Download as pptx, pdf, or txt
You might also like
- HAP & VAP IDSA Pocketcard Guidelines (2016)Document12 pagesHAP & VAP IDSA Pocketcard Guidelines (2016)David GerickNo ratings yet
- Protozoal InfectionDocument66 pagesProtozoal InfectionGEM SCANNo ratings yet
- Malaria by Dr. A.M IyagbaDocument51 pagesMalaria by Dr. A.M IyagbaDr. Amb. Monday ZaccheausNo ratings yet
- Protozoa InfectionsDocument71 pagesProtozoa InfectionsfaithjoycelineNo ratings yet
- Collette MalariaDocument47 pagesCollette Malariacollinsmwila98No ratings yet
- Case 3.2 (Malaria) : Arwa Hussain Al-Onayzan. 215007943. 66Document24 pagesCase 3.2 (Malaria) : Arwa Hussain Al-Onayzan. 215007943. 66Danial HassanNo ratings yet
- Plasmodium SpeciesDocument61 pagesPlasmodium SpeciesSubhas KarnaNo ratings yet
- MalariaDocument62 pagesMalariaYousuf skNo ratings yet
- Parasitic Causes of HaematologyDocument65 pagesParasitic Causes of HaematologySolomonNo ratings yet
- Malaria, Typhus and RFDocument54 pagesMalaria, Typhus and RFLet MeflyNo ratings yet
- MalariaDocument60 pagesMalariaHSC UNITEDNo ratings yet
- Lecture 10 (Plasmodium) (F)Document59 pagesLecture 10 (Plasmodium) (F)jolan.freedomNo ratings yet
- Malaria MB CHB January 2018-FinalDocument36 pagesMalaria MB CHB January 2018-Finalokwadha simionNo ratings yet
- Diseases Caused by ProtozoaDocument47 pagesDiseases Caused by ProtozoaDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU PhilippinesNo ratings yet
- MalariaDocument49 pagesMalaria2253010837No ratings yet
- SESSION 16-Malaria and TrypanosomiasisDocument46 pagesSESSION 16-Malaria and Trypanosomiasisgbunyara100No ratings yet
- MalariaDocument16 pagesMalariachachamwangoNo ratings yet
- Malaria: DR Sulaiman Conteh Medical StudentsDocument36 pagesMalaria: DR Sulaiman Conteh Medical StudentsAbubakar JallohNo ratings yet
- E MalariaDocument40 pagesE MalariaUmair AliNo ratings yet
- MALARIA (Autosaved)Document16 pagesMALARIA (Autosaved)Mpanso Ahmad AlhijjNo ratings yet
- Malaria by Professor Motea Al-AwlaqiDocument23 pagesMalaria by Professor Motea Al-AwlaqiMotea AlawlaqiNo ratings yet
- One Day Workshop Yums: - Tissue and Blood Protozoan DiseasesDocument47 pagesOne Day Workshop Yums: - Tissue and Blood Protozoan DiseasesAndre KerenNo ratings yet
- Vector Borne - PPTX 1Document140 pagesVector Borne - PPTX 1Nursing septemberNo ratings yet
- Malaria Es PregcyDocument61 pagesMalaria Es PregcyNinaNo ratings yet
- Blood and Tissue ProtozoaDocument32 pagesBlood and Tissue ProtozoaFort SalvadorNo ratings yet
- Malaria 141112210953 Conversion Gate02Document33 pagesMalaria 141112210953 Conversion Gate02shubham vermaNo ratings yet
- Family Spirochaetaceae AND LeptospiraceaeDocument33 pagesFamily Spirochaetaceae AND Leptospiraceaeyosef awokeNo ratings yet
- Malaria: Prima Dewi Yuliani 1210312120 Widyatul Aina Alfioni ParsiskaDocument27 pagesMalaria: Prima Dewi Yuliani 1210312120 Widyatul Aina Alfioni ParsiskaAnonymous Di1zSIkRBHNo ratings yet
- Malaria: Department of Internal Medicine, School of MedicineDocument33 pagesMalaria: Department of Internal Medicine, School of MedicineAndarge ImperialNo ratings yet
- DR Anil Sabharwal MDDocument57 pagesDR Anil Sabharwal MDsaump3No ratings yet
- Malaria FalciparumDocument35 pagesMalaria FalciparumAboubakar Moalim Mahad moh'dNo ratings yet
- Malaria 1Document20 pagesMalaria 1Ankush GahlotNo ratings yet
- GROUP A1 (A) Topic 5Document37 pagesGROUP A1 (A) Topic 5KhaiNo ratings yet
- Anti Malarial DrugsDocument107 pagesAnti Malarial DrugsSindile MchunuNo ratings yet
- Malaria TropmedDocument47 pagesMalaria TropmedDickyNo ratings yet
- 2 MalariaDocument79 pages2 MalariaSabyashashi SaikiaNo ratings yet
- MalariaDocument34 pagesMalariaKidistNo ratings yet
- ANAPLASMOSISDocument19 pagesANAPLASMOSISAshfaq Ahmad KhanNo ratings yet
- MalariaDocument21 pagesMalariaRakshithNo ratings yet
- Practical Seminar1.13Document35 pagesPractical Seminar1.13chrisibinuNo ratings yet
- Nervous System Module (Parasitology)Document13 pagesNervous System Module (Parasitology)NAOGE GEDEFANo ratings yet
- Malaria/Hms: Dr. Muhammad Hamza (MB, BS, FMCP) Department of Medicine Akth/Buk KanoDocument47 pagesMalaria/Hms: Dr. Muhammad Hamza (MB, BS, FMCP) Department of Medicine Akth/Buk Kanoadamu mohammadNo ratings yet
- 40 MalariaDocument68 pages40 MalariaShiv SharmaNo ratings yet
- Acute Febrile IllnessesDocument96 pagesAcute Febrile IllnessesHAlid mohammed100% (1)
- Unit 11. Blood and Tissue Coccidian (Apicomplexa)Document40 pagesUnit 11. Blood and Tissue Coccidian (Apicomplexa)Michael DawitNo ratings yet
- Major Bacteria Infecting The Hematology System 2. Major Parasites Infecting The Hematologic SystemDocument128 pagesMajor Bacteria Infecting The Hematology System 2. Major Parasites Infecting The Hematologic SystemƯớc Của BếttingNo ratings yet
- Malaria: Prof Dr. Hj. Wan Omar Abdullah, JSMDocument35 pagesMalaria: Prof Dr. Hj. Wan Omar Abdullah, JSMMohd ZulhanafiNo ratings yet
- Major Bacteria Infecting The Hematology System 2. Major Parasites Infecting The Hematologic SystemDocument121 pagesMajor Bacteria Infecting The Hematology System 2. Major Parasites Infecting The Hematologic SystemƯớc Của BếttingNo ratings yet
- AnaplasmaDocument22 pagesAnaplasmaSomesh SharmaNo ratings yet
- Anti Malaria¡Document107 pagesAnti Malaria¡makioedesemiNo ratings yet
- Plasmodium: 25/02/2019 Ss NghoshiDocument31 pagesPlasmodium: 25/02/2019 Ss NghoshiJohanna HaludiluNo ratings yet
- Malaria - The MulasDocument46 pagesMalaria - The MulasRobinNo ratings yet
- Malaria. Mr.r.phiriDocument29 pagesMalaria. Mr.r.phiricheweblessings03No ratings yet
- Malaria PresentationDocument56 pagesMalaria PresentationMuhammad Shiddiq DwisuryaNo ratings yet
- Bone MarrowDocument72 pagesBone MarrowSumit PandyaNo ratings yet
- Malarial NephropathyDocument68 pagesMalarial Nephropathyhendra_darmawan_4No ratings yet
- Malaria ىواسكرك كرابم ةلئان .د دادعاDocument87 pagesMalaria ىواسكرك كرابم ةلئان .د دادعاkoncoerrorNo ratings yet
- MalariaDocument28 pagesMalariaAbdul AtaNo ratings yet
- Malaria Symptoms, ImmunityDocument29 pagesMalaria Symptoms, Immunity2022mls045No ratings yet
- Lepto Dan RabiesDocument69 pagesLepto Dan RabiesHiszom AsyhariNo ratings yet
- Cestodes: Prepared By: Charriz A. AmoyanDocument37 pagesCestodes: Prepared By: Charriz A. AmoyanAudrie Allyson GabalesNo ratings yet
- Name: Ikhtiara Fakhrunisa Class: X MIPA 5 Date: Wednesday, 26 Maret 2020 Text Report About InventionDocument2 pagesName: Ikhtiara Fakhrunisa Class: X MIPA 5 Date: Wednesday, 26 Maret 2020 Text Report About InventionIkhtiaraNo ratings yet
- Microsoft Word - Pneumonia Education EnglishDocument9 pagesMicrosoft Word - Pneumonia Education Englishjustin_saneNo ratings yet
- Veterinary Parasitology Questionbank - 1Document5 pagesVeterinary Parasitology Questionbank - 1VIJAYNo ratings yet
- (Impetigo) : Erbil Polythecnic University Soran Technical Insititute Nuraing Department First StageDocument14 pages(Impetigo) : Erbil Polythecnic University Soran Technical Insititute Nuraing Department First StageKubra ĖdrisNo ratings yet
- Sepsis and Pneumonia v1.3Document2 pagesSepsis and Pneumonia v1.3Luis HANo ratings yet
- Antiparasitic DrugsDocument51 pagesAntiparasitic Drugsmanik_ghadlinge100% (2)
- Mtap BB 1Document23 pagesMtap BB 1Jennie Grace MaloomNo ratings yet
- Importance Surveillance and DetectionDocument6 pagesImportance Surveillance and Detectionsherog ahmedNo ratings yet
- Ebola Virus Disease: A Review On Epidemiology, Symptoms, Treatment and PathogenesisDocument8 pagesEbola Virus Disease: A Review On Epidemiology, Symptoms, Treatment and PathogenesisAuliaZahraNo ratings yet
- Wound InfectionDocument30 pagesWound InfectionIbrahim SultanNo ratings yet
- Running Head: Current Bio-Terrorism Issues 1Document6 pagesRunning Head: Current Bio-Terrorism Issues 1api-400900026No ratings yet
- BIOS E-72: Infectious Diseases in A World of Changing Climate, Drug Resistance, and Vaccine HesitancyDocument3 pagesBIOS E-72: Infectious Diseases in A World of Changing Climate, Drug Resistance, and Vaccine HesitancyPK MK SocNo ratings yet
- Expanded Program On ImmunizationDocument6 pagesExpanded Program On ImmunizationAiza Oronce100% (1)
- Coombs TestDocument11 pagesCoombs Testtamer273No ratings yet
- Drug Resistant TB GuidelineDocument46 pagesDrug Resistant TB Guidelineameer abdullahNo ratings yet
- Requirements: For A Valid Vaccination Certificate (3 Doses)Document1 pageRequirements: For A Valid Vaccination Certificate (3 Doses)HaoYang ChiaNo ratings yet
- Lyme OverviewDocument87 pagesLyme OverviewAmanda MehallNo ratings yet
- 6 Human Diseases That Cause by VirusesDocument7 pages6 Human Diseases That Cause by VirusesJefry JapNo ratings yet
- Filaria - Final 4Document14 pagesFilaria - Final 4Arun Jv100% (1)
- Hand HygieneDocument42 pagesHand HygieneHamisi OmarNo ratings yet
- Wcms 117313Document105 pagesWcms 117313Hervis Francisco FantiniNo ratings yet
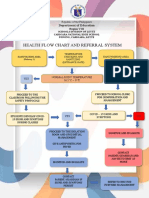
- Health Flow Chart and Referral System: Department of EducationDocument2 pagesHealth Flow Chart and Referral System: Department of EducationWendy TablaNo ratings yet
- Communicable DiseasesDocument12 pagesCommunicable Diseasesjustinejeon6No ratings yet
- HERPESVIRUSES, PARVO 2021 Students - KopieDocument38 pagesHERPESVIRUSES, PARVO 2021 Students - KopieMr.FantasthiccNo ratings yet
- Training Manual For Counselors PDFDocument197 pagesTraining Manual For Counselors PDFمخلص منيب اللهNo ratings yet
- Vaginal Discharge Flow ChartDocument1 pageVaginal Discharge Flow ChartHafizuddin RazidNo ratings yet
- Evaluation Form For GPBP Project Briefs (DOH) : Name of LGUDocument3 pagesEvaluation Form For GPBP Project Briefs (DOH) : Name of LGUMarius Clifford BilledoNo ratings yet
- CHN NCPDocument2 pagesCHN NCPIna Marie Calungcaguin Castro100% (1)