Download as pptx, pdf, or txt
You might also like
- Managing Bipolar DisorderDocument129 pagesManaging Bipolar DisorderLaura Bechtolsheimer100% (11)
- Postpartum DepressionDocument28 pagesPostpartum DepressionRiza Angela Barazan100% (1)
- Examen Ortopedico InfantilDocument21 pagesExamen Ortopedico InfantilSebastian CamiloNo ratings yet
- Psychological Complications, Post Partum Blues, Depression, PsychosisDocument42 pagesPsychological Complications, Post Partum Blues, Depression, Psychosisbasamma kumbarNo ratings yet
- Postnatal Depression Shakespeare BMJ - 2014Document3 pagesPostnatal Depression Shakespeare BMJ - 2014Tebah AlatwanNo ratings yet
- Research Paper On Postpartum DepressionDocument8 pagesResearch Paper On Postpartum Depressiongw2x60nw100% (1)
- Postpartum Depression Literature ReviewDocument4 pagesPostpartum Depression Literature Reviewapi-549828920No ratings yet
- Tropical Medicine System: Course Study GuideDocument16 pagesTropical Medicine System: Course Study GuideJohn P M SinagaNo ratings yet
- Individual Mental Health AssignmentDocument18 pagesIndividual Mental Health AssignmentRebekah Roberts100% (1)
- Postpartum Depression Essay ThesisDocument9 pagesPostpartum Depression Essay Thesisafcmfuind100% (2)
- Inggris JurnalDocument5 pagesInggris JurnalMeisya MonicaNo ratings yet
- Postpartum Depression: Clinical PracticeDocument11 pagesPostpartum Depression: Clinical PracticeCasey Daisiu100% (1)
- Postnatal Depression Dissertation IdeasDocument5 pagesPostnatal Depression Dissertation IdeasWhoWillWriteMyPaperForMeCanada100% (1)
- Day 4 - Common Session 1 - Ped PC - DR Maryann MuckadenDocument82 pagesDay 4 - Common Session 1 - Ped PC - DR Maryann Muckadenm debNo ratings yet
- Midwifery Dissertation Postnatal DepressionDocument8 pagesMidwifery Dissertation Postnatal DepressionCollegePaperHelpCanada100% (1)
- Endometriosis Case Study AroojDocument36 pagesEndometriosis Case Study AroojAli AkbarNo ratings yet
- Dissertation Bipolar DisorderDocument4 pagesDissertation Bipolar DisorderWhereCanIFindSomeoneToWriteMyPaperSingapore100% (1)
- Duchenne MD EHusbandsDocument33 pagesDuchenne MD EHusbandsfirst name last nameNo ratings yet
- 3a 2 - NCM 117 Rle Schizophrenia Case PresentationDocument97 pages3a 2 - NCM 117 Rle Schizophrenia Case PresentationArianne Rose Afable PagulayanNo ratings yet
- Depression Research Paper PDFDocument8 pagesDepression Research Paper PDFgz9g97ha100% (1)
- Caregiver Stress Research PaperDocument5 pagesCaregiver Stress Research Paperegxtc6y3100% (1)
- Saludamay Nursing JournalDocument76 pagesSaludamay Nursing JournalcrisjavaNo ratings yet
- ABC of Palliative Care: Special Problems of Children: Clinical ReviewDocument12 pagesABC of Palliative Care: Special Problems of Children: Clinical ReviewvabcunhaNo ratings yet
- Wa0001.Document74 pagesWa0001.relaxtube2506No ratings yet
- Goiter CPDocument86 pagesGoiter CPTianna Jane StephensonNo ratings yet
- Cochise Tail Oa Group ProjectDocument13 pagesCochise Tail Oa Group Projectapi-644444841No ratings yet
- New Born ScreeningDocument22 pagesNew Born ScreeninglendiibanezNo ratings yet
- Literature Review On Postpartum DepressionDocument5 pagesLiterature Review On Postpartum Depressionea6bmkmc100% (1)
- Prevalence of Postpartum Depression Among Mothers Who DeliveredDocument14 pagesPrevalence of Postpartum Depression Among Mothers Who DeliveredwhatsnotclickingbabehNo ratings yet
- Prevalence of Postpartum Depression Among Mothers Who DeliveredDocument7 pagesPrevalence of Postpartum Depression Among Mothers Who Deliveredroven desuNo ratings yet
- Postnatal DepressionDocument17 pagesPostnatal Depressionmaria100% (1)
- Depression During Pregnancy Final Amah and WalaDocument21 pagesDepression During Pregnancy Final Amah and WalaAmna Sidi MohammadNo ratings yet
- CaseDocument16 pagesCaseJesil MarolinaNo ratings yet
- Postnatal DepressionDocument6 pagesPostnatal DepressionWasemBhatNo ratings yet
- Postpartum Depression DissertationDocument7 pagesPostpartum Depression DissertationPaperWritingServiceCheapAnnArbor100% (1)
- Clinical Pearls in Perinatal Mental HealthDocument10 pagesClinical Pearls in Perinatal Mental HealthJona JoyNo ratings yet
- Case 2 Depression 3F G4Document51 pagesCase 2 Depression 3F G4Eduard MontanoNo ratings yet
- Oa GRP Project Template W Instructions1 1Document11 pagesOa GRP Project Template W Instructions1 1api-643384875No ratings yet
- SchizophreniaDocument91 pagesSchizophreniaJanielle Christine Monsalud100% (1)
- Abm Clinical Protocol 18 PDFDocument10 pagesAbm Clinical Protocol 18 PDFMarianaNo ratings yet
- University of BahrainDocument7 pagesUniversity of Bahrainزهرة الدوارNo ratings yet
- Term Paper On Postpartum DepressionDocument8 pagesTerm Paper On Postpartum Depressionc5mr3mxf100% (1)
- 2-Premarital Counseling & Menstrual DisordeDocument69 pages2-Premarital Counseling & Menstrual Disordematter.nesma.nmNo ratings yet
- Rose-Morris Final EvalDocument13 pagesRose-Morris Final Evalapi-242018884No ratings yet
- E Table of Contents. Postpartum Psychosis: The Role of Women's Health Care Providers and The Health Care SystemDocument15 pagesE Table of Contents. Postpartum Psychosis: The Role of Women's Health Care Providers and The Health Care System4mdw25zqghNo ratings yet
- Psych NotesDocument57 pagesPsych NotesTheGreat100% (1)
- Women and Birth: Joanne Marnes, Pauline HallDocument5 pagesWomen and Birth: Joanne Marnes, Pauline Halljo_marnes100% (1)
- Draft 3-30-2024 Ob Case StudyDocument54 pagesDraft 3-30-2024 Ob Case StudyKent Jerimhe Daileg ManiaulNo ratings yet
- Thesis For Depression PaperDocument5 pagesThesis For Depression Paperjenniferriveraerie100% (2)
- Cognitive-Behavioral Therapy To Miscarriage - Results From The Use of A Grief TherapyDocument3 pagesCognitive-Behavioral Therapy To Miscarriage - Results From The Use of A Grief TherapyWaneska LimaNo ratings yet
- The Overdiagnosis of Depression in Non-Depressed Patients in Primary CareDocument7 pagesThe Overdiagnosis of Depression in Non-Depressed Patients in Primary Careengr.alinaqvi40No ratings yet
- Screening Tools For PostpartumDocument9 pagesScreening Tools For PostpartumNeni RochmayatiNo ratings yet
- General Hospital Psychiatry: Psychiatry and Primary CareDocument5 pagesGeneral Hospital Psychiatry: Psychiatry and Primary CareAndra NicoleNo ratings yet
- Bipolar Disorder TreatmentDocument16 pagesBipolar Disorder Treatmentaarushi sabharwalNo ratings yet
- Breaking Bad NewsDocument26 pagesBreaking Bad News8625g8xmbpNo ratings yet
- Scenario One Diabetes (Sweet A 2018-1Document5 pagesScenario One Diabetes (Sweet A 2018-1Regina PunNo ratings yet
- Food and Your Mood: A Guide to Improving Your Depression with Diet and Lifestyle ChangesFrom EverandFood and Your Mood: A Guide to Improving Your Depression with Diet and Lifestyle ChangesNo ratings yet
- Critical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeFrom EverandCritical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeNo ratings yet
- Bipolar: Practical Advice and Lived Experience (The Most Effective Strategies for a Great Sense of Structure Overall Mood Enhancement)From EverandBipolar: Practical Advice and Lived Experience (The Most Effective Strategies for a Great Sense of Structure Overall Mood Enhancement)No ratings yet
- Your Child's First Consultation Questions You Should Ask Your 31st Psychiatric Consultation William R. Yee M.D., J.D., Copyright Applied for May 22, 2022From EverandYour Child's First Consultation Questions You Should Ask Your 31st Psychiatric Consultation William R. Yee M.D., J.D., Copyright Applied for May 22, 2022No ratings yet
- Travis Oakes Fatality Inquiry ReportDocument10 pagesTravis Oakes Fatality Inquiry ReportcalcitydeskNo ratings yet
- With and Without GaltonDocument696 pagesWith and Without GaltonclaitonfloydNo ratings yet
- Acc21 March18Document12 pagesAcc21 March18Romero Mary Jane C.No ratings yet
- Iqwq-Ft-Rspds-00-120103 - 1 Preservation During Shipping and ConstructionDocument31 pagesIqwq-Ft-Rspds-00-120103 - 1 Preservation During Shipping and Constructionjacksonbello34No ratings yet
- Islam A Case of Mistaken Identity.Document29 pagesIslam A Case of Mistaken Identity.AndrewNo ratings yet
- The Enneagram GuideDocument26 pagesThe Enneagram GuideMoon5627No ratings yet
- STUDENT 2021-2022 Academic Calendar (FINAL)Document1 pageSTUDENT 2021-2022 Academic Calendar (FINAL)Babar ImtiazNo ratings yet
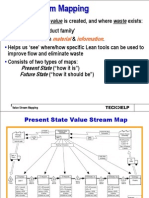
- 4 Slides Value Stream MappingDocument13 pages4 Slides Value Stream MappingRanjan Raj Urs100% (2)
- 03 Tiongson Cayetano Et Al Vs Court of Appeals Et AlDocument6 pages03 Tiongson Cayetano Et Al Vs Court of Appeals Et Alrandelrocks2No ratings yet
- Assignment of MGT 2133 (Section: 08) : Date of Submission: 24 August 2017Document17 pagesAssignment of MGT 2133 (Section: 08) : Date of Submission: 24 August 2017Mahzabeen NahidNo ratings yet
- VERNACULAR ARCHITECTURE (Mud)Document26 pagesVERNACULAR ARCHITECTURE (Mud)Ashina Gupta100% (1)
- Grey Alba Vs Dela CruzDocument4 pagesGrey Alba Vs Dela CruzJamie StevensNo ratings yet
- Outstanding-Performance-in-SOCIAL SCIENCE-1Document16 pagesOutstanding-Performance-in-SOCIAL SCIENCE-1Tyron Rex SolanoNo ratings yet
- Other Hands - Issue #15-16, Supplement PDFDocument8 pagesOther Hands - Issue #15-16, Supplement PDFAlHazredNo ratings yet
- S R S M: Arah Owell and Cott AckenzieDocument7 pagesS R S M: Arah Owell and Cott AckenzieEduardo MBNo ratings yet
- Chapter 4 SolutionsDocument4 pagesChapter 4 SolutionsSamantha ReedNo ratings yet
- Coraline QuotesDocument2 pagesCoraline Quotes145099No ratings yet
- Bounty Hunter CreationDocument3 pagesBounty Hunter CreationdocidleNo ratings yet
- Pre-Test - Pediatric NursingDocument6 pagesPre-Test - Pediatric NursingogiskuadzNo ratings yet
- Current Trends Issues and Problems in Education SystemDocument49 pagesCurrent Trends Issues and Problems in Education SystemfuellasjericNo ratings yet
- Supreme Court: Federico D. Ricafort For Petitioner. Eriberto D. Ignacio For RespondentDocument2 pagesSupreme Court: Federico D. Ricafort For Petitioner. Eriberto D. Ignacio For RespondentEspino EmmanuelNo ratings yet
- Online Writing SampleDocument2 pagesOnline Writing SampleSamson_Lam_9358No ratings yet
- Kenneth Alvis Pierce v. Ray H. Page, Warden, and The State of Oklahoma, 362 F.2d 534, 10th Cir. (1966)Document2 pagesKenneth Alvis Pierce v. Ray H. Page, Warden, and The State of Oklahoma, 362 F.2d 534, 10th Cir. (1966)Scribd Government DocsNo ratings yet
- Group Practice Agency AuthorizationDocument2 pagesGroup Practice Agency AuthorizationAurangzeb JadoonNo ratings yet
- Histtory and Importance of HadithDocument31 pagesHisttory and Importance of HadithAbdullah AhsanNo ratings yet
- 3310-Ch 10-End of Chapter solutions-STDocument30 pages3310-Ch 10-End of Chapter solutions-STArvind ManoNo ratings yet
- Gulf Times: HMC Providing State-Of-The-Art Treatment To All Covid-19 PatientsDocument20 pagesGulf Times: HMC Providing State-Of-The-Art Treatment To All Covid-19 PatientsmurphygtNo ratings yet
- Born Again of The People: Luis Taruc and Peasant Ideology in Philippine Revolutionary PoliticsDocument43 pagesBorn Again of The People: Luis Taruc and Peasant Ideology in Philippine Revolutionary PoliticsThania O. CoronicaNo ratings yet
- Blue Economy CourseDocument2 pagesBlue Economy CourseKenneth FrancisNo ratings yet
- Ancient History 12 - Daily Notes - (Sankalp (UPSC 2024) )Document16 pagesAncient History 12 - Daily Notes - (Sankalp (UPSC 2024) )nigamkumar2tbNo ratings yet