiary Diseases: Tutor: DR SocdaalDocument32 pagesHepato-Billiary Diseases: Tutor: DR SocdaalOmar mohamedNo ratings yet
- Hepatitis D Virus (HDV) : PathogenesisDocument30 pagesHepatitis D Virus (HDV) : PathogenesisJc GaldosNo ratings yet
- TASH CI HepatitisDocument47 pagesTASH CI HepatitisBeamlak Getachew WoldeselassieNo ratings yet
- Hepatitis A-E Viruses: An OverviewDocument49 pagesHepatitis A-E Viruses: An OverviewDeepak VermaNo ratings yet
- L3. Transfusion-Transmitted DiseasesDocument5 pagesL3. Transfusion-Transmitted Diseasesjmdimasacat9No ratings yet
- 05 Prevention of TransmissionDocument35 pages05 Prevention of TransmissionANUAR ASISNo ratings yet
- Virus Hepatitis - KBKDocument53 pagesVirus Hepatitis - KBKfifi anggraeniNo ratings yet
- Muhammad Asaad Maidin Departement Microbiology Faculty of Medicine Hasanuddin University, MakassarDocument54 pagesMuhammad Asaad Maidin Departement Microbiology Faculty of Medicine Hasanuddin University, MakassarPratiwi PurnamaNo ratings yet
- Viral Hepatitis (Virus Hepatitis)Document75 pagesViral Hepatitis (Virus Hepatitis)Ilmiah Bagus100% (1)
- Viral Hepatitis: Dr. Staar Mohammed QaderDocument60 pagesViral Hepatitis: Dr. Staar Mohammed QaderMohammed R.HusseinNo ratings yet
- Hepatitis A VirusDocument27 pagesHepatitis A VirusAna KarlaNo ratings yet
- Jaundice and Hepatitis in Children: Dr. MwendwaDocument46 pagesJaundice and Hepatitis in Children: Dr. MwendwaAlvin OmondiNo ratings yet
- Hepatitis A-EDocument34 pagesHepatitis A-EVer Garcera TalosigNo ratings yet
- Viral HepatitisDocument51 pagesViral HepatitisIlmiah BagusNo ratings yet
- Hepatitis Viruses: VIRUS:Hepatitis A, B, CDocument25 pagesHepatitis Viruses: VIRUS:Hepatitis A, B, Carisita firmanNo ratings yet
- Hepatitis FK 2008Document42 pagesHepatitis FK 2008Dokter KarisNo ratings yet
- Hepatitis A - Typhoid Fever - KBKDocument50 pagesHepatitis A - Typhoid Fever - KBKanggunNo ratings yet
- Viral HepatitisDocument58 pagesViral HepatitisKathrine SiahaanNo ratings yet
- Hepadna VirusesDocument30 pagesHepadna Virusesraymondvicent9No ratings yet
- Viral Hepatitis PC II 2023Document76 pagesViral Hepatitis PC II 2023Suhayb CumarNo ratings yet
- Hepatitis A, B and C VirusDocument46 pagesHepatitis A, B and C VirusChyzhi SylviaNo ratings yet
- Viral Hepatitis (Part I)Document12 pagesViral Hepatitis (Part I)Maarveen RajNo ratings yet
- HepatitisDocument51 pagesHepatitisriturajrastogibpt22-26No ratings yet
- Infeksi Virus Pada Sistem Pencernaan Bawah: Hepatitis: Ety AprilianaDocument27 pagesInfeksi Virus Pada Sistem Pencernaan Bawah: Hepatitis: Ety AprilianaAsmorowatiNo ratings yet
- HepatitisDocument24 pagesHepatitisAnn MariaNo ratings yet
- Acute Hepatitis DR NjokuDocument43 pagesAcute Hepatitis DR Njokufrankozed1No ratings yet
- Viral Hepatitis: Reading AssignmentDocument51 pagesViral Hepatitis: Reading AssignmentNadya VanessaNo ratings yet
- Viral Hepatitis For PhoDocument60 pagesViral Hepatitis For Phomehdikhalid09No ratings yet
- Viral Hepatitis: by Dimie Ogoina Internal Medicine Ndu/NduthDocument16 pagesViral Hepatitis: by Dimie Ogoina Internal Medicine Ndu/NduthPrincewill SeiyefaNo ratings yet
- Viral Hepatitis: DR - Abiy F. Nov 2019 Arsi UniversityDocument67 pagesViral Hepatitis: DR - Abiy F. Nov 2019 Arsi UniversityWakjira NigusuNo ratings yet
- HBV Si HCV Studenti 201 PDFDocument117 pagesHBV Si HCV Studenti 201 PDFDianaTricoracheNo ratings yet
- 3.0HEPATIT Lecture 5Document48 pages3.0HEPATIT Lecture 5Jiya MuhammadNo ratings yet
- Hepatitis A, D, E & GDocument28 pagesHepatitis A, D, E & GsaleemNo ratings yet
- Hep B VirusDocument20 pagesHep B VirusBhupesh ChandNo ratings yet
- 1hepatitis (HBV) 07Document47 pages1hepatitis (HBV) 07ganyetzNo ratings yet
- 2018 Hepatitis Viral InfectionDocument51 pages2018 Hepatitis Viral Infectionkomang nickoNo ratings yet
- Hepatitis B Virus and Liver DiseaseFrom EverandHepatitis B Virus and Liver DiseaseJia-Horng KaoNo ratings yet
- Annual_plan_of_cervical_cancer_screening_and_treatment_of_shabe (2)Document2 pagesAnnual_plan_of_cervical_cancer_screening_and_treatment_of_shabe (2)Mulugeta DagneNo ratings yet
- 1 IntroductionDocument32 pages1 IntroductionMulugeta DagneNo ratings yet
- iskorkaardii 2007Document123 pagesiskorkaardii 2007Mulugeta DagneNo ratings yet
- IFH GabasaaDocument11 pagesIFH GabasaaMulugeta DagneNo ratings yet
- Revised_Ethiopian_Health_Center_Reform_Basic_training_schedule_JuneDocument8 pagesRevised_Ethiopian_Health_Center_Reform_Basic_training_schedule_JuneMulugeta DagneNo ratings yet
- Behavior 1BDocument9 pagesBehavior 1BMulugeta DagneNo ratings yet
- Delegation of AuthorityDocument16 pagesDelegation of AuthorityMulugeta DagneNo ratings yet
- 06. Dr Bijoy Kar Infertility and IVF ReviewDocument20 pages06. Dr Bijoy Kar Infertility and IVF ReviewMulugeta DagneNo ratings yet
- 06 Privacy & ConfidentialityDocument22 pages06 Privacy & ConfidentialityMulugeta DagneNo ratings yet
- 1 - Introduction To Health ManagementDocument82 pages1 - Introduction To Health ManagementMulugeta DagneNo ratings yet
- ARVNurse Training WorkbookDocument57 pagesARVNurse Training WorkbookMulugeta DagneNo ratings yet
- Emotional IntelligenceDocument45 pagesEmotional IntelligenceMulugeta DagneNo ratings yet
- Hambiso PHCU SBC PlanDocument15 pagesHambiso PHCU SBC PlanMulugeta DagneNo ratings yet
- ARVNurse Training ManualDocument71 pagesARVNurse Training ManualMulugeta DagneNo ratings yet
- Comprehensive Visual Inspection of The Cervix With Acetic Acid (VIA) and Lugol's Iodine (VILI)Document1 pageComprehensive Visual Inspection of The Cervix With Acetic Acid (VIA) and Lugol's Iodine (VILI)Mulugeta DagneNo ratings yet
- Public Relations VECODDocument30 pagesPublic Relations VECODMulugeta DagneNo ratings yet
- Colposcopy and Treatment of Cervical Intraepithelial Neoplasia - A Beginners' ManualDocument10 pagesColposcopy and Treatment of Cervical Intraepithelial Neoplasia - A Beginners' ManualMulugeta DagneNo ratings yet
- Early Detection, Prevention, and Infections Branch (EPR) - IARCDocument5 pagesEarly Detection, Prevention, and Infections Branch (EPR) - IARCMulugeta DagneNo ratings yet
- Public Administration and BureaucracyDocument12 pagesPublic Administration and BureaucracyMulugeta DagneNo ratings yet
- Decision Making 11Document9 pagesDecision Making 11Mulugeta DagneNo ratings yet
- All Communication IPV2 Rota HPVDocument24 pagesAll Communication IPV2 Rota HPVMulugeta DagneNo ratings yet
- Record Management AdjestedDocument25 pagesRecord Management AdjestedMulugeta DagneNo ratings yet
- Assessment - Attempt ReviewDocument10 pagesAssessment - Attempt ReviewMulugeta DagneNo ratings yet
- General Frame WorkDocument85 pagesGeneral Frame WorkMulugeta DagneNo ratings yet
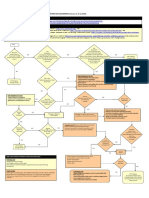
- VHF Algo PDFDocument1 pageVHF Algo PDFMulugeta DagneNo ratings yet
- Indicative Target TemplateDocument11 pagesIndicative Target TemplateMulugeta DagneNo ratings yet
- Challenge Rules and Eligibility - Million Hearts®Document6 pagesChallenge Rules and Eligibility - Million Hearts®Mulugeta DagneNo ratings yet
- SOAEMgt Urti PRNTDocument2 pagesSOAEMgt Urti PRNTMulugeta DagneNo ratings yet
- End of Life Care - Elearning For HealthcareDocument9 pagesEnd of Life Care - Elearning For HealthcareMulugeta DagneNo ratings yet
- 4.raggasaa Kabbadaa: Kan Ji'a Hagaya Bara 2012Document5 pages4.raggasaa Kabbadaa: Kan Ji'a Hagaya Bara 2012Mulugeta DagneNo ratings yet
- Symposium 11 - Irsan Hasan, Indonesia Management of Hepatitis B in Indonesia PDFDocument81 pagesSymposium 11 - Irsan Hasan, Indonesia Management of Hepatitis B in Indonesia PDFGiovani Purba100% (1)
- Scienceofwrestling PDFDocument46 pagesScienceofwrestling PDForpheusNo ratings yet
- High Seroprevalence and Factors Associated With Syphilis Infection A Snapshot From The HIV-Infected Pregnant Women Population in Mtwara, TanzaniaDocument9 pagesHigh Seroprevalence and Factors Associated With Syphilis Infection A Snapshot From The HIV-Infected Pregnant Women Population in Mtwara, TanzaniaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- UPHIA Uganda FactsheetDocument4 pagesUPHIA Uganda FactsheetWorld Health Organization, Uganda75% (4)
- CDC Healthcare Personnel Vaccination RecommendationsDocument1 pageCDC Healthcare Personnel Vaccination RecommendationsdocktpNo ratings yet
- Epidemiology and Prevention of Viral Hepatitis A To E:: An OverviewDocument36 pagesEpidemiology and Prevention of Viral Hepatitis A To E:: An OverviewJaylive AnziaNo ratings yet
- Principles of Molecular VirologyDocument8 pagesPrinciples of Molecular VirologyAJCannNo ratings yet
- Bds Third Professional Examination 2007 General Medicine (Seqs) Model PaperDocument15 pagesBds Third Professional Examination 2007 General Medicine (Seqs) Model PaperDania RiazNo ratings yet
- Digestive System PathophysiologyDocument16 pagesDigestive System PathophysiologyCamryn NewellNo ratings yet
- Covid or PuiDocument45 pagesCovid or PuiChristyl JoNo ratings yet
- Occupational Health Hazards and Workers' Health: Marissa G. Lomuntad - San Jose, MD, MOHDocument86 pagesOccupational Health Hazards and Workers' Health: Marissa G. Lomuntad - San Jose, MD, MOHAviects Avie JaroNo ratings yet
- Hepatitis BDocument48 pagesHepatitis BHari Suthan TNo ratings yet
- Medical Examination For An Australian Visa: CostsDocument9 pagesMedical Examination For An Australian Visa: CostsKHAIRUL REDZUANNo ratings yet
- Needle Stick and Sharp Injuries and Associated Factors Among Nurses Workingin Jimma University Specialized Hospital South West Ethiopia 2167 1168 1000291Document8 pagesNeedle Stick and Sharp Injuries and Associated Factors Among Nurses Workingin Jimma University Specialized Hospital South West Ethiopia 2167 1168 1000291MrLarry DolorNo ratings yet
- Ijms 20 01358Document24 pagesIjms 20 01358CHETAN SOMUNo ratings yet
- Dr. Noto ID HandoutDocument35 pagesDr. Noto ID HandoutSoleil DaddouNo ratings yet
- Training To Prevent Healthcare Associated InfectionsDocument12 pagesTraining To Prevent Healthcare Associated Infectionsarchana goswamiNo ratings yet
- Hepatitis B Virus Transmissions Associated With ADocument9 pagesHepatitis B Virus Transmissions Associated With AAyesha Nasir KhanNo ratings yet
- Journal Club Hepatitis BDocument45 pagesJournal Club Hepatitis BMadeeha ArifNo ratings yet
- BCAB - Ce Insert Rev.1 0713 EngDocument8 pagesBCAB - Ce Insert Rev.1 0713 EngSantiagoAFNo ratings yet
- Mei-Hwei Chang, Kathleen B. Schwarz - Viral Hepatitis in Children - Prevention and Management (2019, Springer Singapore)Document229 pagesMei-Hwei Chang, Kathleen B. Schwarz - Viral Hepatitis in Children - Prevention and Management (2019, Springer Singapore)Mădălina SuciuNo ratings yet
- Infection Control in AnaesthesiaDocument19 pagesInfection Control in AnaesthesiaSherifMohamedNo ratings yet
- Who CDS Cpe SMT 2001.13Document190 pagesWho CDS Cpe SMT 2001.13Thoko KavamgomoNo ratings yet
- Lecture 8 - SCI 8007SEF Medical Microbiology & Virology-Virology II - 2023Document76 pagesLecture 8 - SCI 8007SEF Medical Microbiology & Virology-Virology II - 2023YY CheungNo ratings yet
- Abnormal Liver Function TestsDocument6 pagesAbnormal Liver Function Testskronic12daniNo ratings yet
- READINGDocument21 pagesREADINGdiya baby100% (1)
- Etiologic Agent Means A Disease-Causing Agent. Hepatitis A - o - o o - o - oDocument5 pagesEtiologic Agent Means A Disease-Causing Agent. Hepatitis A - o - o o - o - ojin0meNo ratings yet
- Hepatitis B Prevention and ControlDocument19 pagesHepatitis B Prevention and Controlcolltfrank100% (1)
- Assessment and Management of Patients With Hepatic Disorder (Cruz)Document3 pagesAssessment and Management of Patients With Hepatic Disorder (Cruz)Mary Ruth CruzNo ratings yet