Download as pptx, pdf, or txt
You might also like
- Parapac Plus Transport Ventilator: Pneupac Ventilation in MotionDocument2 pagesParapac Plus Transport Ventilator: Pneupac Ventilation in Motionamor kermaya100% (1)
- Critical Care Goals and ObjectivesDocument28 pagesCritical Care Goals and ObjectivesjyothiNo ratings yet
- Early Physical and Occupational Therapy in Mechanically Ventilated, Critically Ill Patients A Randomised Controlled Trial - Barker2010Document2 pagesEarly Physical and Occupational Therapy in Mechanically Ventilated, Critically Ill Patients A Randomised Controlled Trial - Barker2010RodrigoSachiFreitasNo ratings yet
- 6.025 Control of Remote Area Travel and Search and Rescue ProceduresDocument16 pages6.025 Control of Remote Area Travel and Search and Rescue ProceduresAhmed TrabelsiNo ratings yet
- Cardiology PolyclinicDocument22 pagesCardiology PolyclinicJoão CakeNo ratings yet
- Trial of Continuous or Interrupted Chest Compressions During CPRDocument12 pagesTrial of Continuous or Interrupted Chest Compressions During CPRDinar Riny NvNo ratings yet
- Emergency Physician-Initiated Resuscitative Extracorporeal Membrane OxygenationDocument13 pagesEmergency Physician-Initiated Resuscitative Extracorporeal Membrane Oxygenationshiffa ramadhantiNo ratings yet
- EC EBM Presentation Template-ExpandedDocument28 pagesEC EBM Presentation Template-ExpandedErgon ÇoçajNo ratings yet
- Extubation With or Without Spontaneous Breathing TrialDocument9 pagesExtubation With or Without Spontaneous Breathing TrialPAULA SORAIA CHENNo ratings yet
- Extubation Success Prediction in A Multicentric Cohort of Patients With Severe Brain InjuryDocument9 pagesExtubation Success Prediction in A Multicentric Cohort of Patients With Severe Brain InjuryEdison LucioNo ratings yet
- CPR EthicsDocument51 pagesCPR EthicsDoha EbedNo ratings yet
- E Cacy of Early Respiratory Physiotherapy and Mobilization After On-Pump Cardiac Surgery: A Prospective Randomized Controlled TrialDocument15 pagesE Cacy of Early Respiratory Physiotherapy and Mobilization After On-Pump Cardiac Surgery: A Prospective Randomized Controlled TrialAsmaa GamalNo ratings yet
- Jurnal Flail Chest.Document6 pagesJurnal Flail Chest.Dessy Christiani Part IINo ratings yet
- Orthopedic Principles To Facilitate Enhanced RecovDocument14 pagesOrthopedic Principles To Facilitate Enhanced RecovBader ZawahrehNo ratings yet
- Research Cardiac SurgeryDocument7 pagesResearch Cardiac SurgeryImran KalyarNo ratings yet
- Chest Physiotherapy in Mechanically Ventilated Children A ReviewDocument10 pagesChest Physiotherapy in Mechanically Ventilated Children A Reviewmrizki_1No ratings yet
- PreOperative & PremedicationDocument9 pagesPreOperative & PremedicationMastering Archangel SchneiderNo ratings yet
- 2015 Article 159Document8 pages2015 Article 159andri anaNo ratings yet
- Skoretz 2014Document8 pagesSkoretz 2014Gonzalo FragaNo ratings yet
- Factsheet CTODocument2 pagesFactsheet CTObayusetia150278No ratings yet
- Noninvasive Ventilation For Prevention of Post-Extubation Respiratory Failure in Obese PatientsDocument8 pagesNoninvasive Ventilation For Prevention of Post-Extubation Respiratory Failure in Obese PatientsLestat80No ratings yet
- Deep Breath & SpirometerDocument7 pagesDeep Breath & SpirometerAsmaa GamalNo ratings yet
- Meroni2017 CompressedDocument8 pagesMeroni2017 Compresseddayllyn iglesiasNo ratings yet
- Ventilatorweaningand Extubation: Karen E.A. Burns,, Bram Rochwerg, Andrew J.E. SeelyDocument18 pagesVentilatorweaningand Extubation: Karen E.A. Burns,, Bram Rochwerg, Andrew J.E. Seelyأركان هيلث Arkan healthNo ratings yet
- Noninvasive VentilationDocument6 pagesNoninvasive VentilationEma MagfirahNo ratings yet
- DR Lila - Patient Preparation For Emergencies Surgeries - New 11012017Document37 pagesDR Lila - Patient Preparation For Emergencies Surgeries - New 11012017bloadyroar100% (1)
- JournalDocument37 pagesJournalLeahNo ratings yet
- Critical Care Medicine: Background: Methods: ResultsDocument9 pagesCritical Care Medicine: Background: Methods: ResultsMedicina InternaNo ratings yet
- The Effectiveness of Early Position Change Postcardiac Catheterization On Patient's Outcomes A Randomized Controlled TrialDocument9 pagesThe Effectiveness of Early Position Change Postcardiac Catheterization On Patient's Outcomes A Randomized Controlled TrialAdelia putriNo ratings yet
- 10 1016@j Jemermed 2019 12 004Document10 pages10 1016@j Jemermed 2019 12 004Fraternity LiviNo ratings yet
- 348-Article Text-1233-1-10-20201221Document5 pages348-Article Text-1233-1-10-20201221Salsabila FitriaNo ratings yet
- Journal Cardiac ArrestDocument6 pagesJournal Cardiac ArrestDavid Fransiskus SimarmataNo ratings yet
- CCM 45 10 2017 05 25 Zhang Ccmed-D-16-00678 sdc2Document6 pagesCCM 45 10 2017 05 25 Zhang Ccmed-D-16-00678 sdc2denisNo ratings yet
- Preoperative Assessment, Premedication, & Perioperative DocumentationDocument16 pagesPreoperative Assessment, Premedication, & Perioperative DocumentationWenny Eka FildayantiNo ratings yet
- Journal of Trauma Management & OutcomesDocument7 pagesJournal of Trauma Management & OutcomesCahyaning WijayantiNo ratings yet
- Randomized Trial of Stents Versus Bypass Surgery For Left Main Coronary Artery DiseaseDocument9 pagesRandomized Trial of Stents Versus Bypass Surgery For Left Main Coronary Artery DiseaseTommy WidjayaNo ratings yet
- Journal Club April 2023 v2Document32 pagesJournal Club April 2023 v2Gail DrescherNo ratings yet
- Journal AppraisalDocument37 pagesJournal AppraisalLeahNo ratings yet
- 2014 Journal - Patient With Congenital Systemic To Pulmonary Shunts and Increased Pulmonary Vascular ResistanceDocument7 pages2014 Journal - Patient With Congenital Systemic To Pulmonary Shunts and Increased Pulmonary Vascular ResistanceAryfKurniawanNo ratings yet
- Lampiran Jurnal 1 PDFDocument7 pagesLampiran Jurnal 1 PDFCyon Siiee D'javuNo ratings yet
- Wu 2017Document7 pagesWu 2017petrus daveNo ratings yet
- 2- High-Velocity Nasal Insufflation in the Treatment of Respiratory FailureDocument31 pages2- High-Velocity Nasal Insufflation in the Treatment of Respiratory FailureabbhamzaaaaNo ratings yet
- تDocument9 pagesتBaleegh A. QahtanNo ratings yet
- Renu VHDDocument91 pagesRenu VHDRenu KhedekarNo ratings yet
- Journal Appraisal: Aiza Gabrinez Drmc-General Surgery JUNE 25, 2020Document34 pagesJournal Appraisal: Aiza Gabrinez Drmc-General Surgery JUNE 25, 2020Tonie AbabonNo ratings yet
- s12872 019 1096 1Document9 pagess12872 019 1096 1sarahNo ratings yet
- Effect of A Pediatric Early Warning System On All-Cause Mortality in Hospitalized Pediatric PatientsDocument35 pagesEffect of A Pediatric Early Warning System On All-Cause Mortality in Hospitalized Pediatric PatientsabdfaqihNo ratings yet
- Gastric Versus Postpyloric Enteral Nutrition in Elderly Patients (Age 75 Years) On Mechanical Ventilation: A Single-Center Randomized TrialDocument11 pagesGastric Versus Postpyloric Enteral Nutrition in Elderly Patients (Age 75 Years) On Mechanical Ventilation: A Single-Center Randomized TrialDyana NurNo ratings yet
- Rapid Rehabilitation Nursing in Postoperative Patients With Colorectal Cancer and Quality of LifeDocument8 pagesRapid Rehabilitation Nursing in Postoperative Patients With Colorectal Cancer and Quality of Lifejamie carpioNo ratings yet
- Yataco2019.Early Progressive Mobilization of Patients With EVD. Safety An FeasibilityDocument7 pagesYataco2019.Early Progressive Mobilization of Patients With EVD. Safety An FeasibilityEviNo ratings yet
- Cardiogenic Shock: Updated Approach To ManagementDocument49 pagesCardiogenic Shock: Updated Approach To ManagementelsarahmiNo ratings yet
- Mithun Journal-1 4Document27 pagesMithun Journal-1 4Tanuja LNo ratings yet
- Evolution of Outcomes in Cardiothoracic SurgeryDocument8 pagesEvolution of Outcomes in Cardiothoracic Surgeryannisa statiraNo ratings yet
- Journacl Club Med 4Document29 pagesJournacl Club Med 4saveetha purushothamanNo ratings yet
- Journal Club April 2023 v2Document32 pagesJournal Club April 2023 v2Gail DrescherNo ratings yet
- Critical (17-24)Document15 pagesCritical (17-24)kololll lllknNo ratings yet
- Graft Patency After Off-Pump Versus On-Pump Coronary Artery Surgery in High-Risk PatientsDocument8 pagesGraft Patency After Off-Pump Versus On-Pump Coronary Artery Surgery in High-Risk PatientsZul FikarNo ratings yet
- ICC2 (008) Perioperative Care WorkbookDocument99 pagesICC2 (008) Perioperative Care WorkbookMariam Mokhtar ZedanNo ratings yet
- Vaishali Syal Moderator - Prof. J. R. ThakurDocument34 pagesVaishali Syal Moderator - Prof. J. R. ThakurTasha NurfitrianiNo ratings yet
- Jurnal TracheostomyDocument17 pagesJurnal TracheostomyLora Angraeni PatodingNo ratings yet
- Early Intensive Care Unit Mobility Therapy in The Treatment of Acute Respiratory FailureDocument6 pagesEarly Intensive Care Unit Mobility Therapy in The Treatment of Acute Respiratory FailureTakashi NakamuraNo ratings yet
- 2022 Preoperative Assessment Premedication Perioperative DocumentationDocument38 pages2022 Preoperative Assessment Premedication Perioperative DocumentationMohmmed Mousa100% (1)
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
- Trilogy Evo Quick Start GuideDocument24 pagesTrilogy Evo Quick Start GuideAngeloNo ratings yet
- Transkrip Tugas Percakapan Bahasa InggrisDocument3 pagesTranskrip Tugas Percakapan Bahasa InggrisZhincan 07No ratings yet
- Handling Complaint and To Be Warming Person For Everybody: Dr. Dr. Andry, MM, MhkesDocument28 pagesHandling Complaint and To Be Warming Person For Everybody: Dr. Dr. Andry, MM, MhkesBidang Pelayanan RSUD SekarwangiNo ratings yet
- Resumen Unidad 2Document31 pagesResumen Unidad 2yeseniaram073No ratings yet
- Medical BillDocument1 pageMedical BillAkshay ShendreNo ratings yet
- Tong Hop de Thi That Ielts Reading 2023 - Bee IeltsDocument36 pagesTong Hop de Thi That Ielts Reading 2023 - Bee Ielts23006546100% (1)
- Gland Pharma Thread - Vishnu KapadiaDocument6 pagesGland Pharma Thread - Vishnu KapadiatempofaltuNo ratings yet
- Dsem TRM 0514 0052 1 - LRDocument68 pagesDsem TRM 0514 0052 1 - LRAbhishek JirelNo ratings yet
- Laporan Mutasi Inventory GlobalDocument61 pagesLaporan Mutasi Inventory GlobalEustas D PickNo ratings yet
- Guidelines To The Diagnostic Centre For Lic Pre-Insurance Medical CheckupDocument3 pagesGuidelines To The Diagnostic Centre For Lic Pre-Insurance Medical CheckupAmita SaigalNo ratings yet
- MyobraceFlowchart 0320 ENG v1.0.4Document1 pageMyobraceFlowchart 0320 ENG v1.0.4rinahpsNo ratings yet
- Public Information Officers Contact ListDocument3 pagesPublic Information Officers Contact ListAman KhanNo ratings yet
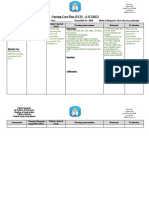
- Nursing Care Plan (NCP) 6 SCORES: Patient-Centered (In Priority Order)Document2 pagesNursing Care Plan (NCP) 6 SCORES: Patient-Centered (In Priority Order)WorodNo ratings yet
- Manual de Uso Videocolonoscopio Ec-530wlDocument60 pagesManual de Uso Videocolonoscopio Ec-530wlEddy Fernando Ruiz AvilaNo ratings yet
- SSC 59 Removal of & Protection From Negative Emotions CombinationDocument1 pageSSC 59 Removal of & Protection From Negative Emotions CombinationhimaNo ratings yet
- WEBMEDQUEST Brochure PDFDocument29 pagesWEBMEDQUEST Brochure PDFKartkkNo ratings yet
- Césarienne RPC Oct 2022 CngofDocument375 pagesCésarienne RPC Oct 2022 CngofTchimon VodouheNo ratings yet
- Menu Dak Reguler & Dak Penugasan 2021: 1. Alkes Ruang IccuDocument21 pagesMenu Dak Reguler & Dak Penugasan 2021: 1. Alkes Ruang IccuNoor IstichawariNo ratings yet
- Formulation and Pharmacological Evaluation of Acalypha Fruticosa Ethosomal Gel For Wound Healing ActivityDocument35 pagesFormulation and Pharmacological Evaluation of Acalypha Fruticosa Ethosomal Gel For Wound Healing ActivitydaniyaNo ratings yet
- FIRST AID EDUCATION Part 1 and 2 - EntrepreneurshipDocument17 pagesFIRST AID EDUCATION Part 1 and 2 - EntrepreneurshipMary Ann VALLECERNo ratings yet
- Drug Resistance TB Mono Drug Resistant TBDocument2 pagesDrug Resistance TB Mono Drug Resistant TBMalavath PavithranNo ratings yet
- Full Download Solution Manual For Human Anatomy Physiology Main Version 4th Edition Terry Martin Cynthia Prentice Crave PDF Full ChapterDocument35 pagesFull Download Solution Manual For Human Anatomy Physiology Main Version 4th Edition Terry Martin Cynthia Prentice Crave PDF Full Chaptergabertconsomme.gygy100% (25)
- Introduction To Research in Ayurveda: DR Sudhikumar K B Professor KUHS-School of Fundamental Research in AyurvedaDocument57 pagesIntroduction To Research in Ayurveda: DR Sudhikumar K B Professor KUHS-School of Fundamental Research in AyurvedamadhubalaNo ratings yet
- PRUValue Med PRUMillion Med Booster Leaflet - ENGDocument14 pagesPRUValue Med PRUMillion Med Booster Leaflet - ENGMuadz AmirazamNo ratings yet
- So Obat Apbd April 2022Document42 pagesSo Obat Apbd April 2022suprihartiwiNo ratings yet
- Thai PF 31.3.23Document11 pagesThai PF 31.3.23gaurav sharmaNo ratings yet
- Assessment of The Ear and Hearing AcuityDocument3 pagesAssessment of The Ear and Hearing AcuityJay Debby RuizoNo ratings yet