Download as pptx, pdf, or txt
You might also like
- Trigeminal Neuralgia. Diagnosis and Treatment. Allam AK, Sharma H, Larkin MB, Viswanathan ADocument15 pagesTrigeminal Neuralgia. Diagnosis and Treatment. Allam AK, Sharma H, Larkin MB, Viswanathan ANana ShkodinaNo ratings yet
- Ultimate Stretching GuideDocument18 pagesUltimate Stretching GuideJason Collingburn100% (11)
- Antiretroviral Drugs: DR - Vijay BhushanamDocument44 pagesAntiretroviral Drugs: DR - Vijay Bhushanamshree devNo ratings yet
- 38.ANTIRETROVIRALS PDFDocument5 pages38.ANTIRETROVIRALS PDFireneNo ratings yet
- Antiretroviral DrugsDocument60 pagesAntiretroviral DrugsDeribe BekeleNo ratings yet
- 9) AntiretroviralDocument79 pages9) AntiretroviralOkot ChristopherNo ratings yet
- Antiviral ChemotherapyDocument59 pagesAntiviral ChemotherapyDiriba feyisaNo ratings yet
- Hiv-Aids SSDocument22 pagesHiv-Aids SSAINo ratings yet
- Antiretroviral Presentation - LamivudineDocument14 pagesAntiretroviral Presentation - LamivudineTehreem KhanNo ratings yet
- Antiretroviral DrugsDocument26 pagesAntiretroviral DrugsAmit ShahNo ratings yet
- 29 Anti-Viral Drugs PDFDocument43 pages29 Anti-Viral Drugs PDFabhishek talokarNo ratings yet
- Art DrugsDocument70 pagesArt DrugsDr Daulat Ram DhakedNo ratings yet
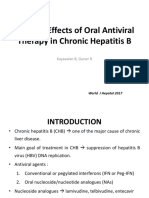
- Adverse Effects of Oral Antiviral Therapy in ChronicDocument12 pagesAdverse Effects of Oral Antiviral Therapy in ChronicAndi SusiloNo ratings yet
- Antiretrovirals Mechanisms of Action and Side Effects: Dr. Syed Faisal MahmoodDocument31 pagesAntiretrovirals Mechanisms of Action and Side Effects: Dr. Syed Faisal MahmoodAtif AliNo ratings yet
- Antiviral Agents: KatzungDocument62 pagesAntiviral Agents: KatzungDep SilvestreNo ratings yet
- Antiviral DrugsDocument75 pagesAntiviral DrugsluamsmarinsNo ratings yet
- HIV MedicineDocument32 pagesHIV Medicinechongocletus02No ratings yet
- PrepDocument36 pagesPrepsameralhameerNo ratings yet
- Antiretroviral Therapy (ART) : When, How To Start HAART and Combination TherapiesDocument36 pagesAntiretroviral Therapy (ART) : When, How To Start HAART and Combination TherapiesMwanja MosesNo ratings yet
- Ii. Antifungal Antiviral and Antiparasitic DrugsDocument73 pagesIi. Antifungal Antiviral and Antiparasitic DrugsMiguel Luis NavarreteNo ratings yet
- Hiv in PregnancyDocument98 pagesHiv in PregnancyAkrit DahalNo ratings yet
- CCC GRP 6Document61 pagesCCC GRP 6Stacy JumaNo ratings yet
- Antiviral Agents: Jason J. Schafer, Pharmd, MPH, BCPS, Aahivp Associate Professor, Jefferson College of PharmacyDocument73 pagesAntiviral Agents: Jason J. Schafer, Pharmd, MPH, BCPS, Aahivp Associate Professor, Jefferson College of PharmacyJeffrey LeeNo ratings yet
- 22-Antiviral Agents IIIDocument39 pages22-Antiviral Agents IIIShashidharan MenonNo ratings yet
- Antiviral Drugs-3Document72 pagesAntiviral Drugs-3charitykimberly3No ratings yet
- Lec 10 AntiviralsDocument26 pagesLec 10 AntiviralsAiqa QaziNo ratings yet
- Kuliah Farmakologi - Farmakokinetik Dan Farmakodinamik Antivirus Dan Antiparasit Secara UmumDocument87 pagesKuliah Farmakologi - Farmakokinetik Dan Farmakodinamik Antivirus Dan Antiparasit Secara UmumGabriel AnindhitaNo ratings yet
- Hiv in Pregnant WomenDocument33 pagesHiv in Pregnant WomenWill CheahNo ratings yet
- Hiv Treatment: IC2 Haemato-Lymphoid and Tropical Medicine HLTM Dr. Eoghan de Barra 2014Document55 pagesHiv Treatment: IC2 Haemato-Lymphoid and Tropical Medicine HLTM Dr. Eoghan de Barra 2014Faiq Syukri Bin SaparudinNo ratings yet
- 3 Anti Retroviral Drugs 2012Document29 pages3 Anti Retroviral Drugs 2012Youths With PurposesNo ratings yet
- W11 & W12 - Medication For Immune SystemDocument27 pagesW11 & W12 - Medication For Immune SystemAkari ChanNo ratings yet
- Antivirals - DR Arundhati AbhyankarDocument34 pagesAntivirals - DR Arundhati AbhyankarSiddhant BanwatNo ratings yet
- Hiv Hepc PresentationDocument16 pagesHiv Hepc Presentationapi-748224285No ratings yet
- Anti-Viral and Anti-Fungal AgentsDocument212 pagesAnti-Viral and Anti-Fungal Agentsmiguel cuevas100% (1)
- Aids UpdateDocument40 pagesAids UpdateipursNo ratings yet
- NCM 106 AntiviralDocument34 pagesNCM 106 AntiviralJod BellNo ratings yet
- Management of HIV/AIDS by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaDocument13 pagesManagement of HIV/AIDS by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaSreekrishnan TrikkurNo ratings yet
- Slide - K-27 - Farmakologi AntivirusDocument36 pagesSlide - K-27 - Farmakologi AntivirusFaisal AlhasNo ratings yet
- Antiviral Agents: Dr. Nutan RaoDocument18 pagesAntiviral Agents: Dr. Nutan RaoNutan Desai RaoNo ratings yet
- Anti+HIV DrugsDocument40 pagesAnti+HIV DrugsThao TrinhNo ratings yet
- Description of Antiviral DrugsDocument26 pagesDescription of Antiviral DrugsChristopher SongoroNo ratings yet
- AntiviralsDocument68 pagesAntiviralsapi-3839550No ratings yet
- Management of ART ComplicationsDocument88 pagesManagement of ART Complicationsangkatanjuli2019No ratings yet
- Antiviral AgentsDocument14 pagesAntiviral Agentsalishba100% (1)
- K45 - Antiviral Antifungi Anthelmentic Antiamoeba Antimalaria (FT)Document210 pagesK45 - Antiviral Antifungi Anthelmentic Antiamoeba Antimalaria (FT)Rizky Indah SorayaNo ratings yet
- Antiparasit AntifungiDocument63 pagesAntiparasit AntifungiMagfirah AlamNo ratings yet
- AntihepatitisDocument38 pagesAntihepatitismariamanoNo ratings yet
- Antivirals & AntifungalsDocument51 pagesAntivirals & AntifungalsanojNo ratings yet
- Chemotherapy - 2Document90 pagesChemotherapy - 2shNo ratings yet
- Human Immunodeficiency Virus (Hiv)Document30 pagesHuman Immunodeficiency Virus (Hiv)Manesa ManeshaNo ratings yet
- Antiviral TherapyDocument19 pagesAntiviral TherapyMalueth AnguiNo ratings yet
- Modes of TransmissionDocument5 pagesModes of TransmissionMaheen IdreesNo ratings yet
- Antivirals (AE, Drug-Drug Interactions)Document11 pagesAntivirals (AE, Drug-Drug Interactions)ShiraishiNo ratings yet
- Nnrtis: Nonnucleoside Reverse Trancriptase InhibitorsDocument12 pagesNnrtis: Nonnucleoside Reverse Trancriptase InhibitorsMalueth AnguiNo ratings yet
- Hiv & Persons Living With HIVDocument32 pagesHiv & Persons Living With HIVjericho dinglasanNo ratings yet
- Antiviral DrugsDocument44 pagesAntiviral DrugsMohammed WasimNo ratings yet
- Antiviral DrugsDocument44 pagesAntiviral DrugsMohammed WasimNo ratings yet
- Obat Antivirus HIVDocument16 pagesObat Antivirus HIVRasyidNo ratings yet
- Antiretroviral Drugs and The Importance of Adherence To The DrugsDocument20 pagesAntiretroviral Drugs and The Importance of Adherence To The DrugsSalihu MustaphaNo ratings yet
- 408 Antiviral Stu 07Document6 pages408 Antiviral Stu 07Hassan.shehriNo ratings yet
- Antiviral AgentsDocument133 pagesAntiviral AgentssyedtayyabrazazaidiNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- The Principles of The Surgical Management of Gastric CancerDocument5 pagesThe Principles of The Surgical Management of Gastric CancerRobert ChristevenNo ratings yet
- Patient Consent Form For ConsultationDocument1 pagePatient Consent Form For ConsultationKhristian Joshua G. JuradoNo ratings yet
- BIOETHICSDocument15 pagesBIOETHICSEvianne Jersey LofstedtNo ratings yet
- CMCSS Return To Work/School FlowchartDocument1 pageCMCSS Return To Work/School FlowchartFOX 17 NewsNo ratings yet
- Many Health Benefits of Fennel PDFDocument8 pagesMany Health Benefits of Fennel PDFAnonymous yE2LIYBNo ratings yet
- Drug Therapy in DermatologyDocument486 pagesDrug Therapy in Dermatologyfitra khoNo ratings yet
- Fresh Frozen Plasma Transfusion - Guideline For PracticeDocument16 pagesFresh Frozen Plasma Transfusion - Guideline For PracticeMohd Anas SheikhNo ratings yet
- Useful and Harmful Materials Part - 1 SciDocument31 pagesUseful and Harmful Materials Part - 1 SciKate OchaveNo ratings yet
- Abcede Davidson Discharge Summary Cic Pamana 1 - 1Document11 pagesAbcede Davidson Discharge Summary Cic Pamana 1 - 1iNo ratings yet
- Trans Aubf Lec3Document8 pagesTrans Aubf Lec3USLT- Angoluan, Andrei T.No ratings yet
- Pencegahan COVID-19 Melalui Pemberian Asuhan Keperawatan Komunitas DaringDocument10 pagesPencegahan COVID-19 Melalui Pemberian Asuhan Keperawatan Komunitas DaringDai Muhammad AbdiNo ratings yet
- Arterial Puncture: Claire Babcock O'ConnellDocument10 pagesArterial Puncture: Claire Babcock O'ConnellGerson Tocno LopezNo ratings yet
- MS2760 HiViral Mediu de Transport KitDocument2 pagesMS2760 HiViral Mediu de Transport KitLidia NarbNo ratings yet
- Baltimore County Resource Guide December 2023Document13 pagesBaltimore County Resource Guide December 2023api-516741446No ratings yet
- IFH Newsletter Q1 2022Document4 pagesIFH Newsletter Q1 2022Nicole SwenartonNo ratings yet
- Histiocyte Society LCH Treatment GuidelinesDocument21 pagesHistiocyte Society LCH Treatment GuidelinesAshok KumarNo ratings yet
- 星创降压神经锤套装Diagnostic Set Buck Neurological Hammer SetDocument4 pages星创降压神经锤套装Diagnostic Set Buck Neurological Hammer SetsintruemedicalNo ratings yet
- Pengaruh Kelebihan Berat Badan Ibu, Obesitas Dan Berat Badan Kehamilan Pada Hasil Perinatal Pada Wanita Dengan Diabetes MellitusDocument8 pagesPengaruh Kelebihan Berat Badan Ibu, Obesitas Dan Berat Badan Kehamilan Pada Hasil Perinatal Pada Wanita Dengan Diabetes Mellitusshabrina KdgNo ratings yet
- The Routes of Covid-19 Transmission: A Literature Review: Ati Surya Mediawati, Rachmat Susanto, Elly NurahmahDocument3 pagesThe Routes of Covid-19 Transmission: A Literature Review: Ati Surya Mediawati, Rachmat Susanto, Elly NurahmahChona Cari ReyesNo ratings yet
- Cognitive-Motor Exergaming For Reducing Fall Risk in People With Chronic Stroke: A Randomized Controlled TrialDocument18 pagesCognitive-Motor Exergaming For Reducing Fall Risk in People With Chronic Stroke: A Randomized Controlled TrialZilbran BerontaxNo ratings yet
- Nuclear CaseDocument106 pagesNuclear CaseAkramNo ratings yet
- Teachers Weekly Work Plan 1 March 22 262021Document9 pagesTeachers Weekly Work Plan 1 March 22 262021CHERRY ANN OLAJAYNo ratings yet
- Safety Management PlanDocument9 pagesSafety Management PlandhcastanoNo ratings yet
- Z-Alizadeh Sani DatasetDocument74 pagesZ-Alizadeh Sani DatasetROIHATUL JANNAHNo ratings yet
- UntitledDocument691 pagesUntitledTiago Santos Da SilvaNo ratings yet
- Esophageal Atresia: DR - Ibrahim AlsbouDocument21 pagesEsophageal Atresia: DR - Ibrahim Alsbouraed faisalNo ratings yet
- Indonesia. Vol. 28 (4) : 285 - 296. Pediatric. 18Document2 pagesIndonesia. Vol. 28 (4) : 285 - 296. Pediatric. 18Anonymous 4DnGXiBpRNo ratings yet
- Prof. Erlina Burhan - CVDocument18 pagesProf. Erlina Burhan - CVgmsmsuNo ratings yet