Download as pptx, pdf, or txt
You might also like
- Aramco Evaluation QuestionsDocument21 pagesAramco Evaluation QuestionsKunal Singh100% (11)
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Terror Infinity Vol 1Document63 pagesTerror Infinity Vol 1Azlan RabanNo ratings yet
- Reading Exercise 1Document4 pagesReading Exercise 1JumahirNo ratings yet
- Radiologi Decomp. CordisDocument25 pagesRadiologi Decomp. CordisHanifah RahmaniaNo ratings yet
- Cardiomegaly, CCF, Pulmonary EdemaDocument20 pagesCardiomegaly, CCF, Pulmonary EdemarajhiniNo ratings yet
- Radiograph Examination On Drowning Case: Debora BravianaDocument7 pagesRadiograph Examination On Drowning Case: Debora BravianaDeborah Bravian TairasNo ratings yet
- Interpretation of Chest Imaging1Document91 pagesInterpretation of Chest Imaging1Brooke TurnerNo ratings yet
- Cor PulmonaleDocument42 pagesCor PulmonaleNym Angga SantosaNo ratings yet
- Week 6 Disturbances in CirculationDocument83 pagesWeek 6 Disturbances in CirculationHans CortezNo ratings yet
- Kuliah 16 Cor PulmonaleDocument41 pagesKuliah 16 Cor PulmonalecaturwiraNo ratings yet
- Cardiovascular Pathology FINALDocument45 pagesCardiovascular Pathology FINALIanNo ratings yet
- Chest XDocument8 pagesChest XAnnandra RahmanNo ratings yet
- Congenital Heart Disease: MashuriDocument31 pagesCongenital Heart Disease: MashuriAlvienz SaputraNo ratings yet
- Cor Pulmonal and CHDDocument44 pagesCor Pulmonal and CHDamir iksanNo ratings yet
- BF - PJB - Yaf Mel Tia NiaDocument20 pagesBF - PJB - Yaf Mel Tia NiaRoberto HutapeaNo ratings yet
- Tetralogy of FallotDocument18 pagesTetralogy of FallotAaronMaroonFive100% (1)
- Cardiac TamponadeDocument43 pagesCardiac TamponadeMădălina GreereNo ratings yet
- Disturbances in The Pulmonary CirculationDocument13 pagesDisturbances in The Pulmonary CirculationironNo ratings yet
- Pathophysiology Congenital Heart Disease-1Document54 pagesPathophysiology Congenital Heart Disease-1single_ladyNo ratings yet
- Basic Chest Imaging and Heart FailureDocument57 pagesBasic Chest Imaging and Heart FailureKiaa auliaNo ratings yet
- Basics of Chest RadiographyDocument103 pagesBasics of Chest RadiographyEzekiel ArtetaNo ratings yet
- Basic Interpretation of CXRDocument84 pagesBasic Interpretation of CXRAbdiqani Mohamed AdanNo ratings yet
- Stage I - RedistributionDocument4 pagesStage I - RedistributionDenise DianeNo ratings yet
- Recognizing A Pleural EffusionDocument27 pagesRecognizing A Pleural EffusionLanny Dwi ChandraNo ratings yet
- Pulmonary Edema: Prepared By: South West Education CommitteeDocument65 pagesPulmonary Edema: Prepared By: South West Education CommitteedanradulescuNo ratings yet
- 3 - Valvular Heart DiseasesDocument43 pages3 - Valvular Heart DiseasesHamzehNo ratings yet
- Basicinterpretationofcxr 110913060449 Phpapp01Document84 pagesBasicinterpretationofcxr 110913060449 Phpapp01Alexandra DîrțuNo ratings yet
- Interpretasi Foto DadaDocument137 pagesInterpretasi Foto DadaRofi Irman100% (1)
- Pulmonary CirculationDocument43 pagesPulmonary CirculationbhaktiNo ratings yet
- CHD ApproachDocument140 pagesCHD ApproachauNo ratings yet
- Echocardiography: Pericardial Effusions & Cardiactamponade: David M. Whitaker, MDDocument43 pagesEchocardiography: Pericardial Effusions & Cardiactamponade: David M. Whitaker, MDusfcardsNo ratings yet
- Pulmonary EmbolismDocument5 pagesPulmonary EmbolismKian Justin HidalgoNo ratings yet
- Wk7 PLP Cardiovascular Disorder Part 1,2,3,4Document210 pagesWk7 PLP Cardiovascular Disorder Part 1,2,3,4claire yowsNo ratings yet
- Chest Radiology PG 2Document109 pagesChest Radiology PG 2rumanameman107No ratings yet
- Pulmo HPNDocument36 pagesPulmo HPNAlexander Santiago ParelNo ratings yet
- Cong - Heart DefectsDocument50 pagesCong - Heart DefectsMayuri SharmaNo ratings yet
- Breathing & CirculationDocument40 pagesBreathing & CirculationRia UtamiNo ratings yet
- Acute Pulmonary ThromboembolismDocument37 pagesAcute Pulmonary ThromboembolismОльга КоваленкоNo ratings yet
- MR Radiologi 28 JuniDocument20 pagesMR Radiologi 28 JuninanasafietriNo ratings yet
- Mechanisms of InjuryDocument19 pagesMechanisms of InjurydeklearNo ratings yet
- PH ReportDocument40 pagesPH ReportAlexander Santiago ParelNo ratings yet
- X-Rays of ChestDocument20 pagesX-Rays of Chesttahirreshi80No ratings yet
- 22 Ventricular Septal DefectDocument26 pages22 Ventricular Septal Defectdhiraj parmarNo ratings yet
- EMERGENCYmedical Imaging Respiratory SystemDocument69 pagesEMERGENCYmedical Imaging Respiratory SystemAndrei CealanNo ratings yet
- X Thorax BeoordelenDocument135 pagesX Thorax BeoordelenmtescasuraNo ratings yet
- Differential Diagnosis of Pleural Effusion-82892Document56 pagesDifferential Diagnosis of Pleural Effusion-82892Salih AslaNo ratings yet
- PedsnotesDocument18 pagesPedsnoteskp13oyNo ratings yet
- Interstitial Vs AlveolarDocument17 pagesInterstitial Vs AlveolarEdwin DarmawanNo ratings yet
- Acyanotic Heart Disease& Fetal Circulation: Guided By, Dr.K.Sivakanthan Consultant PaediatricianDocument98 pagesAcyanotic Heart Disease& Fetal Circulation: Guided By, Dr.K.Sivakanthan Consultant PaediatricianVijayakanth VijayakumarNo ratings yet
- LME SelfDocument5 pagesLME SelfJM Mizraime Gallo Dela-peñaNo ratings yet
- Pleural PathologiesDocument49 pagesPleural PathologiesIsaac ShirimaNo ratings yet
- Pleural EffusionDocument13 pagesPleural EffusionAbdirahman Ali YabarNo ratings yet
- Pleural EffusionDocument72 pagesPleural Effusionmaeliszxc kimNo ratings yet
- Pulmonary Embolus (PE)Document3 pagesPulmonary Embolus (PE)Heidi M FischerNo ratings yet
- Hanan Fathy Pediatric Nephrology UnitDocument59 pagesHanan Fathy Pediatric Nephrology UnitdrhananfathyNo ratings yet
- Surgical Conditions of Pleura: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonDocument63 pagesSurgical Conditions of Pleura: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonVincent SerNo ratings yet
- CXR, CT, MriDocument125 pagesCXR, CT, MrimevunimNo ratings yet
- 16 57 1 Total Anomalous Pulmonary Venous Connection IDocument38 pages16 57 1 Total Anomalous Pulmonary Venous Connection Iwiyay34652ceoshubcomNo ratings yet
- Congestive Heart FailureDocument11 pagesCongestive Heart Failurepvs5155No ratings yet
- CSL CXRDocument21 pagesCSL CXRBrandonRyanF.MosidinNo ratings yet
- Pulmonary EdemaDocument20 pagesPulmonary EdemaMohmmad Lateef GanieNo ratings yet
- Congestive Cardiac FailureDocument61 pagesCongestive Cardiac FailureYAMINIPRIYANNo ratings yet
- Happiness - Mark MansonDocument26 pagesHappiness - Mark MansonJake100% (3)
- Graphs: Presented By, M.Sangeetha, Ap/Cse, Kongu Engineering CollegeDocument61 pagesGraphs: Presented By, M.Sangeetha, Ap/Cse, Kongu Engineering CollegesangeethaNo ratings yet
- Modest Barbie Style Perfecting The PantyDocument4 pagesModest Barbie Style Perfecting The PantyapfelkraftNo ratings yet
- Intel System Management Specification - Rev2p0Document63 pagesIntel System Management Specification - Rev2p0Nisarg UpadhyayNo ratings yet
- Hagendoorn, I. Dance, Aesthetics and The BrainDocument471 pagesHagendoorn, I. Dance, Aesthetics and The Brainbboyindio217No ratings yet
- Executive Summary: Project TitleDocument57 pagesExecutive Summary: Project Titlenabajit1989No ratings yet
- Hematopoiesis, Including Lymphocyte Development and MaturationDocument2 pagesHematopoiesis, Including Lymphocyte Development and MaturationMuhammad FakhrizalNo ratings yet
- Tarot and Oracle List 2022Document2 pagesTarot and Oracle List 2022Rachel Abad-FabeNo ratings yet
- High Altitude Aeronautical Platform Systems (Presentation)Document30 pagesHigh Altitude Aeronautical Platform Systems (Presentation)Mahenoor SiddiquiNo ratings yet
- Eros and Psyche Print 2 PDFDocument8 pagesEros and Psyche Print 2 PDFNizzy Hope Nulada CartagoNo ratings yet
- c08 - Pending 8.36Document262 pagesc08 - Pending 8.36SeungMin LeeNo ratings yet
- Assignment 1 2 PumpDocument2 pagesAssignment 1 2 PumpAnkit0% (1)
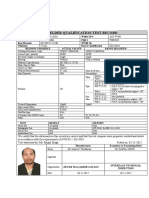
- Wqt-1-13-W-1-3g-Smaw-Alclad-Aws D1.1Document1 pageWqt-1-13-W-1-3g-Smaw-Alclad-Aws D1.1Rejoy babyNo ratings yet
- CKD NCPDocument4 pagesCKD NCPArlene Macatangay100% (1)
- 03 Vision 2020 The Right To SightDocument9 pages03 Vision 2020 The Right To SightMwanja MosesNo ratings yet
- Project Proposal TemplateDocument3 pagesProject Proposal TemplateNimrah KhanNo ratings yet
- Chapter 3 - HypothyroidismDocument59 pagesChapter 3 - HypothyroidismSteffi AraujoNo ratings yet
- Rash Driving Detection SystemDocument5 pagesRash Driving Detection SystemIJSTE100% (1)
- LPMDL 110x User Guide EN 4.9.6Document33 pagesLPMDL 110x User Guide EN 4.9.6Nikolay MilovanovNo ratings yet
- 6G Press ReleaseDocument2 pages6G Press Release6G Wellhead LLCNo ratings yet
- M45913-1 RevADocument4 pagesM45913-1 RevAMAI_QualityNo ratings yet
- PPT01-Introduction To Big DataDocument34 pagesPPT01-Introduction To Big DataTsabitAlaykRidhollahNo ratings yet
- Prevention of Foodborne Disease: The Five Keys To Safer FoodDocument2 pagesPrevention of Foodborne Disease: The Five Keys To Safer FoodZubda ButtNo ratings yet
- Doc-20240210-Wa0005 240508 203425Document110 pagesDoc-20240210-Wa0005 240508 203425cristina silvaNo ratings yet
- Checklist AS-Tronic / AS - MidDocument5 pagesChecklist AS-Tronic / AS - MidBroCactusNo ratings yet
- SCI10 Q3 M8 Adaptation and Ecological StabilityDocument18 pagesSCI10 Q3 M8 Adaptation and Ecological StabilityDoreen Lorraine ZabaleNo ratings yet
- Model-Based Strategic PlanningDocument18 pagesModel-Based Strategic PlanningBintang ramadhanNo ratings yet