Download as ppt, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- ACLS Exam - A&B VersionsDocument36 pagesACLS Exam - A&B VersionsMohamed El-sayed100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Vitamin B12 DeficiencyDocument52 pagesVitamin B12 DeficiencyMohamed El-sayedNo ratings yet
- Blood Transfusion ReactionDocument38 pagesBlood Transfusion ReactionMohamed El-sayedNo ratings yet
- 8 - MRCP Part 1 - Recall May 2013Document28 pages8 - MRCP Part 1 - Recall May 2013Mohamed El-sayedNo ratings yet
- Human Drug List Dec 2011 V1 WebDocument1,260 pagesHuman Drug List Dec 2011 V1 WebMohamed El-sayedNo ratings yet
- Iron ToxicityDocument35 pagesIron ToxicityMohamed El-sayedNo ratings yet
- Blood Transfusion ReactionDocument38 pagesBlood Transfusion ReactionMohamed El-sayedNo ratings yet
- SdarticleDocument2 pagesSdarticleMohamed El-sayedNo ratings yet
- Acute UGI Bleeding: Stephen Matarazzo MDDocument20 pagesAcute UGI Bleeding: Stephen Matarazzo MDMohamed El-sayedNo ratings yet
- Short Bowel SyndromeDocument20 pagesShort Bowel SyndromeMohamed El-sayedNo ratings yet
- Bellezza-WetCast Paver 80mm PDFDocument2 pagesBellezza-WetCast Paver 80mm PDFkhaniskhan03No ratings yet
- Dewatering TechniquesDocument25 pagesDewatering Techniqueskrupa100% (1)
- Design Operation and Maintenance of CT PDFDocument24 pagesDesign Operation and Maintenance of CT PDFHamid Ariz50% (2)
- Vegan DogsDocument64 pagesVegan DogsOuerGentorix50% (2)
- Everything You Want To Know About RecrystallizationDocument3 pagesEverything You Want To Know About Recrystallizationrana_mohamed558100% (2)
- Ionic EquilibriumDocument2 pagesIonic Equilibriumpinnaacleclasses salemNo ratings yet
- Photo Degradation of PlasticsDocument19 pagesPhoto Degradation of PlasticsJHA UJJWAL RAKESHNo ratings yet
- Midazolam (RX) : Dosing & UsesDocument4 pagesMidazolam (RX) : Dosing & Usesintrovert ikonNo ratings yet
- Dryer Data Sheet Refrigerant Dryers Model DataDocument21 pagesDryer Data Sheet Refrigerant Dryers Model Dataroni kurniawanNo ratings yet
- Sr. No. Instrument Description Make Range L.C. ID. No. Location Reactor-101Document10 pagesSr. No. Instrument Description Make Range L.C. ID. No. Location Reactor-101SagarNo ratings yet
- Alkanes ClassDocument27 pagesAlkanes ClassRyan JamesNo ratings yet
- Side Pocket Mandrel NS 1 A4 1watermarked PDFDocument7 pagesSide Pocket Mandrel NS 1 A4 1watermarked PDFislam atifNo ratings yet
- Chinese Herbal Medicines: Pei-Ling Tang, Er-Wei Hao, Jia-Gang Deng, Xiao-Tao Hou, Zuo-Hui Zhang, Jin-Ling XieDocument6 pagesChinese Herbal Medicines: Pei-Ling Tang, Er-Wei Hao, Jia-Gang Deng, Xiao-Tao Hou, Zuo-Hui Zhang, Jin-Ling Xiemetha anandaNo ratings yet
- AAA - Beneficiation of Iron Ore by Flotation - Review of Industrial and Potential ApplicationsDocument22 pagesAAA - Beneficiation of Iron Ore by Flotation - Review of Industrial and Potential Applicationsmehra222No ratings yet
- Petronas Urania CF: High-Performance Single Grade Diesel Engine Oils Exceeding API Service CF Performance LevelsDocument1 pagePetronas Urania CF: High-Performance Single Grade Diesel Engine Oils Exceeding API Service CF Performance Levelsbarrysmith77No ratings yet
- Interface Solutions Gasket MaterialsDocument7 pagesInterface Solutions Gasket MaterialsBerkah PowerindoNo ratings yet
- Alcohol ProductionDocument85 pagesAlcohol Productiondebjani kundu100% (1)
- Practical Household Uses of Vinegar Margaret BriggsDocument111 pagesPractical Household Uses of Vinegar Margaret Briggsjorge_artola_6No ratings yet
- TheOldMadeNew PDFDocument66 pagesTheOldMadeNew PDFLuis A GuevaraNo ratings yet
- 5 - K. Horova, J. Tomsu, F. Wald - To Base Plates of Hollow Sections ColumnsDocument36 pages5 - K. Horova, J. Tomsu, F. Wald - To Base Plates of Hollow Sections ColumnsAnonymous bqV7MbFSuNo ratings yet
- Décembre 1995: Boutique AFNOR Pour: Solios Carbone Client 8319200 Commande N-20100112-383554-TA Le 12/1/2010 16:25Document15 pagesDécembre 1995: Boutique AFNOR Pour: Solios Carbone Client 8319200 Commande N-20100112-383554-TA Le 12/1/2010 16:25Mahesh Kumar BandariNo ratings yet
- Material Science and Engineering Ch. 10 SolDocument72 pagesMaterial Science and Engineering Ch. 10 SolPatrick GibsonNo ratings yet
- Lecture Notes PDFDocument134 pagesLecture Notes PDFShivam VermaNo ratings yet
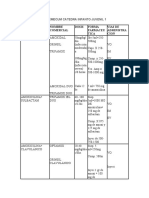
- Antibioticos Nombre Comercial Dosis Forma Farmaceu Tica Vias de Administra CionDocument10 pagesAntibioticos Nombre Comercial Dosis Forma Farmaceu Tica Vias de Administra CionLUCRECIA SUAREZ MORENONo ratings yet
- Mechanical Engineering-Machine Design MCQDocument22 pagesMechanical Engineering-Machine Design MCQBala MetturNo ratings yet
- Toaz - Info Chemtech Reviewer PRDocument1 pageToaz - Info Chemtech Reviewer PRchristy janioNo ratings yet
- Hot Work PermitDocument6 pagesHot Work PermitDasari VenkateshNo ratings yet
- Jps 21771Document11 pagesJps 21771Ana CicadaNo ratings yet
- (Total 1 Mark) : Hasmonean High School 1Document79 pages(Total 1 Mark) : Hasmonean High School 1dillanp15No ratings yet
- Tempra - Google SearchDocument1 pageTempra - Google Searchlys.hereNo ratings yet