Download as pptx, pdf, or txt
You might also like
- Dwnload Full Essentials of Physical Anthropology 10th Edition Jurmain Solutions Manual PDFDocument35 pagesDwnload Full Essentials of Physical Anthropology 10th Edition Jurmain Solutions Manual PDFmollybrevet.9xj4b0100% (10)
- Cell WorksheetDocument12 pagesCell WorksheetNahed Safi100% (1)
- Curs Anatomie PatologicaDocument114 pagesCurs Anatomie PatologicaAndreea AignatoaieNo ratings yet
- Pathology of NoaDocument164 pagesPathology of NoaAnonymous milwFDXNo ratings yet
- Molecular Organization of The Plasma MembraneDocument53 pagesMolecular Organization of The Plasma MembraneJD100% (1)
- Cell DeathDocument42 pagesCell DeathAlexander Mensah SarpongNo ratings yet
- Cell Adaptation, Injury, and DeathDocument48 pagesCell Adaptation, Injury, and DeathRizka SukmasariNo ratings yet
- Cellular Adaptation - 2022Document49 pagesCellular Adaptation - 2022Leo Lucifer 104No ratings yet
- Pathology NotesDocument29 pagesPathology NotesMK100% (2)
- Pathology (3) Adaptation and Cellular DepostitionDocument50 pagesPathology (3) Adaptation and Cellular Depostitionnurul dwi ratihNo ratings yet
- Cellular Injury, Adaptation and Cellular DeathDocument72 pagesCellular Injury, Adaptation and Cellular DeathlawrencenandowNo ratings yet
- Cellular Injury, Adaptation and Cell DeathDocument8 pagesCellular Injury, Adaptation and Cell DeathJessica Febrina Wuisan100% (1)
- Cellular Injury, Adaptation and Cellular DeathDocument40 pagesCellular Injury, Adaptation and Cellular DeathSuleiman KikulweNo ratings yet
- Cellular Injury, Adaptation and Cellular DeathDocument40 pagesCellular Injury, Adaptation and Cellular DeathSuleiman KikulweNo ratings yet
- Cell Growth Patterns/Disorders of Growth: Prof - Abdul Jabbar N. Al-ShammariDocument52 pagesCell Growth Patterns/Disorders of Growth: Prof - Abdul Jabbar N. Al-Shammariمختبرات ابوسارةNo ratings yet
- 1 Cellular Response To Injury 1Document33 pages1 Cellular Response To Injury 1Alex XanderNo ratings yet
- Pathology Cell InjuryDocument57 pagesPathology Cell InjuryMajd MustafaNo ratings yet
- 6 CellularAdaptationsDocument87 pages6 CellularAdaptationsMaria MoiseencuNo ratings yet
- Lect 2 Patho SentDocument79 pagesLect 2 Patho SentPuranjay ChandelNo ratings yet
- Pathology: Yacob Alemu (MD) May 2021Document74 pagesPathology: Yacob Alemu (MD) May 2021Tazeb AyeleNo ratings yet
- Cell Injury and AdaptationDocument47 pagesCell Injury and AdaptationPujashree SabatNo ratings yet
- Cellular AdaptationDocument30 pagesCellular AdaptationTauqeer AhmedNo ratings yet
- Cellular Pathology: Normal CellsDocument20 pagesCellular Pathology: Normal CellsRHONENo ratings yet
- Section 1: Cellular AdaptationsDocument30 pagesSection 1: Cellular AdaptationsElena PoriazovaNo ratings yet
- Prof - Abdul Jabbar N. Al-ShammariDocument51 pagesProf - Abdul Jabbar N. Al-Shammariمختبرات ابوسارةNo ratings yet
- Introduction To Pathology 02Document66 pagesIntroduction To Pathology 02sunday danielNo ratings yet
- Pujasari - Adaptation, Injury, & Death of CellsDocument24 pagesPujasari - Adaptation, Injury, & Death of CellsEfa FathurohmiNo ratings yet
- Cellular Response To Stress & Toxic Insults: Adaptation, Injury & DeathDocument70 pagesCellular Response To Stress & Toxic Insults: Adaptation, Injury & DeathMila DamayantiNo ratings yet
- RH PATHO2022 - (Chapt 02 - Cell Injury, Death, Adaptations - A)Document9 pagesRH PATHO2022 - (Chapt 02 - Cell Injury, Death, Adaptations - A)Toka AlzoubiNo ratings yet
- Cellular Responses To Stress and Toxic Insults PDFDocument11 pagesCellular Responses To Stress and Toxic Insults PDFDental TutorNo ratings yet
- Adaptation of Cellular Growth & Differentiation: Presented By: Dr. Hrudi Sundar SahooDocument28 pagesAdaptation of Cellular Growth & Differentiation: Presented By: Dr. Hrudi Sundar SahooEdsel Ian S. FuentesNo ratings yet
- Apoptosis & Necrosis: Suad Omar NafiDocument46 pagesApoptosis & Necrosis: Suad Omar Nafisoad onafiNo ratings yet
- Draft Sooca Case 8 CarbuncleDocument41 pagesDraft Sooca Case 8 CarbuncleGabriela Grace SinagaNo ratings yet
- Introduction To Basic Pathology - 09.08.2023.ppt-1Document31 pagesIntroduction To Basic Pathology - 09.08.2023.ppt-1Abdur RaquibNo ratings yet
- Cell Adaptation Cell Injury: DR Ia. Ratih Wulansari Manuaba, SPPD-KR, M.Kes, FinasimDocument51 pagesCell Adaptation Cell Injury: DR Ia. Ratih Wulansari Manuaba, SPPD-KR, M.Kes, Finasimluh komang ari trisna jayantiNo ratings yet
- Cellular Pathology: Normal CellsDocument22 pagesCellular Pathology: Normal CellsPrakash PanthiNo ratings yet
- PATHOPHYSIOLOGYDocument27 pagesPATHOPHYSIOLOGYBhavya agarwalNo ratings yet
- (Gen Path) Case 4, Numbers 2 and 3Document1 page(Gen Path) Case 4, Numbers 2 and 3Faiki Disomangcop Disomangcop-KimNo ratings yet
- Cell injury Lecture 1Document46 pagesCell injury Lecture 1hiraalizafarNo ratings yet
- Cell Injury, Cell Death, and AdaptationsDocument81 pagesCell Injury, Cell Death, and AdaptationsDrSyeda RimaNo ratings yet
- Histopathology NotesDocument12 pagesHistopathology NotesLeandro Miguel TongolNo ratings yet
- Lecture 1Document14 pagesLecture 1Ansari FarhanNo ratings yet
- Section 1: Cellular AdaptationsDocument30 pagesSection 1: Cellular AdaptationsVirli AnaNo ratings yet
- Section 1: Cellular AdaptationsDocument30 pagesSection 1: Cellular AdaptationsAya KinugasaNo ratings yet
- Cell InjuryDocument29 pagesCell InjuryDrVnita VaishyaNo ratings yet
- CellularAdaptation Injury and Death - General OverviewDocument13 pagesCellularAdaptation Injury and Death - General OverviewlydNo ratings yet
- 2 Cell Injury, Adaptation, and Cell DeathDocument6 pages2 Cell Injury, Adaptation, and Cell DeathcedonuliNo ratings yet
- Robbin's SummariesDocument98 pagesRobbin's Summariesnopedontsuemeplease100% (1)
- Cellular Response To Stress and Noxious StimuliDocument31 pagesCellular Response To Stress and Noxious StimuliWinda Syahfitri HasibuanNo ratings yet
- 1 Cellular AdaptationDocument17 pages1 Cellular AdaptationReetu BaralNo ratings yet
- Section 1: Cellular AdaptationsDocument30 pagesSection 1: Cellular Adaptationshaddi awanNo ratings yet
- Cell InjuryDocument46 pagesCell Injuryeri_tariganNo ratings yet
- Cell Injury and AdaptationDocument18 pagesCell Injury and AdaptationNazneen ShawarNo ratings yet
- Cell Injury PathologyDocument40 pagesCell Injury Pathologysridhar100% (1)
- Cell Injury (Dr. Sriwidyani)Document75 pagesCell Injury (Dr. Sriwidyani)galuh dharmapatniNo ratings yet
- 1) Cell Injury BPT - 092731Document110 pages1) Cell Injury BPT - 092731Crystal GamingNo ratings yet
- Bab 1 Cellular Responses To Stress & Toxic InsultsDocument48 pagesBab 1 Cellular Responses To Stress & Toxic InsultsSiti AisyahNo ratings yet
- ETIOLOGY of Cell InjuryDocument77 pagesETIOLOGY of Cell InjurybesthachakrapaniNo ratings yet
- Chapter 2 Cell AdaptationsDocument71 pagesChapter 2 Cell AdaptationsMuhammad Masoom AkhtarNo ratings yet
- 3 Cellular Adaptation and DifferentiationDocument32 pages3 Cellular Adaptation and Differentiationvinoedhnaidu_rajagopalNo ratings yet
- Chapter 1Document51 pagesChapter 1aaajjjaaajjjaaajjjaaajjjaaajjjNo ratings yet
- AdaptationsDocument25 pagesAdaptationsshehranNo ratings yet
- Zoo Sem2 Endoplasmic ReticulumDocument7 pagesZoo Sem2 Endoplasmic ReticulumAnadi ChauhanNo ratings yet
- Biotech Reviewer PDFDocument31 pagesBiotech Reviewer PDFGerald LimNo ratings yet
- Hematology Slides Step 1 UsmleDocument1 pageHematology Slides Step 1 Usmlenreena aslamNo ratings yet
- Creatinine MetabolismDocument108 pagesCreatinine MetabolismLilia PopanuNo ratings yet
- 2017 Midterm Test Practice QuestionsDocument8 pages2017 Midterm Test Practice Questionsaboodh123No ratings yet
- PEG PreparationDocument22 pagesPEG PreparationAshish SinghNo ratings yet
- Difference Between Gram Positive and GramDocument3 pagesDifference Between Gram Positive and Grambaraa aburassNo ratings yet
- The Biochemical Basis of Neuropharmacology 8th EditionDocument513 pagesThe Biochemical Basis of Neuropharmacology 8th EditionNeuro Iztacala100% (1)
- Grade 4 Unit 3 Lesson 1 Plant & Animal Cells PDFDocument16 pagesGrade 4 Unit 3 Lesson 1 Plant & Animal Cells PDFDavid Jhonson BasnilloNo ratings yet
- B1.2 ProteinsDocument8 pagesB1.2 ProteinslittleianlauNo ratings yet
- B EchiosebDocument2 pagesB EchiosebPriscilla Rosalyna MaranathaNo ratings yet
- Chen Et Al. (2022) Crop Transformation TechnologiesDocument9 pagesChen Et Al. (2022) Crop Transformation TechnologiesFreddy Colmenarez-BetancourtNo ratings yet
- G3 Worksheet 6.1 & 6.2Document12 pagesG3 Worksheet 6.1 & 6.2Mani Kumaresan Janarthanavel (Scss)No ratings yet
- FGF21 Activates AMPK Signaling: Impact On Metabolic Regulation and The Aging ProcessDocument9 pagesFGF21 Activates AMPK Signaling: Impact On Metabolic Regulation and The Aging ProcessaginaNo ratings yet
- Ijms 20 01358Document24 pagesIjms 20 01358CHETAN SOMUNo ratings yet
- Cell Unit of Life 1 ST Lecture by Tarun SirDocument6 pagesCell Unit of Life 1 ST Lecture by Tarun SirNIHAR moryaNo ratings yet
- Cell MembraneDocument20 pagesCell MembraneSarahNo ratings yet
- Transes Anaphy BloodDocument5 pagesTranses Anaphy BloodPia LouiseNo ratings yet
- The Effect of Different Solution in Rhoeo Discolor CellsDocument2 pagesThe Effect of Different Solution in Rhoeo Discolor CellsNanda Hasna AmrinaNo ratings yet
- Autoimmune Diseases - MMSDocument37 pagesAutoimmune Diseases - MMSmulatumeleseNo ratings yet
- 03 Epithelium 2022Document78 pages03 Epithelium 2022AlkadafeNo ratings yet
- Plasmaproteins (PP)Document14 pagesPlasmaproteins (PP)Lok ReddyNo ratings yet
- DNA StructureDocument8 pagesDNA StructureKesithan AnandarashNo ratings yet
- Chapter 41 - Neural Signaling (Complete)Document20 pagesChapter 41 - Neural Signaling (Complete)Liana Glorian G. NavarroNo ratings yet
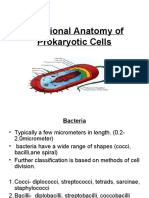
- Functional Anatomy of Prokaryotic CellsDocument28 pagesFunctional Anatomy of Prokaryotic CellsGabz GabbyNo ratings yet
- 5 6087101653624815826 PDFDocument3 pages5 6087101653624815826 PDFDijattx100% (1)
- Grade 10 - 4th Q - LAS 2Document4 pagesGrade 10 - 4th Q - LAS 2Lester Keno LejanoNo ratings yet