Download as pptx, pdf, or txt
You might also like
- FULL Download Ebook PDF Huszars Ecg and 12 Lead Interpretation 5th Edition PDF EbookDocument41 pagesFULL Download Ebook PDF Huszars Ecg and 12 Lead Interpretation 5th Edition PDF Ebookcody.cherry20098% (43)
- Ventricular Septal Defects: Drmlpatel Department of Medicine KgmuDocument19 pagesVentricular Septal Defects: Drmlpatel Department of Medicine KgmuDurgesh PushkarNo ratings yet
- VSDDocument29 pagesVSDVaibhav Krishna100% (2)
- Abnormal Heart Development 4-10-14 For BBDocument21 pagesAbnormal Heart Development 4-10-14 For BBroman7dbNo ratings yet
- A Ventricular Septal Defect (VSD) Is A Hole or A Defect inDocument24 pagesA Ventricular Septal Defect (VSD) Is A Hole or A Defect inTejinder SinghNo ratings yet
- CHD - Med IIDocument70 pagesCHD - Med IISanskruthi KurniNo ratings yet
- Cardio-Respiratory Conditions: by DR Priscus MushiDocument73 pagesCardio-Respiratory Conditions: by DR Priscus MushiMusaNo ratings yet
- Patent Ductus Arteriosus - Most Common Congenital Heart Defect Symptoms DependDocument5 pagesPatent Ductus Arteriosus - Most Common Congenital Heart Defect Symptoms DependANNENo ratings yet
- Ventricular Septal DefectDocument55 pagesVentricular Septal DefecthoneyworksNo ratings yet
- Congenital Heart DiseaseDocument57 pagesCongenital Heart DiseaseAparna RawatNo ratings yet
- University of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingDocument69 pagesUniversity of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingErica Veluz LuyunNo ratings yet
- Congenital Disorder ASD VSDDocument50 pagesCongenital Disorder ASD VSDSachin DwivediNo ratings yet
- Congenital Heart DiseaseDocument60 pagesCongenital Heart DiseaseBonfaceNo ratings yet
- Acynotic DiseaseDocument55 pagesAcynotic DiseaseTesfamichael AbathunNo ratings yet
- PDA Case StudyDocument5 pagesPDA Case StudyDiana Andrea AyongaoNo ratings yet
- Acyanotic CHD 2008Document50 pagesAcyanotic CHD 2008Ana Abadi Al IndNo ratings yet
- CardiologyDocument43 pagesCardiologyhasanatiya41No ratings yet
- 10 Cardiology LectureDocument64 pages10 Cardiology Lectureaemy13266No ratings yet
- VALVULAR HEART DISEASE Copy AutosavedDocument33 pagesVALVULAR HEART DISEASE Copy AutosavedShienna Rose Ann ManaloNo ratings yet
- 01 Cardiovascular IDocument72 pages01 Cardiovascular IcoriezaNo ratings yet
- Congenital Heart Defect-VsdDocument53 pagesCongenital Heart Defect-VsdAuni Akif AleesaNo ratings yet
- Approach To Diagnosis of Congenital Heart DiseasesDocument85 pagesApproach To Diagnosis of Congenital Heart DiseasesNirav CHOVATIYANo ratings yet
- DR - Azad A Haleem AL - Brefkani: University of Duhok Faculty of Medical Science School of Medicine Pediatrics DepartmentDocument58 pagesDR - Azad A Haleem AL - Brefkani: University of Duhok Faculty of Medical Science School of Medicine Pediatrics DepartmentGomathi ShankarNo ratings yet
- Week 6 Disturbances in CirculationDocument83 pagesWeek 6 Disturbances in CirculationHans CortezNo ratings yet
- Cardiac Diseases in ChildrenDocument66 pagesCardiac Diseases in ChildrenHarmas Novryan FarezaNo ratings yet
- Pathophysiology Congenital Heart Disease-1Document54 pagesPathophysiology Congenital Heart Disease-1single_ladyNo ratings yet
- 1 - VSD (Part 2) - Hatem HosnyDocument28 pages1 - VSD (Part 2) - Hatem Hosnyrami ibrahiemNo ratings yet
- Penyakit Jantung KongenitalDocument30 pagesPenyakit Jantung KongenitalrintiikNo ratings yet
- Congenital Cardiovascular Anomalies: Dr. Herlina Dimiati, Spa (K)Document36 pagesCongenital Cardiovascular Anomalies: Dr. Herlina Dimiati, Spa (K)EndiRasadiHermanNo ratings yet
- Paeds CardioDocument28 pagesPaeds CardioIman ZalzilahNo ratings yet
- Valvular & Inflammatory HDDocument33 pagesValvular & Inflammatory HDSinam SinghaNo ratings yet
- ucu-CHDs 240114 230618Document68 pagesucu-CHDs 240114 230618BrianNo ratings yet
- Non-Cyanotic Congenital Heart Disease-UpDate 4-22-53Document136 pagesNon-Cyanotic Congenital Heart Disease-UpDate 4-22-53getnusNo ratings yet
- Cardiovascular Diseases VSD Asd 2022 1Document16 pagesCardiovascular Diseases VSD Asd 2022 1Boyu GrtrNo ratings yet
- Venous Thromboembolism (VTE) Pathophysiology September 2016Document46 pagesVenous Thromboembolism (VTE) Pathophysiology September 2016Nick GouvatsosNo ratings yet
- PAEDs - CVS-1Document44 pagesPAEDs - CVS-1Priscah bhokeNo ratings yet
- Congenital Heart DiseasesDocument27 pagesCongenital Heart DiseasesJumar ValdezNo ratings yet
- Congenital Heart DiseasesDocument121 pagesCongenital Heart DiseasesJayvee V. De GuzmanNo ratings yet
- Congenital Heart DiseaseDocument51 pagesCongenital Heart Diseaseelsa prima putri100% (2)
- Congenital Heart DefectsDocument73 pagesCongenital Heart DefectsStaen KisNo ratings yet
- Ventricular Septal DefectDocument2 pagesVentricular Septal DefectAra AugustoNo ratings yet
- Inflammatory and Valvular DisordersDocument43 pagesInflammatory and Valvular DisordersRifqi Hary ZulfikarNo ratings yet
- Cardiac & Respiratory Diseases in PregnancyDocument30 pagesCardiac & Respiratory Diseases in PregnancyKerod AbebeNo ratings yet
- CHD ApproachDocument140 pagesCHD ApproachauNo ratings yet
- Superior Vena Cava SyndromeDocument57 pagesSuperior Vena Cava SyndromeKhadira MohammedNo ratings yet
- cvs2 CHDDocument27 pagescvs2 CHDIda WilonaNo ratings yet
- Cardiac Disease in Pregnancy1-1Document26 pagesCardiac Disease in Pregnancy1-1Homeground entertainmentNo ratings yet
- Case Presentation: Congenital Heart DiseaseDocument37 pagesCase Presentation: Congenital Heart DiseaseKarin Nadia UtamiNo ratings yet
- Curs Bolile PericarduluiDocument85 pagesCurs Bolile PericarduluiAndreea ElenaNo ratings yet
- Pericardial DX Endocarditis MyocarditisDocument74 pagesPericardial DX Endocarditis MyocarditisJefry SNo ratings yet
- Lapkas ANAKDocument40 pagesLapkas ANAKThemySutejaNo ratings yet
- ASD and VSDDocument18 pagesASD and VSDnoekkuNo ratings yet
- Cardiac Disease in Pregnancy1Document23 pagesCardiac Disease in Pregnancy1Homeground entertainmentNo ratings yet
- 7 PENYAKIT JANTUNG BAWAAN DR - YusraDocument57 pages7 PENYAKIT JANTUNG BAWAAN DR - YusraSurya ArhNo ratings yet
- VSDDocument38 pagesVSDEva MegaNo ratings yet
- ISCHEMIC HEART DISEASE: Stable AnginaDocument51 pagesISCHEMIC HEART DISEASE: Stable AnginaОльга КоваленкоNo ratings yet
- Penyakit Jantung Bawaan II - 2Document30 pagesPenyakit Jantung Bawaan II - 2ahmad syauqieNo ratings yet
- Superior Vena Cava Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSuperior Vena Cava Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Essential Facts in Cardiovascular Medicine: Board Review and Clinical PearlsFrom EverandEssential Facts in Cardiovascular Medicine: Board Review and Clinical PearlsNo ratings yet
- Program Book of INAechoDocument15 pagesProgram Book of INAechoAnthomina MayaNo ratings yet
- Atrial Septal Defect With Pulmonary Hypertension: When/how Can We Consider Closure?Document9 pagesAtrial Septal Defect With Pulmonary Hypertension: When/how Can We Consider Closure?Faradiba MaricarNo ratings yet
- Session 10Document2 pagesSession 10Sistine Rose Labajo100% (1)
- Shazia Kazi ResumeDocument2 pagesShazia Kazi Resumeshazia kaziNo ratings yet
- DC - M. Youssry Final WhiteDocument21 pagesDC - M. Youssry Final Whitemarwa abdelmegedNo ratings yet
- Practical Cardiac AuscultationDocument15 pagesPractical Cardiac AuscultationAugusto Rojas CarrionNo ratings yet
- Lakunar and Outcome StrokeDocument11 pagesLakunar and Outcome StrokesitialimahNo ratings yet
- Golden Ratio Is Beating in Our HeartDocument2 pagesGolden Ratio Is Beating in Our HeartDeepak Kumar Singh Res. Scholar., Dept. of Mechanical Engg., IIT (BHU)No ratings yet
- ElectrocardiogramDocument169 pagesElectrocardiogramjitendra magarNo ratings yet
- Eco DopplerDocument8 pagesEco DopplerClaudia IsabelNo ratings yet
- Regurgitación TricúspideDocument16 pagesRegurgitación TricúspideMissa BernalNo ratings yet
- Abbreviation Meaning: AbdominalDocument3 pagesAbbreviation Meaning: AbdominalMariel GentilesNo ratings yet
- Fundamentals of ECGDocument112 pagesFundamentals of ECGadithya polavarapu100% (1)
- How To Recognize Congenital Heart Disease in Pediatric: Benny TM TogatoropDocument173 pagesHow To Recognize Congenital Heart Disease in Pediatric: Benny TM TogatoropRidyahningtyas SintowatiNo ratings yet
- Ecg ReadingDocument2 pagesEcg Readingtheodore_estradaNo ratings yet
- Ischaemic Heart DiseaseDocument23 pagesIschaemic Heart Diseasebrain bareNo ratings yet
- Prognosis of Patients With Complete Heart BlockDocument7 pagesPrognosis of Patients With Complete Heart BlockRaul OrtegaNo ratings yet
- Principles of ECGDocument11 pagesPrinciples of ECGDeinielle Magdangal RomeroNo ratings yet
- Practical Nursing Diploma Program Nursing Skills Lab 1: Blood Pressure Week 12Document21 pagesPractical Nursing Diploma Program Nursing Skills Lab 1: Blood Pressure Week 12Taryn CorbettNo ratings yet
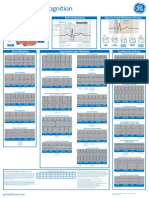
- Arrhythmia Recognition Part 1 and 2 DOC1178264 Rev2Document2 pagesArrhythmia Recognition Part 1 and 2 DOC1178264 Rev2Nico Angelo CopoNo ratings yet
- Dressler Sindrom in Patinet With Large Anterolateral STEMIDocument1 pageDressler Sindrom in Patinet With Large Anterolateral STEMIdrstojanmitreskiNo ratings yet
- 2 - PPT DR Erika Maharani SPJPDocument42 pages2 - PPT DR Erika Maharani SPJPAmry YusufNo ratings yet
- Dysrhythmia TestsDocument3 pagesDysrhythmia TestsKimberly WhitesideNo ratings yet
- Blood VesselsDocument4 pagesBlood VesselsCrazy StrangerNo ratings yet
- Normal Ecg, Infarction & Arrhythmia SDocument98 pagesNormal Ecg, Infarction & Arrhythmia SAdinda GupitaNo ratings yet
- Long-Term Outcome in Congenitally Corrected Transposition of The Great ArteriesDocument7 pagesLong-Term Outcome in Congenitally Corrected Transposition of The Great Arteriespaul00040No ratings yet
- Narasimha Pai Issue 27 Mamatha RathnaDocument7 pagesNarasimha Pai Issue 27 Mamatha RathnadrpklalNo ratings yet
- History Taking and PF CVD Iman Evan Final Fix - Dr. M Yusak SPJPDocument84 pagesHistory Taking and PF CVD Iman Evan Final Fix - Dr. M Yusak SPJPFikriYTNo ratings yet
- Toprank Cardio Hema Post TestDocument5 pagesToprank Cardio Hema Post TestJoyce ObraNo ratings yet